The author performed a microsurgical cervical combined transpedicular lateral and medical procedure with partial pediculotomy (CTPP) in 78 patients (51 men and 27 women) with cervical foraminal stenosis to decompress the affected nerve root. 21 Patients (27%) had multilevel foraminal stenosis (2 - 4 levels). The goal of this surgery was to guarantee satisfactory exploration, to obtain a sufficient decompression of the intervertebral foramen, to maintain the integrity of the pedicle joint structures, and to avoid secondary cervical segmental instability. Neurological impairment, employment, and severity of associated signs were assessed preoperatively and at a 1-year, at a 3-year, and at a 5-years postoperative average follow-up (Mean 5.2 years, range, 3 to 18 years postoperatively). Diminution or complete disappearance of radicular symptoms was observed in 68 cases (87%), 1 year to 5 years after surgery, Minimal neurological deficits persisted in 10 cases (13%), and Neck pain improved in 73 cases, remained unchanged in 3, and progressed in two cases with severe preoperative deficits. Fifty-five patients (70.5%) returned to their previous occupation; only seven (9%) retired prematurely on the basis of disc disease alone. Based on Prolo's functional economic outcome rating scale (adapted by Davis for cervical spine), 69 patients (88.5%) showed excellent economic outcome. CTPP is an efficient means of decompressing lateral and medial spinal roots compromised by soft disk herniations or osteopbytic spurs, without the risk of an anterior approach with or without fusion. The CTPP showed also very good results in Cases with multilevel cervical foraminal stenosis (27%). Careful patient selection and microsurgical technique are essential in obtaining consistent, excellent results. Additionally, the recent trend toward minimally invasive techniques and key-hole operations in neurosurgery and other specialisations favours this minimally invasive procedure of CTPP.
Pediculotomy, Cervical radiculopathy, Cervical foraminotomy, Outcome
CTPP: Cervical transpedicular lateral and medial approach with partial pediculotomy; CR: Cervical radiculopathy;
CT: Computerized tomography; MRI: Magnetic resonance tomography; PJ: Pedicle joint
Since the first descriptions of posterior cervical foraminotomy by Scoville and Fryckholm [1,2], this procedure was extensively used firstly for managing cervical disc disease, Later, the technique was increasingly replaced by the anterior cervical approach with or without fusion (Cloward [3] and Robinson/Smith technique [4]), There is almost unanimous consensus on the advantages of the anterior approach in medial soft disc herniations and spondylotic spur removal [5]. Treatment of lateral soft and hard discs by the anterior or posterior approaches remains, however, controversial.
In a high number of Patients, complete resection of soft-disc fragments and osteophytes cannot be performed medially without excessive retraction on the nerve root and venous plexus, which may exacerbate the preexisting radiculopathy or increase intraoperative blood loss, obscuring the surgical field [6,7].
Avoiding this constellation and complication, a combined approach with medial partial resection of the pedicle joint (PJ) and partial resection of the superolateral portion of the PJ, leaving the most important part for the stability of the PJ (pars interarticularis, Figure 1) intact was developed (the CTPP), which allows for easier and more complete excision of the compressive lesion and, additionally, enlarges the neural foramen and provides a more complete decompression even in cases with multilevel CR, in which discectomy is not performed.
Seventy-eight patients with intraforaminal cervical soft or hard disc disease treated by CTPP between 1994 and 2019 were analysed retrospectively, including 51 men and 27 women with a mean age of 46.7 years at the time of surgery.
Thirty-five patients (45%) were classified as heavy workers (farmers, etc.) and 23 (29%) as light workers (office workers. Invalidity or disablement pensioners), the remaining 17 patients (22%) with nonsedentary occupation (including housewives with or without jobs outside the home) were classified as medium workers. Results were derived from questionnaire responses supplemented by office visits. All patients were asked to judge their recovery and describe residual difficulties in weakness, numbness, or pain in the neck, arms, or hands and other complications.
Fifty-seven patients (73%) presented with a single-level monoradiculopathy, 21 patients (27%) with 2 or more multilevel-radiculopathy.
The main measure of success of the operation was the visual analogue scale (VAS) for pain grading in combination with the Prolo functional economic outcome rating scale.
An x-ray film is obtained to verify the correct position of the incision. The PJ and the adjacent superior and inferior laminae are exposed by making a Para median incision. Using an operating microscope and a high-speed drill, the superolateral portion of the PJ joint and the upper and lateral margin of the interarticular part (pars interarticularis) were drilled away. The amount of PJ resection should not exceed 30%. Afterward, the intertransverse ligament is excised to expose the nerve root lateral to the foramen. The affected nerve root is then followed along the neuroforamen. Decompression of the medial part of the foramen is then completed using the standard interlaminar approach (according to a technique described previously [8]). Sufficient nerve root decompression must be carefully confirmed using a small dissector (Figure 1). This may be done by moving the hook from the medial and lateral sides through the foramen and then laterally. In using this combined approach, we were also able to reach and decompress two nerve roots, if necessary.
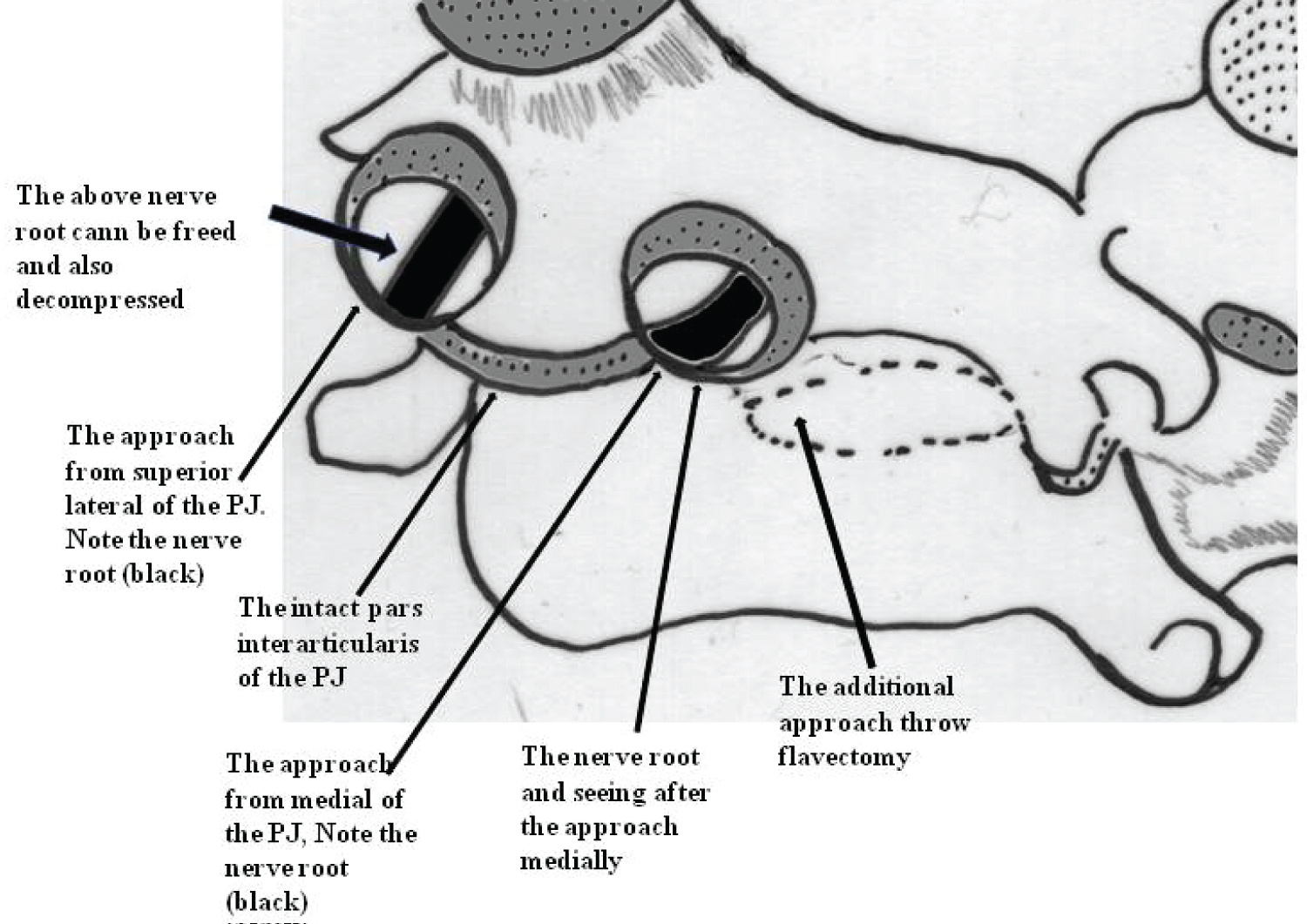 Figure 1: A schematic drawing of the operative field of the cervical transpedicular lateral and medial approach with partial pediculotomy medially and superolaterally. Note the intact pars articularis (most important part of PJ for the segmental stability). Additional partial hemilaminectomy with flavectomy may be necessary to decompress the nerve root medially.
View Figure 1
Figure 1: A schematic drawing of the operative field of the cervical transpedicular lateral and medial approach with partial pediculotomy medially and superolaterally. Note the intact pars articularis (most important part of PJ for the segmental stability). Additional partial hemilaminectomy with flavectomy may be necessary to decompress the nerve root medially.
View Figure 1
The superior nerve root is decompressed by removing the superolateral portion of the PJ and upper and lateral margin of the pars interarticularis, and the inferior nerve root is decompressed by removing the medial part of the PJ and part of the lamina.
Seventy-eight patients with one- or multi-level radiculopathy secondary to lumbar foraminal stenosis and refractory to conservative treatment underwent surgery between 1994 and 2019. These 78 procedures represented approximately 8% (78 of 970) of all cervical spinal surgeries performed during that period. Patients with medial disc herniation were excluded from the study. The patient population consisted of 51 men and 27 women. The most common nerve roots involved were the C-7 nerve root (51 patients, 65%), the C-6 nerve root (11 patients, 14%), the C-8 nerve root (16 patients, 20.5%). 21 patients (27%) hat multilevel foraminal stenosis (2-4 Levels simultaneously). The mean age was 46.7 years at the time of surgery.
Thirty-five patients (45%) were classified as heavy workers (farmers, etc.) and 23 (29%) as light workers (office workers. Invalidity or disablement pensioners), the remaining 17 patients (22%) with nonsedentary occupation (including housewives with or without jobs outside the home) were classified as medium workers. Results were derived from questionnaire responses supplemented by office visits. All patients were asked to judge their recovery and describe residual difficulties in weakness, numbness, or pain in the neck, arms, or hands and other complications.
Outcome was defined as excellent (no pain), good (some neck pain), fair (moderate radiculopathy), and poor (unchanged or worse) based on the Macnab classification [9]. The results were excellent in 63 patients, good in 11, and fair in 4. There were no surgery-related complications. Lateral cervical flexion-extension radiography was performed in all patients at various times ranging from 3 to 48 months after the surgery, and no evidence of postoperative segmental instability was found. Based on Prolo's functional economic outcome rating scale [10], which was adapted by Davis for the cervical spine [11], 59 patients (76%) showed excellent economic functional outcome (score 5 in both economic and functional social outcome). 11 patients (14%) had score 3 in economic and functional social outcome, and 8 patients had score 2 in economic outcome but 3 in functional social outcome (Table 1).
Table 1: The prolo functional and economic outcome rating scale [10] modified by Davis for postoperative cervical radiculopathy [11]. View Table 1
There is almost unanimous consensus on the advantages of the anterior approach in medial soft disc herniations and spondylotic spur removal [5,6]. Treatment of lateral soft and hard discs by the anterior or posterior approaches remains, however, controversial.
In a high number of Patients, complete resection of soft-disc fragments and osteophytes cannot be performed medially without excessive retraction on the nerve root and venous plexus, which may exacerbate the preexisting radiculopathy or increase intraoperative blood loss [6,7].
Avoiding this constellation and complication, a combined approach with medial partial resection of the pedicle joint (PJ) and partial resection of the superolateral portion of the PJ, leaving the most important part for the stability of the PJ (pars interarticularis, Figure 1) intact was developed (the CTPP), which allows for easier and more complete excision of the compressive lesion and, additionally, enlarges the neural foramen and provides a more complete decompression even in cases with multilevel CR, in which discectomy is not performed.
By using the CTPP procedure, the most important portion of the PJ for the segmental stability, the pars articularis remains intact. Although PJ destruction will not produce acute instability, it will transfer the loads to the adjacent disc and conceivably accelerate its degeneration. The procedure described here allows for preservation of the main portion of the PJ and provides good access to and visual control of the nerve root (or two nerve roots, if necessary), as well as the lateral and the medial part of the intervertebral foramen, with minimal risk of nerve root injury because of the improved visualization. The superior nerve root is decompressed by removing the superolateral portion of the PJ and the superolateral margin of the interarticularis, and the inferior nerve root is decompressed by removing the medial part of the PJ and part of the lamina. The preservation of a functional PJ reduces the possibility of postoperative instability. The clinical results of this procedure were excellent in the majority of cases.
The procedure described in this paper is safe and minimally invasive, providing excellent visualization of the lateral spinal structures. Because only minimal bone resection is required, the risk of secondary instability due to complete pediculotomy is avoided.