Adem is an autoimmune disease that can happen after any kind of inflammation and infection [1]. This disease is highly progressive and occurs in the central nervous system [2]. This disease commonly affects children. And in general, it is part of very uncommon diseases [3]. This disease affects more males than females [4]. In most cases, ADEM is associated with or caused by a viral disease or bacteria. This disease is caused in some cases after vaccination [5]. The exact pathogenesis of ADEM has not yet been fully elucidated. The proposed mechanism of ADEM is that myelin autoantigens share antigenicity with infectious pathogens [6]. Adem can appear with symptoms such as headache, nausea, vomiting, convulsions, and imbalance. A definite diagnostic method for ADEM is not yet known and it is diagnosed by MRI findings and exclusion of other diagnoses [7].
The patient is a 2-year-old child who referred to the pediatric emergency room due to loss of consciousness and suspected seizure symptoms. Also, the child's COVID-PCR test was reported positive 12 days before the visit, and the child had symptoms of cough and mild fever at the same time, which recovered at the same time. At the time of visit, the child was sleepy. He opened his eyes with painful stimulation and moved his right limbs less. Pupils were mid-sized, reactive and symmetrical. In the following examinations, there was no deviation in the eyes. Gag and corneal reflexes were normal. The child had spontaneous breathing and blood pressure and heart rate were normal. In the continuation of the history of the child, intolerance to food and milk was also mentioned. The initial blood sugar of the child was normal. After performing the initial measures, due to the unavailability of MRI, the child was subjected to brain CT scan. In the initial CT scan, the large size of the cerebral ventricles and hydrocephalus were mentioned for the child (Figure 1, Figure 2, Figure 3, Figure 4, Figure 5 and Figure 6). Due to hydrocephalus and clinical signs of increased ICP, the child was urgently transferred to the operating room, and while measuring ICP and sending a CSF sample, a ventriculoperitoneal shunt was implanted for the child. The child's icp was measured at 32 cmH2O. After the surgery, the child's level of consciousness improved relatively. The variables of the CSF sample sent were all in the normal range. The next day, the child underwent brain MRI and MRA. In the performed MRI, a clear signal change was seen in the frontal and occipital lobes, which is shown in photos No. 2, 3, 4, 5 and 6. According to the MRI, a biopsy was taken from the child's right frontal lobe for a definitive diagnosis. Immunohistochemical examination revealed the demyelinating nature of the specimen, in which extensive infiltration of basal macrophages and activated microglial cells was seen, while axons were largely preserved. No sign of vasculitis was seen in the examination of the sample. In this way, the result of the examination of the brain sample confirmed ADEM. With this diagnosis, the child was treated with corticosteroids and IVIG. The disease responded dramatically to the treatment. All the child's symptoms improved within two days and the child's level of consciousness reached its normal range. Finally, the child was discharged from the hospital after a week with a good general condition.
 Figure 1: Axial computed tomography image showing hydrocephalus.
View Figure 1
Figure 1: Axial computed tomography image showing hydrocephalus.
View Figure 1
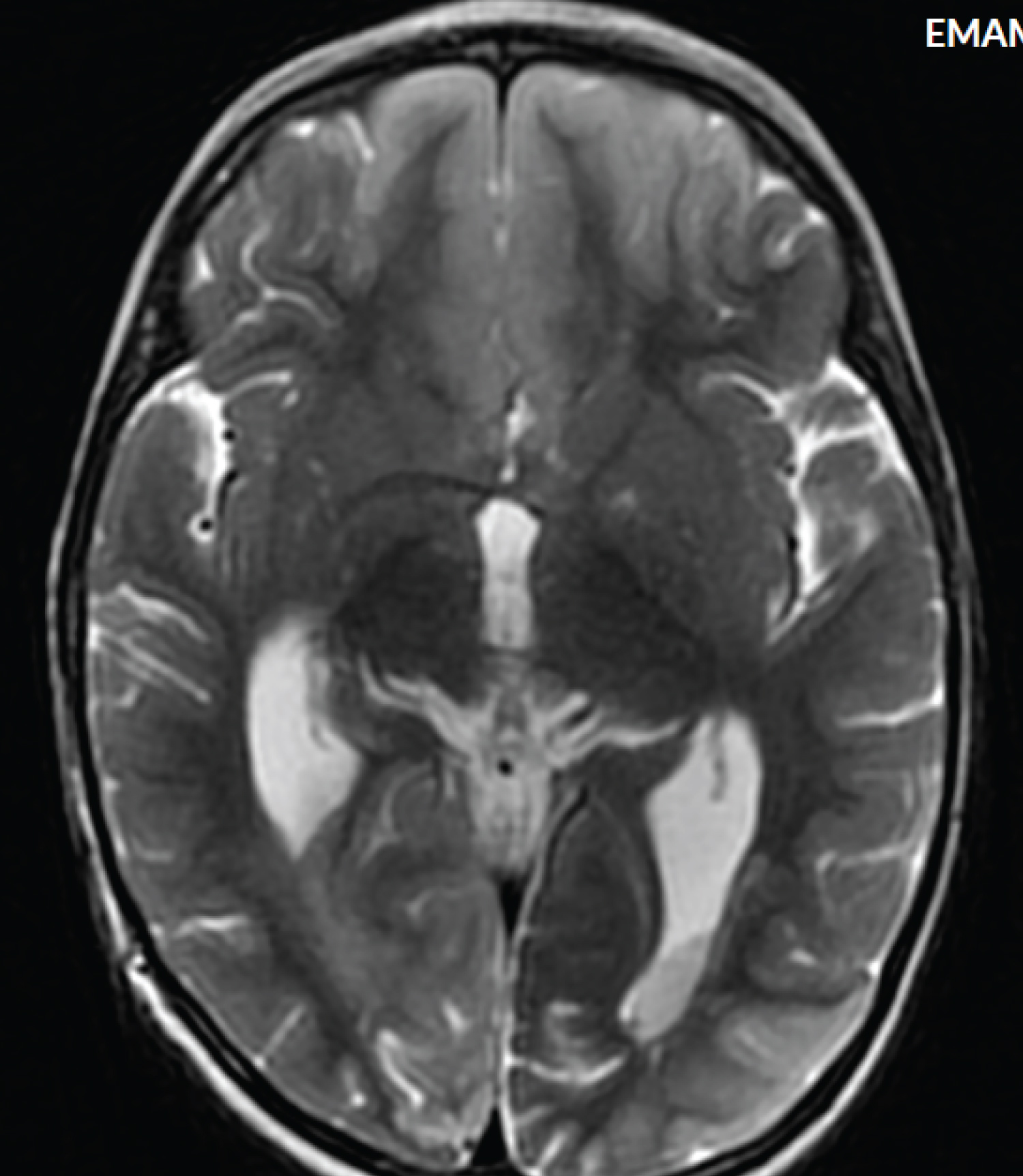 Figure 2: T2 weighted MR image shows signal changes in the frontal and occipital lobes.
View Figure 2
Figure 2: T2 weighted MR image shows signal changes in the frontal and occipital lobes.
View Figure 2
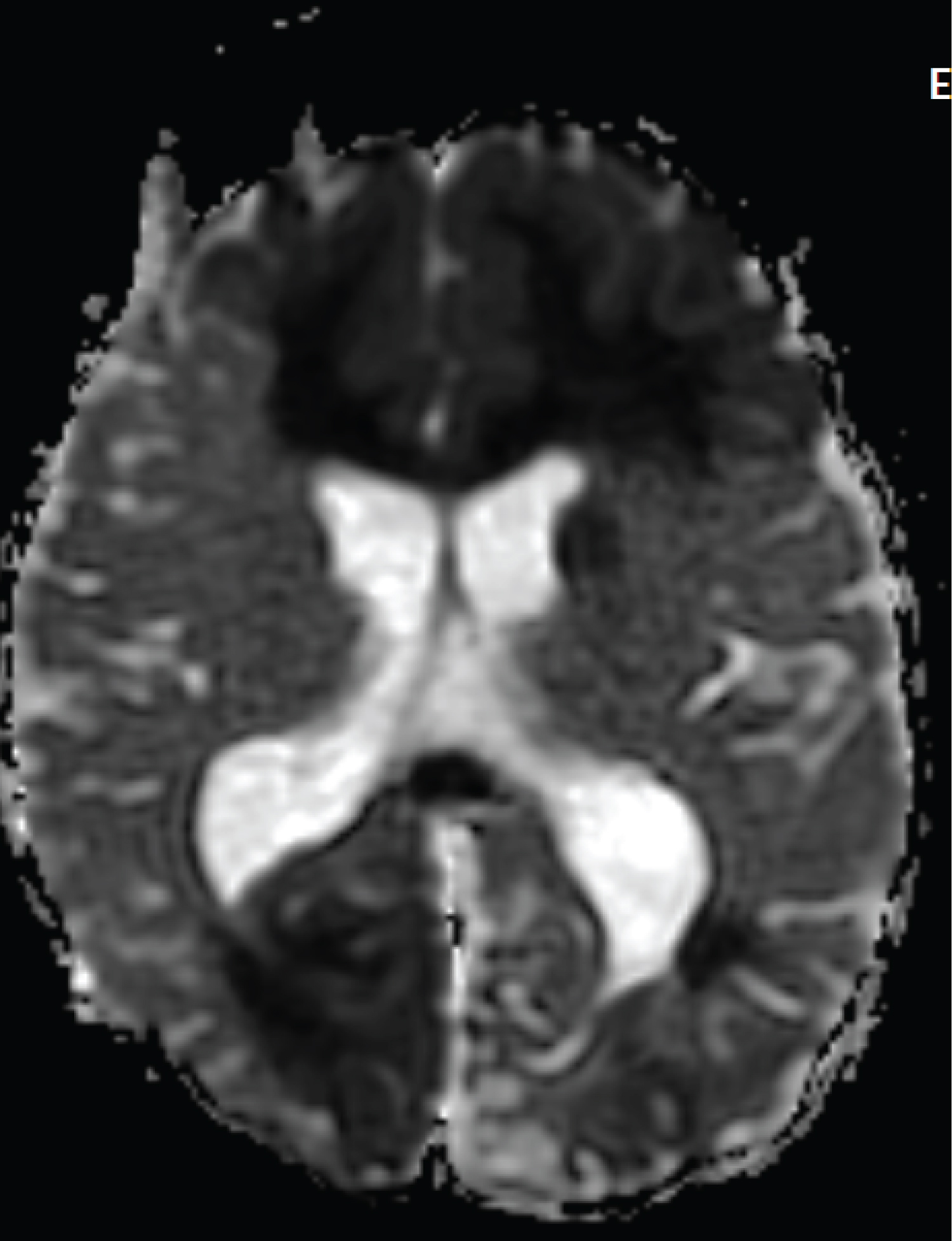 Figure 3: ADC image shows signal changes in the frontal and occipital lobes.
View Figure 3
Figure 3: ADC image shows signal changes in the frontal and occipital lobes.
View Figure 3
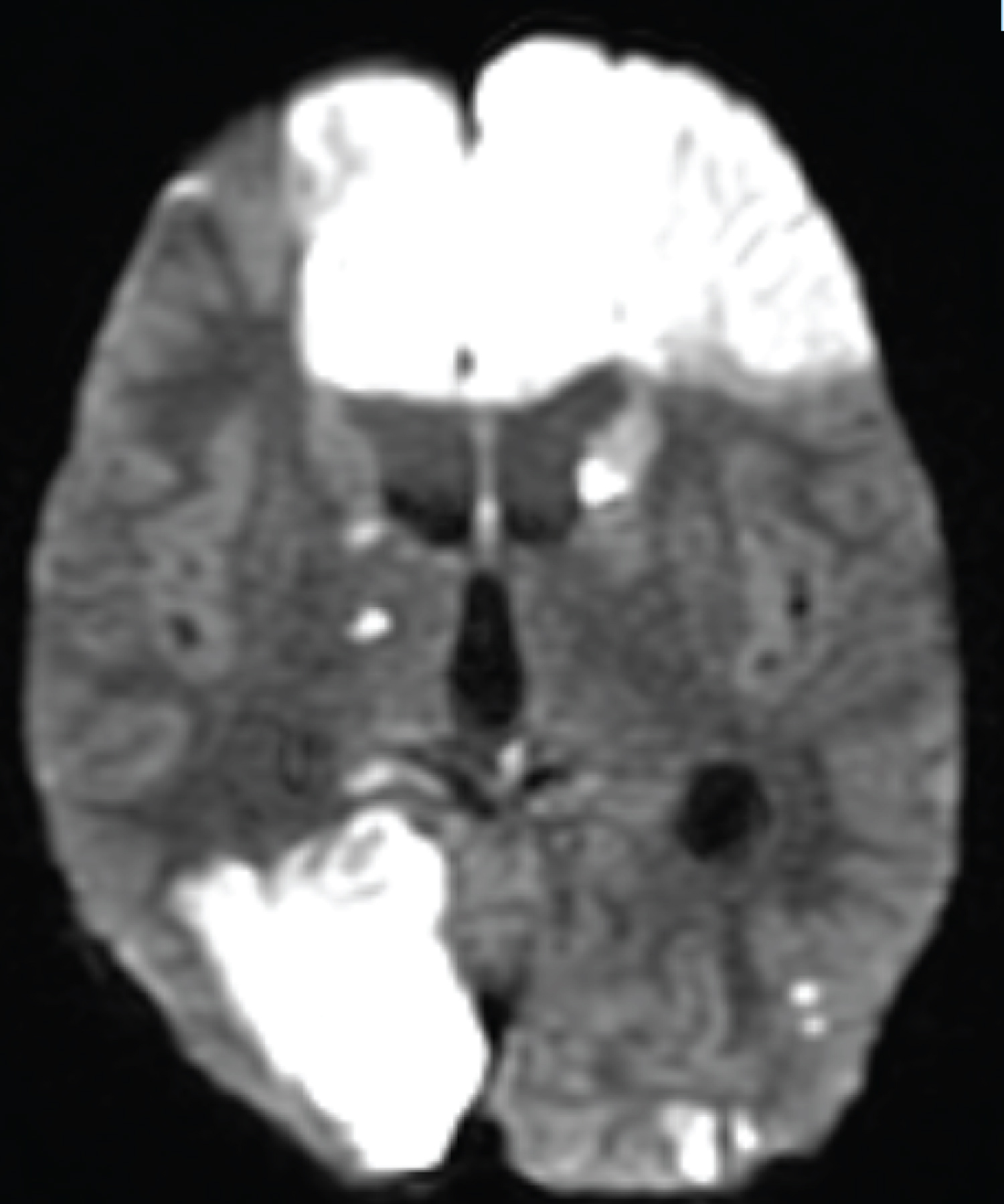 Figure 4: DWI image shows signal changes in the frontal and occipital lobes.
View Figure 4
Figure 4: DWI image shows signal changes in the frontal and occipital lobes.
View Figure 4
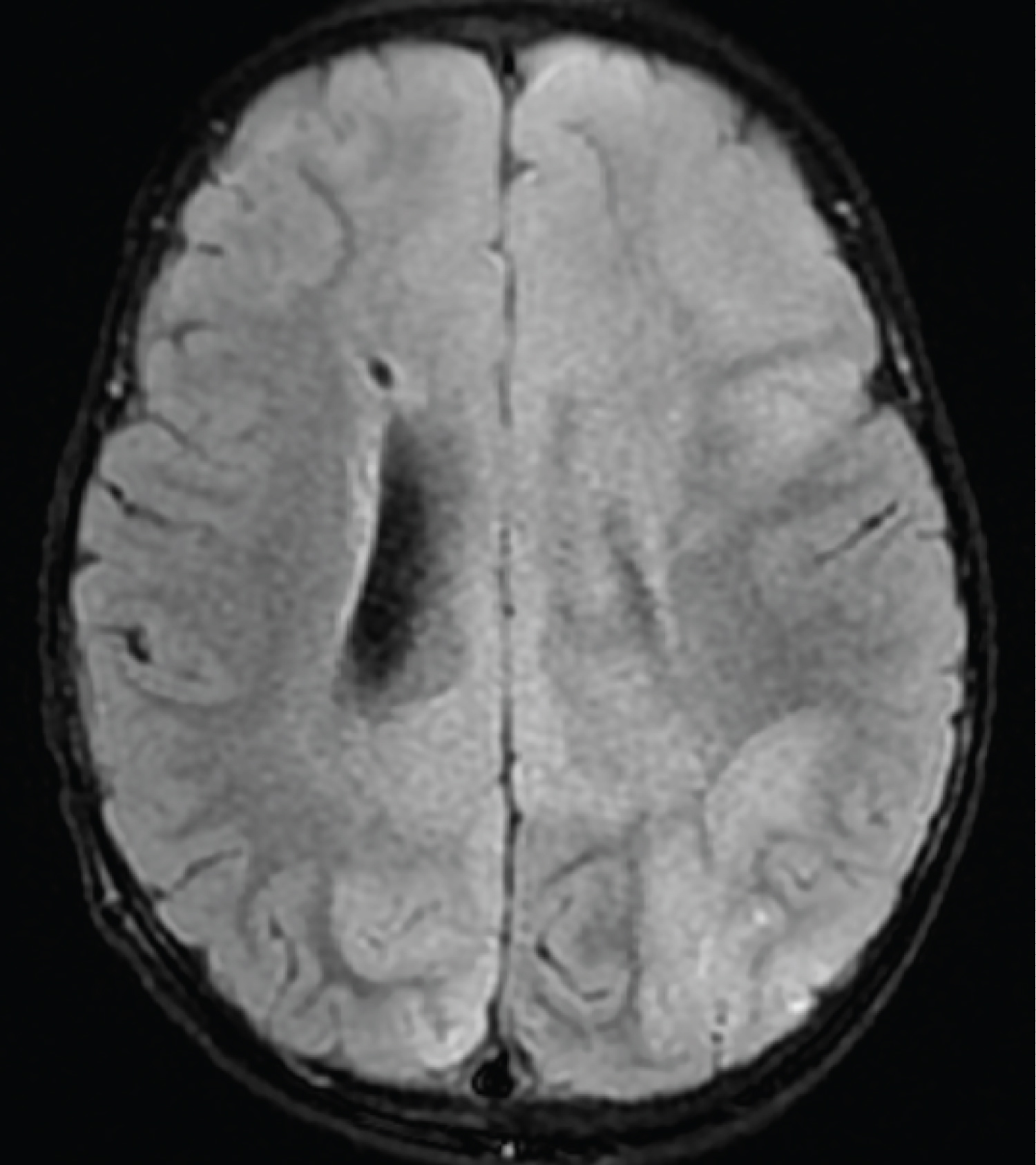 Figure 5: Flair image shows signal changes in the frontal and occipital lobes.
View Figure 5
Figure 5: Flair image shows signal changes in the frontal and occipital lobes.
View Figure 5
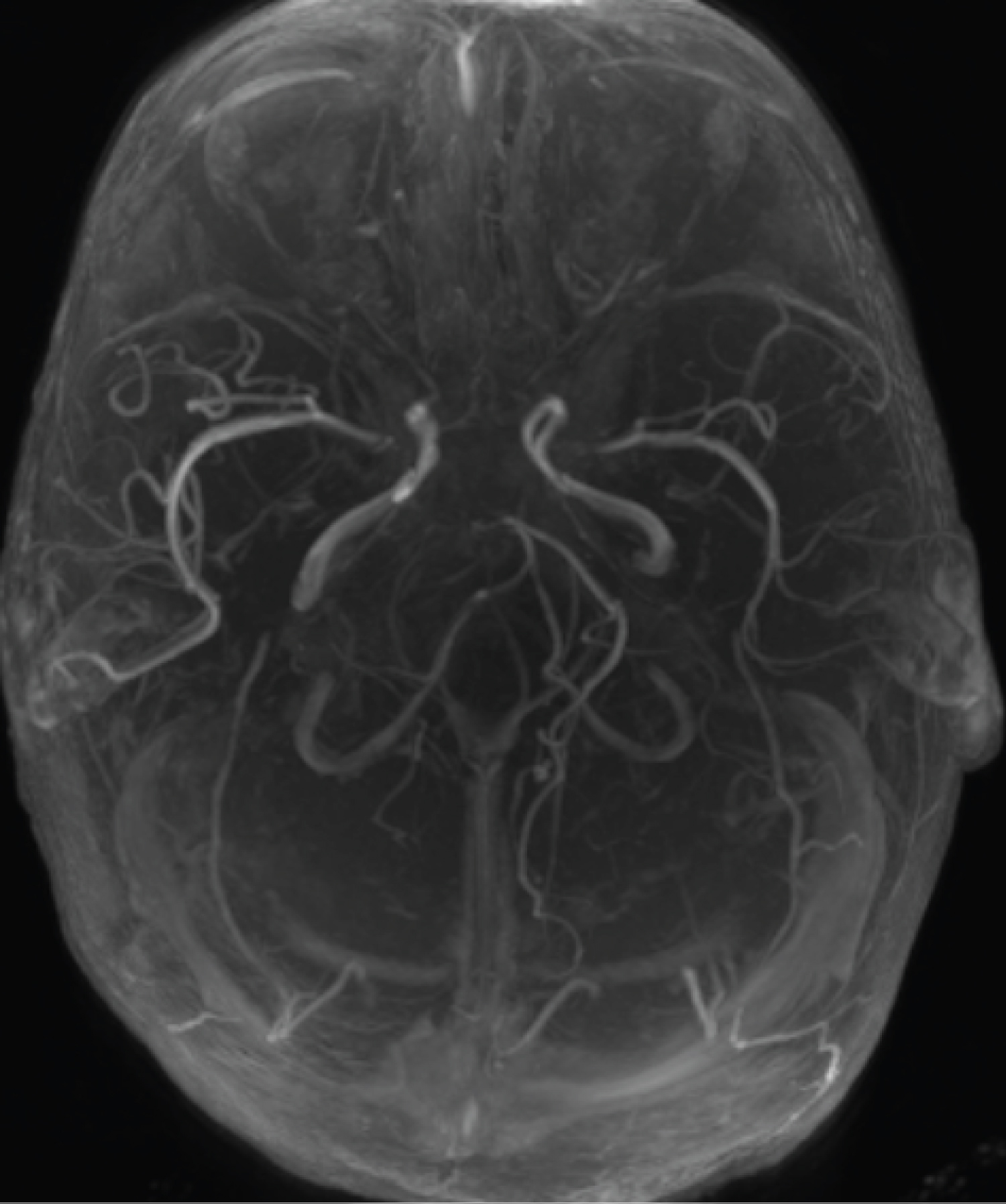 Figure 6: MRA showing normal vascularity.
View Figure 6
Figure 6: MRA showing normal vascularity.
View Figure 6
Covid-19 commonly occurs with respiratory and gastrointestinal symptoms, but this virus has shown over the past few years that it can also dangerously involve the CNS [8]. Due to the uncommon occurrence of symptoms of CNS involvement in patients with COVID-19, in most cases these symptoms are not noticed by doctors. But the presented case shows the high importance of examining issues related to CNS involvement in patients with COVID19. Considering the overall low prevalence of ADEM, its association with Covid-19 is very important. Considering the overall low prevalence of ADEM disease and its treatability, and on the other hand, its association with Covid-19, which has a very high prevalence, is very important.
This case shows the need to investigate CNS involvement in people with COVID-19. And considering the spread of Covid-19, it is likely that the incidence of ADEM will also increase, which leads to the need for more extensive studies.