Fahr's disease is named after the German neurologist Karl Theodor Fahr, who first reported it in 1930. This is a rare neurological condition characterized by abnormal idiopathic calcification of the basal ganglia and is usually inherited in autosomal dominant manner. These calcifications are consisted of calcium carbonate and phosphate, and may also occur in some other locations, such as thalamus, hippocampus, dentate nucleus, cerebral cortex, and cerebellar subcortical white matter [1]. Patients with Fahr's Disease generally misdiagnosed as subarachnoid hemorrhage at emergency services' admissions. In this paper we are reporting a case of Fahr's syndrome, which enlisted as a rare cause of intracranial calcification that may present like many nervous system diseases, who admitted to emergency service with headache found to be a subarachnoid hemorrhage due to an aneurysmal bleeding.
Fahr disease, Intracerebral calcification, Intracranial aneurysm, Subarachnoid hemorrhage
Fahr's disease is named after the German neurologist Karl Theodor Fahr, who first reported it in 1930. This is a rare neurological condition characterized by abnormal idiopathic calcification of the basal ganglia and is usually inherited in autosomal dominant manner. These calcifications are consisted of calcium carbonate and phosphate, and may also occur in some other locations, such as thalamus, hippocampus, dentate nucleus, cerebral cortex, and cerebellar subcortical white matter [1]. Etiology remains to be elucidated. Aneurysm with Fahr's disease in a case reported very rarely in literature. Fahr's Disease may inheredited in autosomal dominant or familial or sporadically. A genetic defect occurred in the short arm of chromosome 14 is thought to be responsible for Fahr's Disease [2]. Clinical hallmarks of the disease include Parkinsonism-like extrapyramidal symptoms, cognitive impairment, psychosis, seizures, and chronic headache-like findings [3].
Case here presented applied to the emergency service with the complaint of headache. Computed Tomography (CT) of head showed calcification at the basal ganglia and cerebellar cortex and subarachnoid hemorrhage. Digital subtraction angiography (DSA) revealed right middle cerebral artery aneurysm. The aneurysm was treated with endovascular intervention and external ventricular drainage was performedfor treatment of hydrocephalus. Patient recovered without any sequelae after the treatment. The patient reported here is the fifth in the literature showing aneurysm and Fahr's disease association.
27-year-old female patient who was brought to the Emergency Department of our hospital with the complaints of severe headache and vomiting. Her general condition was moderate, she was conscious, disorientated, and cooperative. Pupils were isochoric, bilateral light reflex was positive, and there was no lateralized motor deficit. Glasgow Coma Score was evaluated as 14 points. Blood pressure was measured to be 130/80 mmHg, pulse was 90/min, respiratory rate was 14/min, and fever measured 36 centigrade degrees. Head CT reported as hyperdense appearance compatible with intraventricular hematoma in both lateral ventricles and at the level of 3rd and 4th ventricle (Figure 1). Disseminated subarachnoid hemorrhage and additionally widespread calcification across bilateral basal ganglia, thalamus, and subcorticalwhite matter detected. Patient first taken to the OR to place an external ventricular drainage (EVD) catheter (Figure 2). Then DSA performed which revealed saccular aneurysmatic filling with 5*3 millimeters in diameter at the apex of the right Internal Carotid Artery just before theM1 segment of Middle Cerebral Artery. Endovascular coil placement was performed for aneurysm treatment (Figure 3). Then patient was taken to the neurosurgery intensive care unit for post-operative (PO) close follow-up. On the PO-5th day, she was taken to the in-patient floor due to wellness in her general condition. Control angiography showed successful closure of the aneurysm (Figure 4). Patient followed up three days with EVD closed as the clarification of the color of the cerebrospinal fluid in the catheter and resorption of the intraventricular hemorrhage in the control tomography observed (Figure 5). As no changes seen in the clinical status EVD catheter removed and patient discharged to home on the PO-12th day.
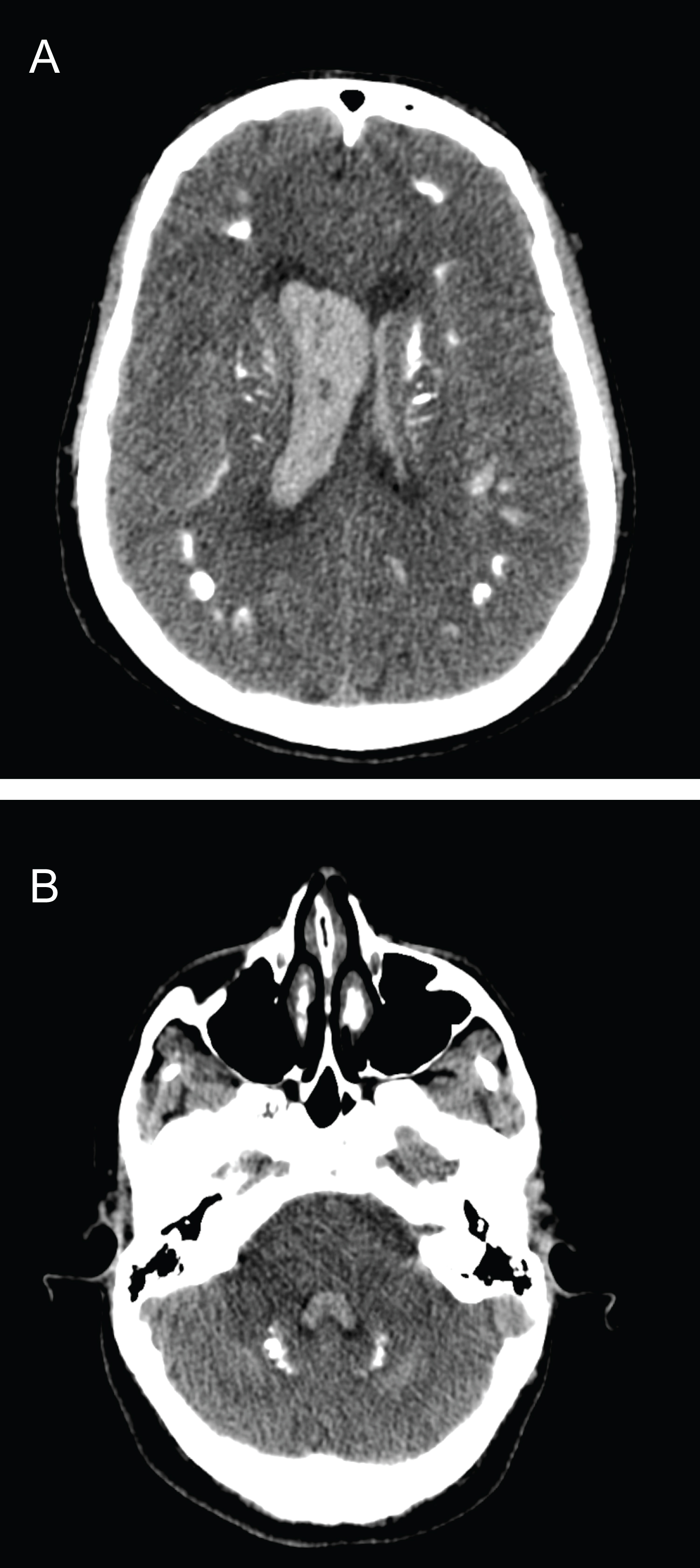 Figure 1: In the brain tomography of the patient who applied to the emergency department with the complaint of headache, there is a hyperdense appearance compatible with intraventricular hematoma in both lateral ventricles and at the level of the 3rd and 4th ventricles.
View Figure 1
Figure 1: In the brain tomography of the patient who applied to the emergency department with the complaint of headache, there is a hyperdense appearance compatible with intraventricular hematoma in both lateral ventricles and at the level of the 3rd and 4th ventricles.
View Figure 1
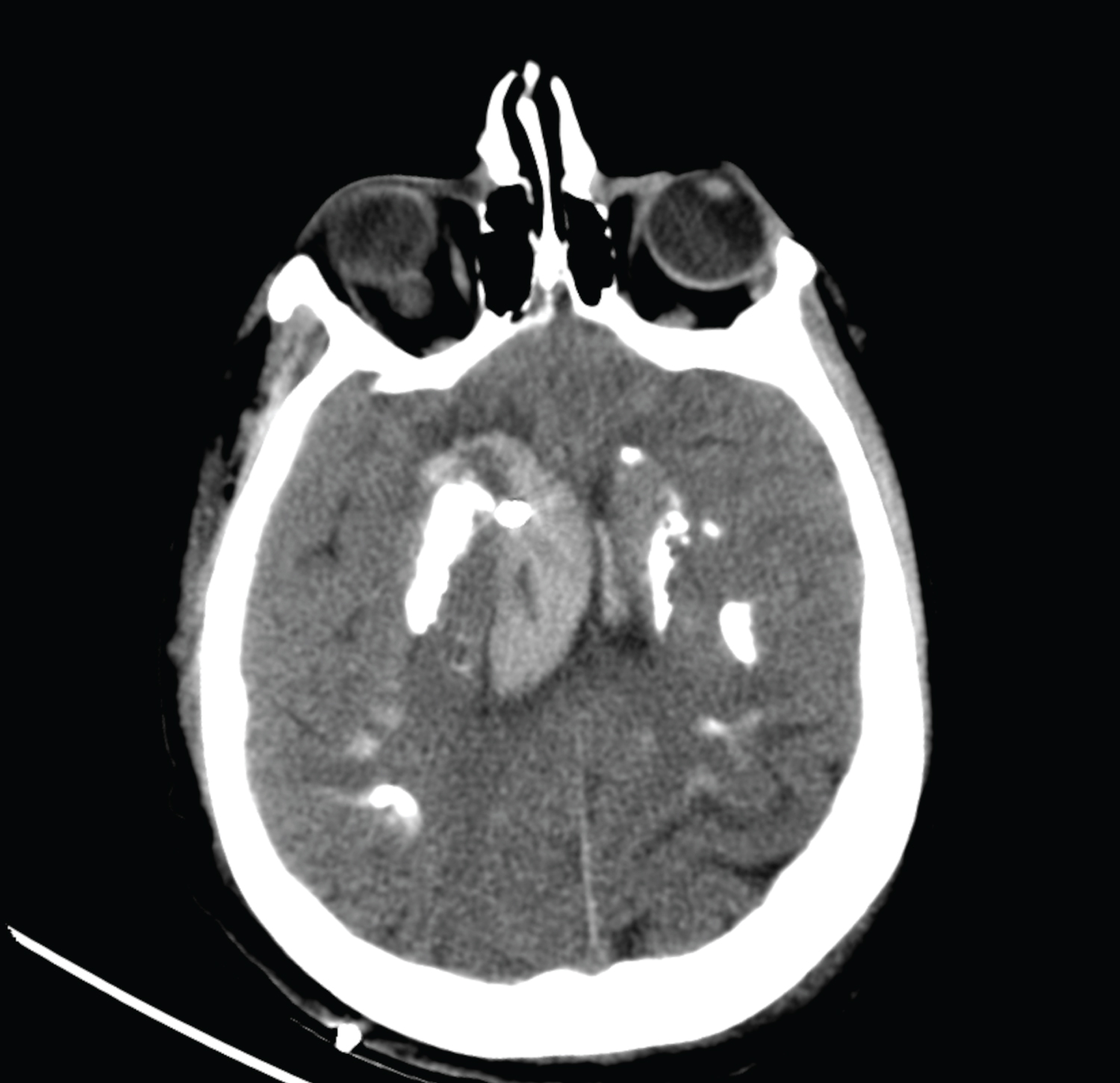 Figure 2: Control brain tomography after external ventricular drainage for drainage of existing bleeding.
View Figure 2
Figure 2: Control brain tomography after external ventricular drainage for drainage of existing bleeding.
View Figure 2
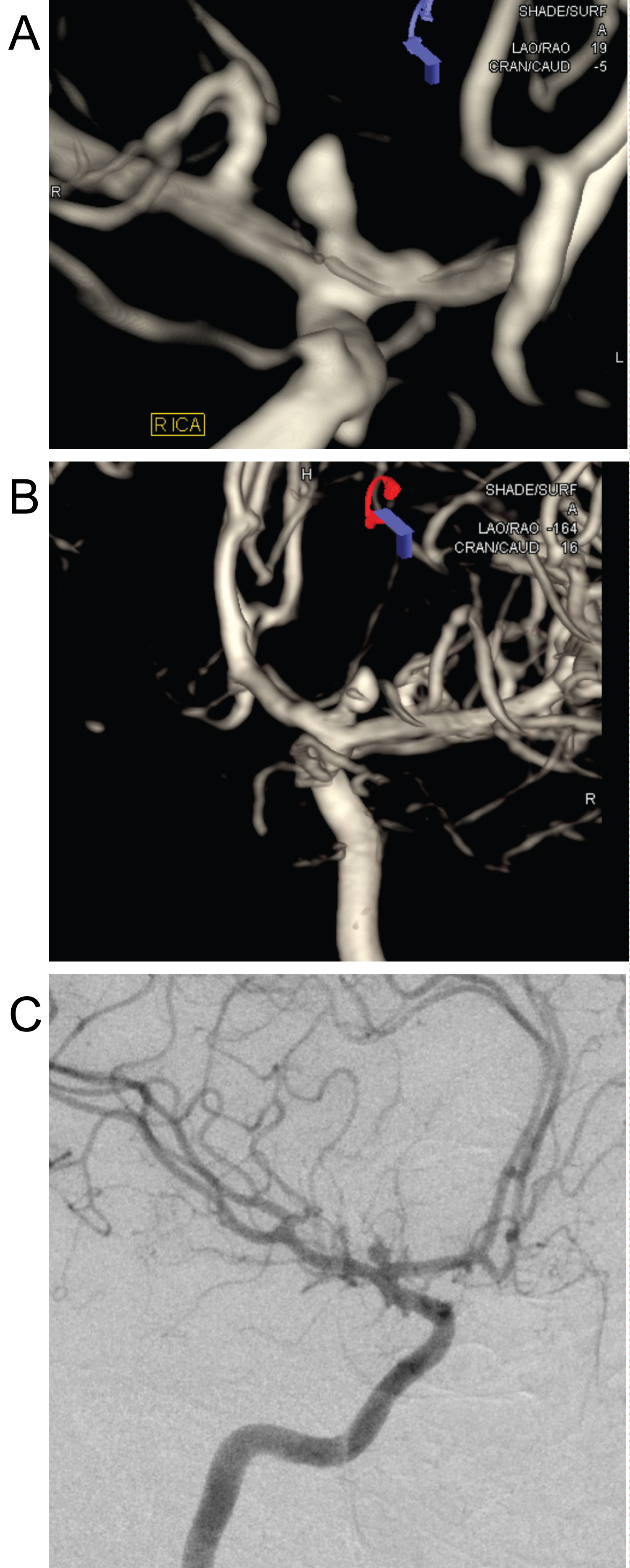 Figure 3: DSA image showing saccular aneurysmatic filling with a diameter of 5*3 millimeters at the apex of the Right Internal Carotid Artery, just before the M1 segment of the Middle Cerebral Artery.
View Figure 3
Figure 3: DSA image showing saccular aneurysmatic filling with a diameter of 5*3 millimeters at the apex of the Right Internal Carotid Artery, just before the M1 segment of the Middle Cerebral Artery.
View Figure 3
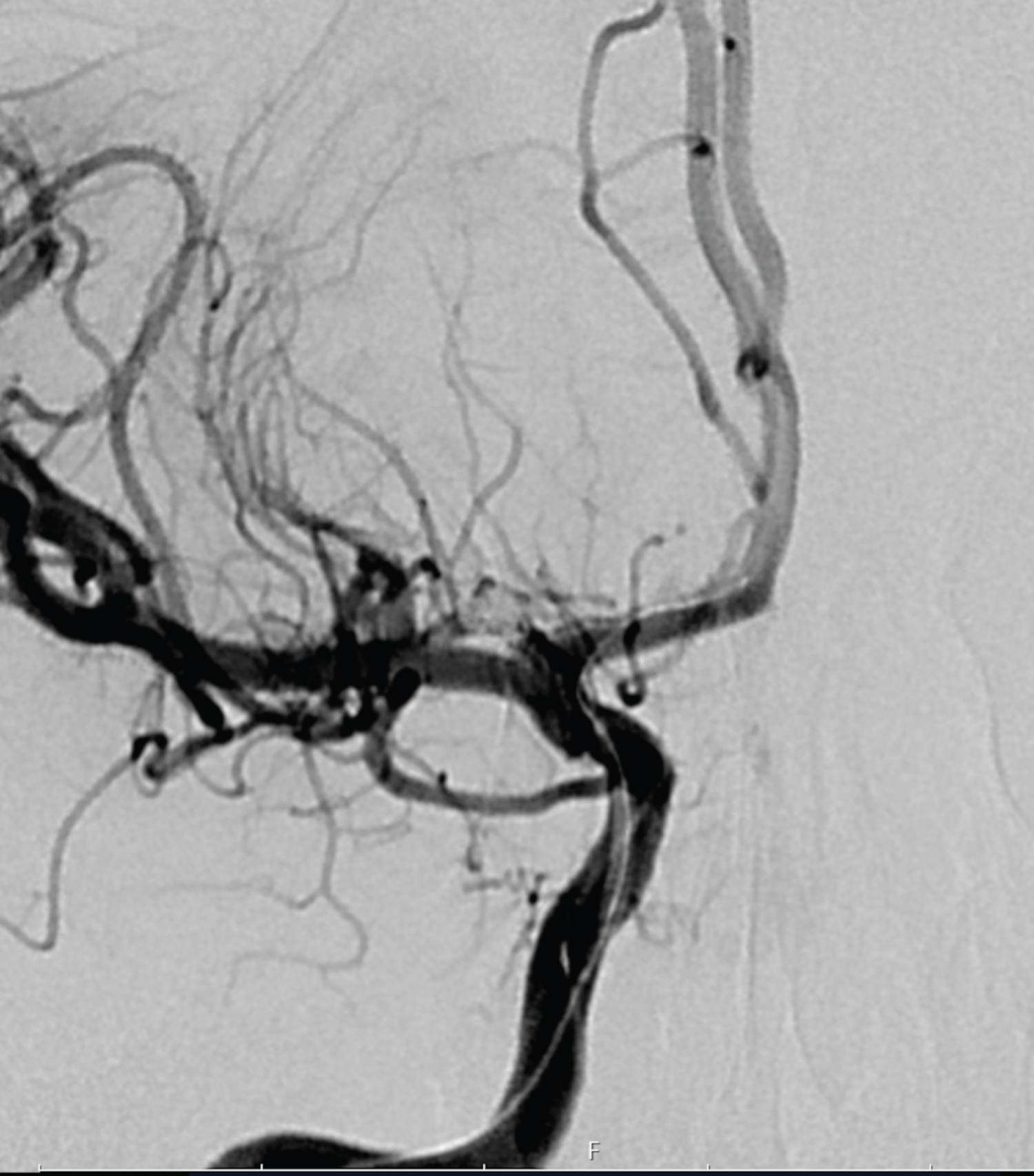 Figure 4: Control DSA image after endovascular coil placement for aneurysm treatment.
View Figure 4
Figure 4: Control DSA image after endovascular coil placement for aneurysm treatment.
View Figure 4
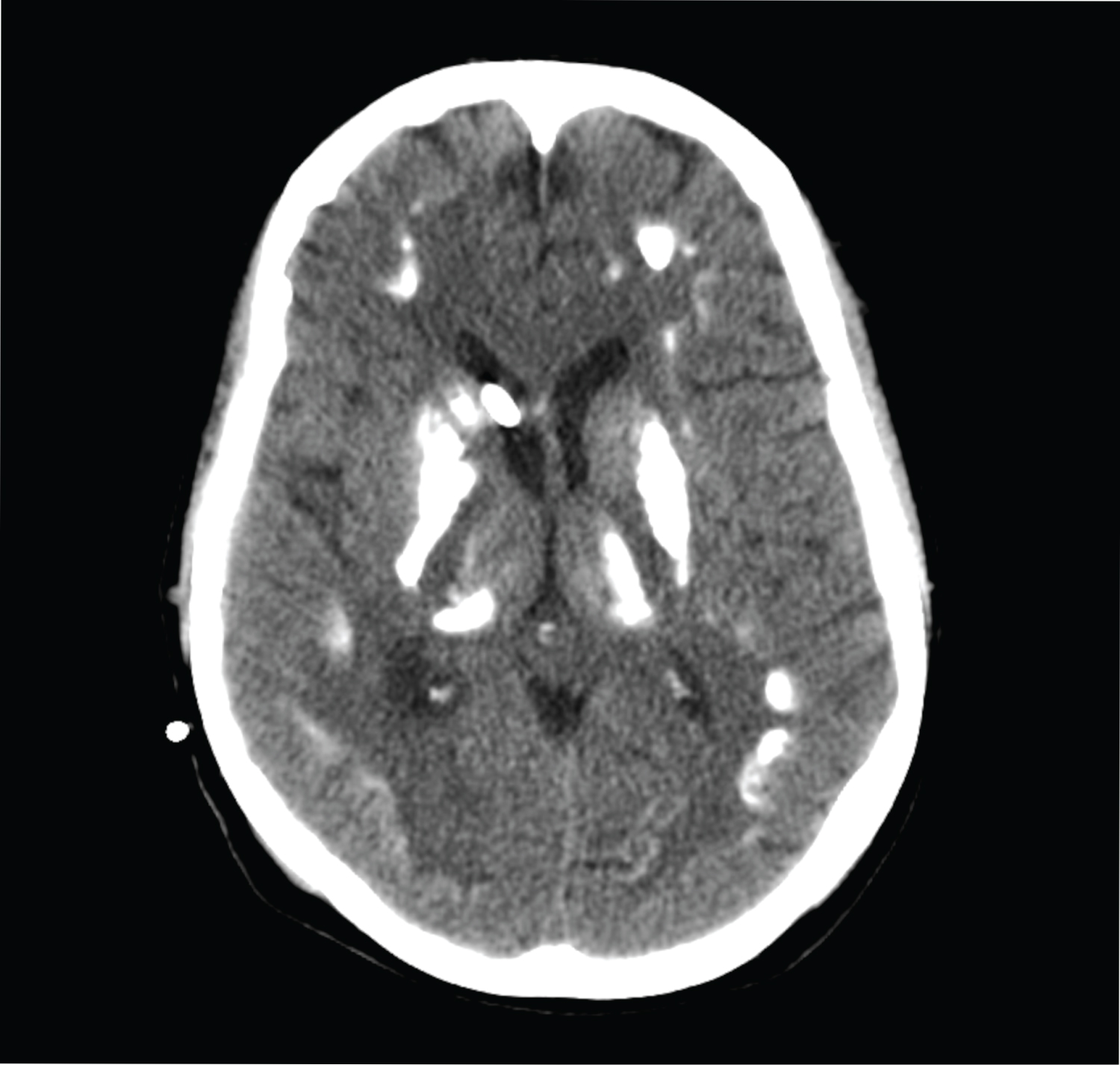 Figure 5: Control brain tomography taken to observe the resorption of hemorrhage after clarification of the cerebrospinal fluid in the External Ventricular drainage catheter.
View Figure 5
Figure 5: Control brain tomography taken to observe the resorption of hemorrhage after clarification of the cerebrospinal fluid in the External Ventricular drainage catheter.
View Figure 5
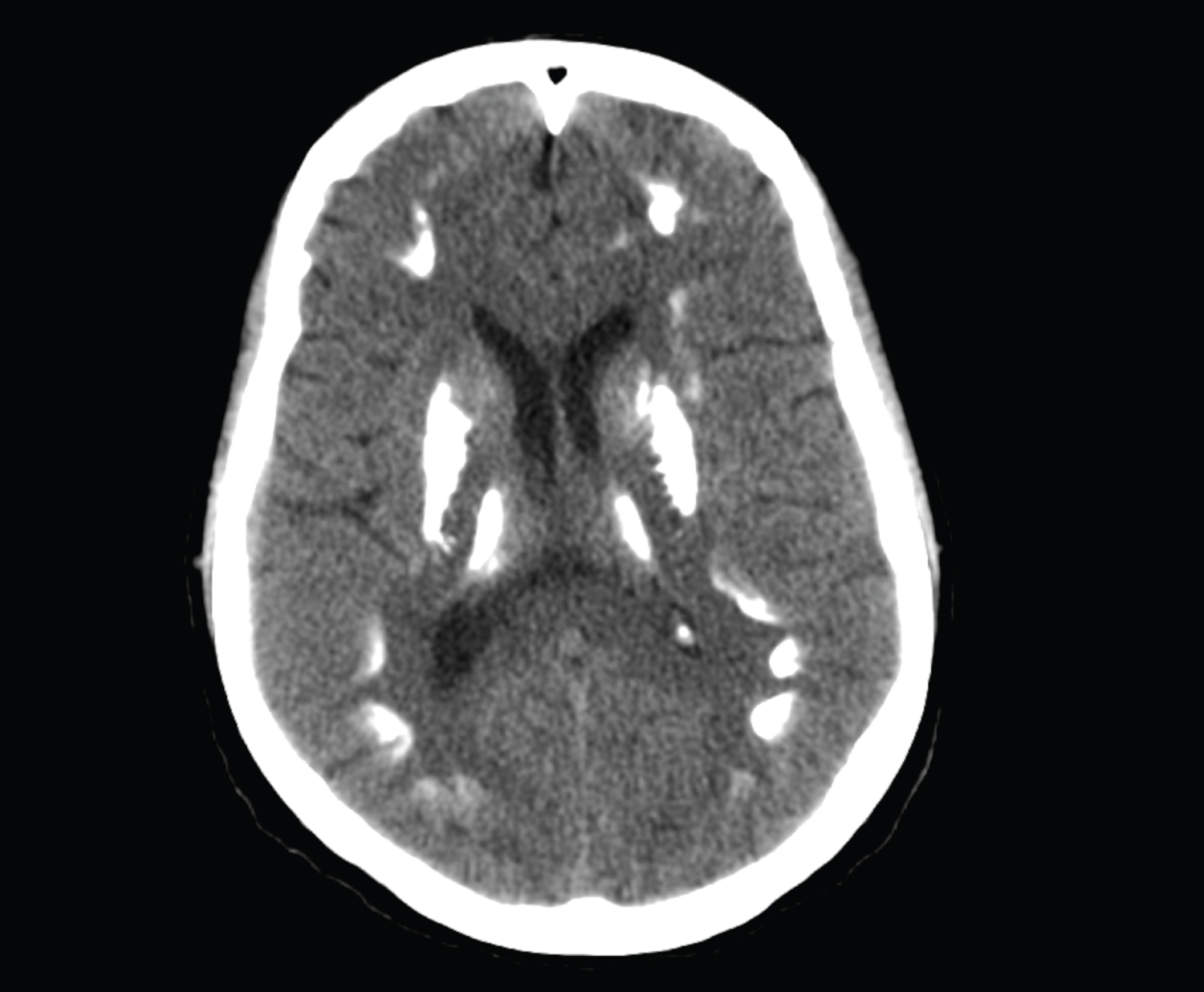 Figure 6: Control brain tomography taken before discharge after removal of the external ventricular drainage catheter.
View Figure 6
Figure 6: Control brain tomography taken before discharge after removal of the external ventricular drainage catheter.
View Figure 6
Fahr's disease, also known as familial idiopathic calcification of basal ganglia, is a rare disorder. Disease may be inherited in autosomal dominant or familial manner orit can be sporadic. Beside inheritance anoxia and/or factors and disorders of the developmental calcium metabolism may cause Fahr's Disease [4]. Idiopathic Fahr's disease cases or idiopathic calcification of basal ganglia characterized by abnormalities. Basal ganglia calcifications are associated with various neurological and metabolic disorders, and calcifications can be frequently encountered in radiological imaging of asymptomatic individuals. Indeed, calcification of the basal ganglia to a certain extent can be considered physiological with aging for 50 years and may be an incidental finding in 15-20% of asymptomatic patients undergoing CT scans [5].
Abnormal calcium deposition is assumed to be due to abnormal brain calcium metabolism or to metastatic deposition due to locally altered blood-brain barrier. Defective iron transport mechanism causes tissue damage that initiates calcification around a nidus composed of free radical production, mucopolysaccharides and related substances. Calcium deposition begins within the vessel wall and perivascular space and gradually expands to encompass the entire neuron. Progressive calcification compresses nearby vessels, reducing blood flow and thus perpetuating the vicious cycle of decreased blood flow, tissue injury, and mineral deposition [6].
Clinical features are important because of the basal ganglia. Calcification can be seen as an incidental finding. Globus Pallidus is the most common site of calcifications for Fahr's Disease. Vertigo, paresis, cognitive disorders, headache, movement disorders, and seizures are the most common symptoms of Fahr's [6,7]. In our case, there were no other findings except headache. CT is the modality of choice in the diagnosis of Fahr's disease because of its superiority in the discrimination of calcification. It's important to note thatMagnetic Resonance Imaging (MRI) can be confusingin intracranial calcifications. It is recommended to integrate the Susceptibility weighted imaging (SWI) phase to the protocol to identify calcifications suspected of neurodegenerative disorders [8,9]. In addition, in our case, intraventricular hemorrhage and subarachnoid hemorrhage (SAH) were detected after imaging, and DSA was performed in addition to CT to elucidate the reason behind SAH. DSA revealed an aneurysm in the M1 segment of the right MCA. Four cases with accompanying cerebrovascular aneurysm have been reported in the literature. In this paper we are presenting the fifth case (Table 1).
Table 1: Four cases with accompanying cerebro vascular aneurysm have been reported in the literature. In this paper we are presenting the fifth case (Table 1). View Table 1
In conclusion, although the pathogenesis of Fahr's disease is not known exactly, it can be said that it facilitates the formation of aneurysm due to mineral accumulation in the vascular structure. Fahr's disease is a chronic, slowly progressive disease. Rare case reports have been reported in the literature, but its relationship with aneurysm has not been clearly demonstrated.
Ethical approval was not necessary for preparation of this article. Because, this is a retrospective study and no new treatment was used.