Background: Posterior Fossa Dermoid Cysts (PFDCs), associated with a Dermal Sinus (DS), are rare congenital brain tumors. More rarely, PFDCs may complicate with cerebellar abscess or hydrocephalus. These complications are represented in only a few case reports as a separate entity. The Neurosurgical literature has a paucity of information regarding the management approach to PFDC when they complicate with both cerebellar abscess and acute obstructive hydrocephalus.
Case description: Here, we illustrate a PFDC which is exceptionally complicated with Cerebellar abscess and acute obstructive hydrocephalus in an 18-months-old child. The child was treated with Frazier's point External Ventricular Drainage (EVD) insertion, Cerebellar abscess evacuation and PFDC removal in same emergency setting. A week later, a second microscopic surgery for removal of a remnant infected dermoid cyst was also performed. After treating the infection with Intravenous (IV) Antibiotics, EVD was changed to Ventriculo Peritoneal Shunt (VPS) and the child was discharged with significant clinical improvement after 12 weeks stay in the ward.
Discussion: When PFDC is complicated by cerebellar abscess and obstructive hydrocephalus, in addition to abscess drainage and dermoid cyst excision, a sound preoperative planning for the management options of hydrocephalus should be made based on the clinical condition of patients. Insertion of EVD helps for emergent control of hydrocephalus, technical ease of PFDC resection and avoids infectious complications of VPS infection. However, regarding the management of hydrocephalus in PFDCs, it needs further study to decide when to apply CSF (Cerebrospinal fluid) diversion procedures and which options to use.
Cerebellar abscess, Posterior fossa dermoid cyst, Dermal sinus, Hydrocephalus, External ventricular drainage, Ventriculoperitoneal shunt
CSF: Cerebrospinal Fluid; CT: Computerized Tomography; DS: Dermal Sinus; EVD: External; IDC: Intracranial Dermoid Cyst; VD: Ventricular Drainage; PFDC: Posterior Fossa Dermoid Cyst; MRI: Magnetic Resonance Imaging; VPS: Ventriculoperitoneal Shunt
Intracranial Dermoid Cyst (IDC), which are usually diagnosed in children and young adults, are rare congenital benign neoplasms that grow slowly as a result of progressive epithelial desquamation and gland secretion within the cyst [1,2]. Embryologically, IDCs originate from abnormal inclusion of the ectodermal element into the neural tube between the 3rd and 5th week of embryological development [3]. They represent between 0.1% and 0.7% of all intracranial tumours [4]. More rarely, dermoid cysts may communicate with the skin through a narrow tract lined by epithelium (dermal sinus) which, therefore, contains the glandular architecture of the skin, promoting colonization by microorganisms [1]. The skin attached to the dermal sinus may manifest with a skin dimple, skin discoloration or a sinus discharge [5]. In those cases, gram positive skin flora is the most common group of pathogens, but polymicrobial infections are also common [6]. This rare infectious complication can also occur in PFDC. Colamaria, et al., in their 2021's published literature review, informed that there are only 14 cases of PFDCs associated with cerebellar abscesses that had been reported [4]. The literature, nearly all of the articles about dermoid cysts discuss about their potential infectious complications. However, there is a little knowledge about hydrocephalus and management of hydrocephalus in patients with PFDCs [7]. Here the authors illustrate a PFDC complicated by cerebellar abscess and acute obstructive hydrocephalus in a podiatric patient; the experience to its management approach is shared as well.
An 18-months-old female child, without remarkable medical history was admitted to our institution with a month history of motor developmental regression signs (inability to hold her head upright and to sit) and a week history of frequent vomiting and irritability. The parents noticed the child had decreased level of alertness the day she visited our institution. Neurologic examination showed a lethargic child with a head circumference of 48.5 cm and bulged anterior fontanelle.
Brain Magnetic Resonance Imaging (MRI) showed three ring enhancing cystic lesions occupying the vermis and the left cerebellar hemisphere. The lesions were associated with surrounding cerebellar edema and obstructive hydrocephalus with transependymal edema (Figure 1). On T2-weighted sequence, DS was visualized as a narrow strand of tissue passing obliquely from the midline cyst wall to diploic space of occipital bone which was a significant clue to suspect the possibility of infected IDC (See Figure 2).
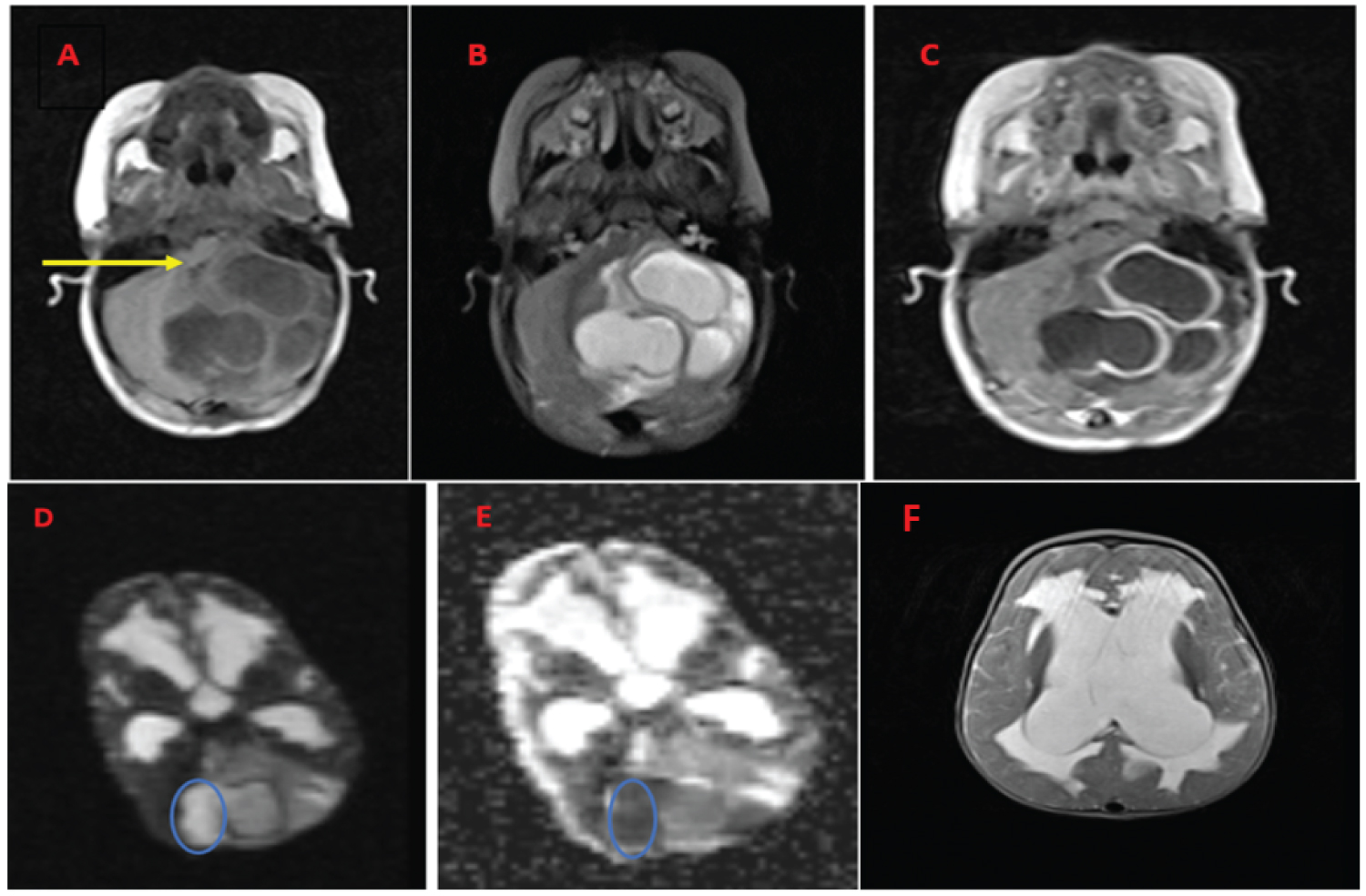 Figure 1: A) Brain MRI showing cerebellar abscess associated with posterior fossa dermoid cysts causing obstructive hydrocephalus. The axial images show T1 hypointense; B) T2 hyperintense three cerebellar cysts causing surrounding cerebellar edema and mass effect on the 4th ventricle; C) On T1 contrast imaging the cysts' wall has enhancement which is not complete in the cyst located at midline; D) The medial part of the midline cyst has diffusion restriction, being bright on DWI sequence; E) Dark on ADC map; F) The axial T2-weighted shows markedly dilated lateral ventricles with trans ependymal edema due to the obstructive hydrocephalus.
View Figure 1
Figure 1: A) Brain MRI showing cerebellar abscess associated with posterior fossa dermoid cysts causing obstructive hydrocephalus. The axial images show T1 hypointense; B) T2 hyperintense three cerebellar cysts causing surrounding cerebellar edema and mass effect on the 4th ventricle; C) On T1 contrast imaging the cysts' wall has enhancement which is not complete in the cyst located at midline; D) The medial part of the midline cyst has diffusion restriction, being bright on DWI sequence; E) Dark on ADC map; F) The axial T2-weighted shows markedly dilated lateral ventricles with trans ependymal edema due to the obstructive hydrocephalus.
View Figure 1
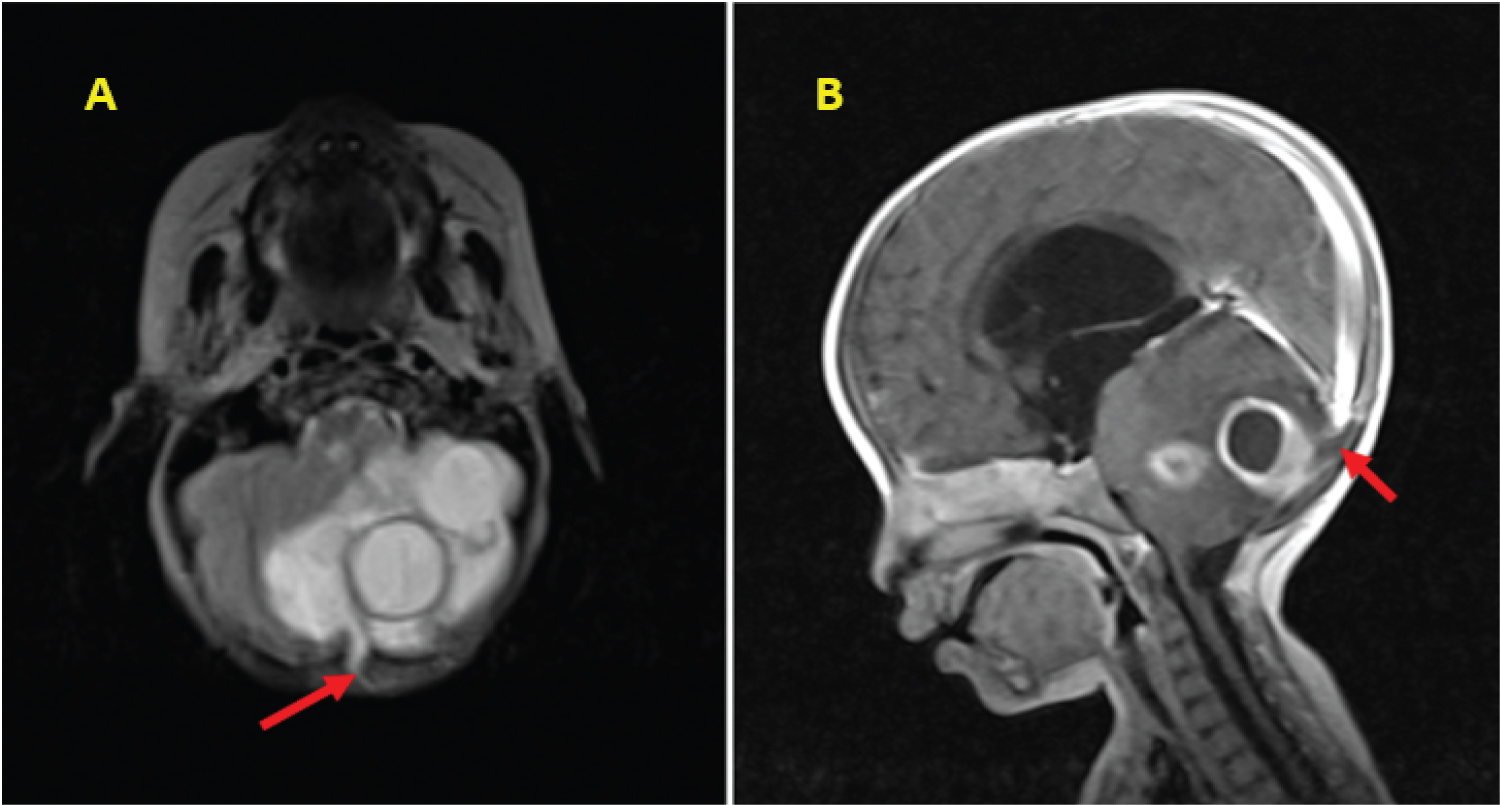 Figure 2: A) Axial T2-weighted; B) Sagittal T1-weighted contrast sequence showing dermal sinus (red arrow) attached to the midline dermoid cyst and the diploic space of the occipital bone.
View Figure 2
Figure 2: A) Axial T2-weighted; B) Sagittal T1-weighted contrast sequence showing dermal sinus (red arrow) attached to the midline dermoid cyst and the diploic space of the occipital bone.
View Figure 2
With the possible diagnosis of infected PFDC causing acute obstructive hydrocephalus, the child was operated on emergency setting. Under general anesthesia, she was positioned prone with a horse shoe head rest. After shaving the hair on the occipital region, we inspected reddish discoloration of the skin; The first procedure we did was inserting EVD at Frazier's point was done. Initially 5 cc of CSF was drained which was clear and came out under high pressure. For the management of the infected PFDC, Sub occipital craniotomy was done to remove the dermal sinus and the dermoid cyst wall containing the abscess cavity. The cyst cavity contained non-foul-smelling abscess and a shaft of hair attached to the cyst wall.
The child was kept on IV antibiotics (Vancomycin, Ceftriaxone and Metronidazole) for empirical coverage of gram positive, gram negative and anerobic bacteria. On control CT scan, there was a remnant ring enhancing lesion in the lateral part of left cerebellar hemisphere which was removed by Microscopic Surgery a week after the first surgery. Postoperatively, as there was no bacterial growth on culture result, the same antibiotics were completed for 8 weeks. Subsequently, Ventriculoperitoneal shunt was inserted and the child was discharged with significant improvement. The diagnosis of Dermoid cyst was confirmed with the histologic section showing cyst lined by keratinizing stratified squamous epithelium with intraluminal hair shaft and keratin flakes (See Figure 3).
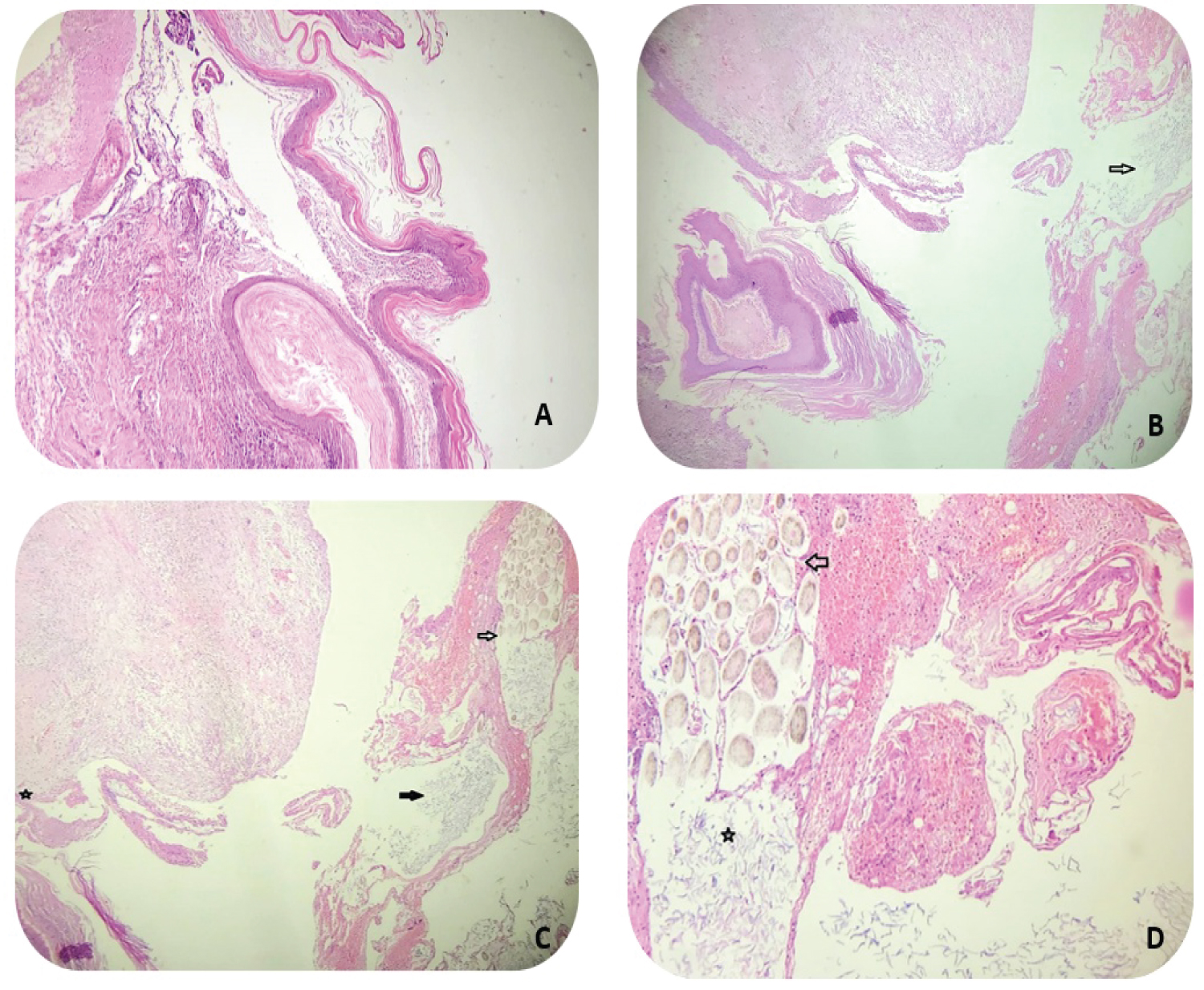 Figure 3: Low power (Magnification ×10) magnification photomicrographs showing. A) Cyst wall lined by keratinizing stratified squamous epithelium; B) With adjacent intraluminal keratin flakes (Arrow); C) Intraluminal hair shaft (white arrow), intraluminal keratin flakes (Black arrow); D) High power (Magnification ×40) magnification photomicrographs showing intraluminal hair shaft (arrow) and intraluminal keratin flakes (asterisk).
View Figure 3
Figure 3: Low power (Magnification ×10) magnification photomicrographs showing. A) Cyst wall lined by keratinizing stratified squamous epithelium; B) With adjacent intraluminal keratin flakes (Arrow); C) Intraluminal hair shaft (white arrow), intraluminal keratin flakes (Black arrow); D) High power (Magnification ×40) magnification photomicrographs showing intraluminal hair shaft (arrow) and intraluminal keratin flakes (asterisk).
View Figure 3
Dermoid cysts may occur anywhere within the skull, but their commonest single site is in the posterior fossa at or near the midline [3,7]. Their most common site in the posterior fossa is usually at the vermis or adjacent meninges and infrequently within the fourth ventricle [1,5]. While the main part of PFDC almost always overlies the vermis, asymmetric growth over one cerebellar hemisphere can be seen [5]. They can assume extradural or intradural locations, with the latter one being more common. The embryological development of the Dermal Sinus associated with DCs in the posterior fossa is not always the same; it can be absent, partially or completely developed [8].
In our case, there was one major dermoid cyst in the midline with other 2 daughter cysts located in the left cerebellar hemisphere. All the three dermoid cysts were intradurally located; the one in the midline had a communication with a dermal sinus passing. However, except reddish discoloration of the skin there was no skin dimple, swelling or discharging sinus.
Dermoid cysts have characteristic CT and MRI appearances which significantly depend upon the amount of lipid present in the lesions [1]. On CT scan, they are typically well circumscribed hypodense or scarcely isodense lesions [5,9,10]. On MRI images, dermoid cysts are typically hyperintense on T1-weighted and hypo- to hyperintense on T2-weighted sequences [10,11]. In case of cyst rupture or abscess formation, they may exhibit hypo intensity on T1-weighted images and hyperintensity on T2-weighted images [1]. Unlike epidermoid cyst, dermoid cysts do not demonstrate restricted diffusion [12]. Preoperative MRI has a significant value in the visualization of dermal sinus associated with infected PFDC [1]. In the presence of infection or abscess associated with dermoid cysts, they characteristically show moderate to marked enhancement of the capsule on both contrast CT and MRI [5,9,10]. In our case, the MRI revealed T1 hypo intensity, T2 hyperintensity and partly diffusion restriction of the dermoid cysts which can be explained by the presence of superinfected cysts. Due to the patient's emergent condition, the patient was not scanned with Brain CT which has limited us in getting the detailed preoperative occipital bony anatomy which can be altered by the presence of DS.
Generally speaking, with prompt diagnosis and appropriate treatment, the prognosis for patients with PFDCs is rewarding [1,2,6]. Their curative treatment is microsurgical excision of the dermoid cyst including the dermal sinus. Complete removal of the tumour is recommended provided that important neurological structures in the vicinity of the tumour are not injured. Radical resection may be possible in 80-87.5% of the cases [1]. If the cyst is significantly attached to the brain structures, it is not a hard-and-fast rule to perform total removal. In such cases, cautious bipolar coagulation of the remaining cyst wall is likely to prevent recurrence. For the purpose of prevention of infection occurrence, rinsing the cyst's cavity with Amikacin solution is reported to be useful. After surgical management of a posterior fossa dermoid cyst, tumour recurrence is extremely rare [1].
In case of an infected dermoid cyst with dermal sinus of posterior fossa, in addition to surgical management post operative systemic antibiotic therapy should be administered as a central component of treatment. Until culture result dictates the choice of antibiotics, coverage of gram-positive, gram-negative, and an aerobe pathogen is recommended. A longer antibiotic course of 6 to 8 weeks should be used depending on the clinical course and the resolution of imaging finding [2,6].
ICDs can cause hydrocephalus when the cyst rupture into subarachnoid space, meningitis complicates dermoid cysts/dermal sinus or dermoid cyst mechanically obstructs CSF pathways [2,6,12]. In the literature, there is no applicable and guiding management algorithm for hydrocephalus associated with ICDs [6]. As there is a risk of CSF contamination or cyst rupture, the safety of VPS insertion during surgical resection of dermoid cyst is questionable. In the absence of infection or CSF contamination, insertion of EVD with the plan of changing it to VPS might not be a safe option due to the risk of CSF infection post-operatively.
For cases like ours, when obstructive hydrocephalus occurs secondary to infected PFDCs, extensive search in the literature showed no tool to stratify patients who need CSF diversion procedure in addition to the surgical resection of the dermoid cyst and abscess drainage. This might be decided based on radiological and clinical condition of patients. When CSF diversion is planned, insertion of EVD may facilitate more rewarding operative circumstances and may diminish the probability of permanent cerebrospinal fluid diversion procedures [2]. Since infection is a major risk in those patients, inserting a shunt at the same session of tumour removal may not be achieved [9].
Infected posterior fossa dermoid cyst should be entertained as differential diagnosis when cerebellar abscess associated with dermal sinus tracts are present; even if, remarkable overlying skin lesions are not visualized on physical examination. Appropriate utilization of CT scan and different sequences of MRI provide ample information in making preoperative diagnosis of dermoid cysts. In the presence of acute hydrocephalus associated with infected dermoid cyst, CSF diversion procedures might be required in addition to cyst removal based on patient's clinical condition. Insertion of temporary external ventricular drainage, while the infection is being treated with systemic antibiotics, is a wise option than inserting ventriculo peritoneal shunts in the first setting.
The authors took a written informed consent from the parents for taking the case details for publication of this case report.
None.
Conceptualization: Amanuel Firew Dilnesaw, Henok Teshome Molla; Original manuscript: Amanuel Firew Dilnesaw; Histopathological figures and diagnosis report: Hidaya Yahya Mohammed, Fadil Nuredin Mohammed; Manuscript review and editing: Abel Gizaw W/Gabriel, Henok Teshome Molla, Amanuel Firew Dilnesaw.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.