Intracranial tumors of different histologic morphologies in concurrent existence are extremely rare with an incidence rate less than 0.9% among the cases of primary brain tumors. Here, we report a case of a 57-year-old male who was diagnosed with coexistence of nonfunctioning pituitary adenoma (PA) and intraventricular glioblastoma multiforme (GBM). She presented with blurred vision from pituitary tumor and right-sided weakness from intraventricular tumor. Interhemispheric transcallosal approach was performed for resection of the intraventricular tumor and the pituitary tumor was subsequently removed by endoscopic transsphenoidal approach. Previous literature regarding the coexisting brain tumor and genetic predisposing factors were also reviewed. Concurrent PA and GBM should be considered in patients presenting with sellar tumor and other brain tumor.
Co-existing brain tumors, Multiple primary brain tumors, Intraventricular glioblastoma multiforme, Pituitary adenoma
ATRX: Alpha-Thalassemia/Mental Retardation, X-Linked; CNS: Central Nervous System; CSF: Cerebrospinal Fluid; EGFR: Epidermal Growth Factor Receptor; GBM: Glioblastoma Multiforme; GFAP: Glial Fibrillary Acidic Protein; IDH 1: Isocitrate Dehydrogenase 1; LOH: Loss Of Heterozygosity; MEN1: Multiple Endocrine Neoplasia Type 1; MRI: Magnetic Resonance Imaging; NF: Neurofibromatosis; PA: Pituitary Adenoma; PTEN: Phosphatase And Tensin Homolog; TSC: Tuberous Sclerosis Complex; VHL: Von Hippel-Lindau Disease
The occurrence of multiple primary brain tumors is associated with the nature of high-grade tumors which commonly disseminate in cerebrospinal fluid (CSF), such as high-grade gliomas, lymphomas, germ cell tumors, or pituitary carcinoma. However, the coexistence of different histological types of primary central nervous system (CNS) tumors is a rare condition with an incidence rate less than 0.9% [1].
Here, we report a rare case of a 57-year-old male who was diagnosed with concurrent existence of non-functioning pituitary adenoma (PA) and intraventricular glioblastoma multiforme (GBM).
A 57-year-old man presented with sudden blurred vision and right-sided weakness. He had progressive headache five days prior to admission. The patient also had a history of hypertension and right-foot leprosy, which was amputated 10 years ago. On physical examination, the patient was fully conscious. He had visual acuity of 20/200 in both eyes. Visual field test revealed bitemporal hemianopia. Right-sided motor power was rated at grade 2. He had no cutaneous stigmata, history of tumors in other organs, or familial tumors. Magnetic resonance imaging (MRI) of the brain showed two discrete heterogeneous enhancing tumors at the sellar region and in bilateral lateral ventricles. Both tumors were isointense on T1-weighted and heterogeneously hyperintense on T2-weighted images. The sellar tumor was measured 4.0 × 3.4 × 3.2 cm in diameter with hemorrhagic content at the right superior aspect of the tumor. It extended into bilateral cavernous sinuses, sphenoid sinus, and suprasellar area which compressed optic chiasm and the third ventricle (Figure 1). The intraventricular tumor, measured 4.0 × 4.3 × 5.4 cm in diameter, was located in the body of lateral ventricles. It involved the body of corpus callosum, mainly in the left side, with adjacent periventricular brain edema (Figure 2). Blood levels of pituitary hormones were within normal range, and serum tumor markers, including alpha fetoprotein, beta human chorionic gonadotropin, carcinoembryonic antigen, and prostate-specific antigen, were unremarkable. There was no evidence of seeding metastasis on MRI of the whole spine.
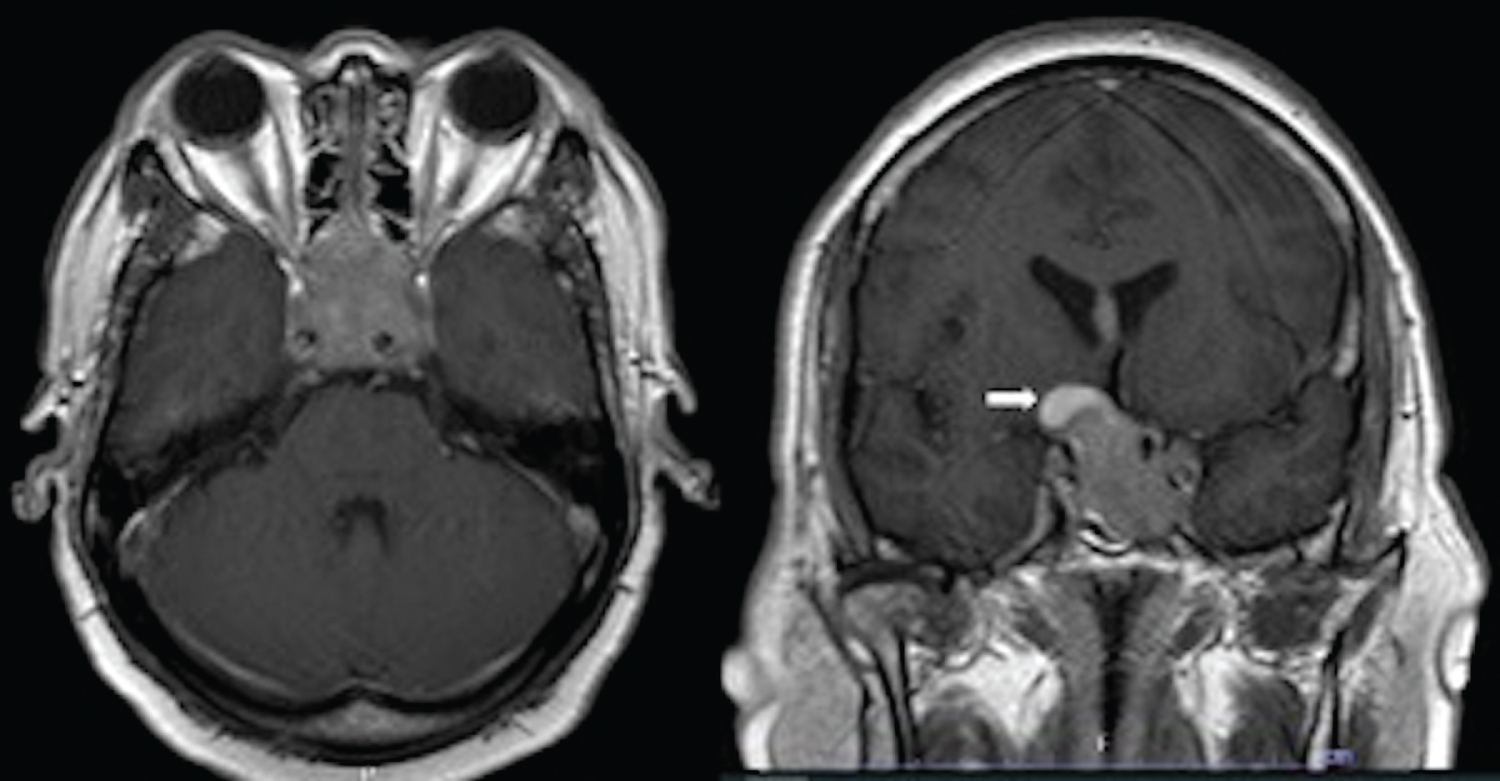 Figure 1: Contrast-enhanced T1-weighted MRI of the brain showing sellar tumor involving bilateral cavernous sinuses, pituitary gland, infundibulum, and optic chiasm in axial (left) and coronal views (right) with hemorrhage at the right superior aspect (white arrow).
View Figure 1
Figure 1: Contrast-enhanced T1-weighted MRI of the brain showing sellar tumor involving bilateral cavernous sinuses, pituitary gland, infundibulum, and optic chiasm in axial (left) and coronal views (right) with hemorrhage at the right superior aspect (white arrow).
View Figure 1
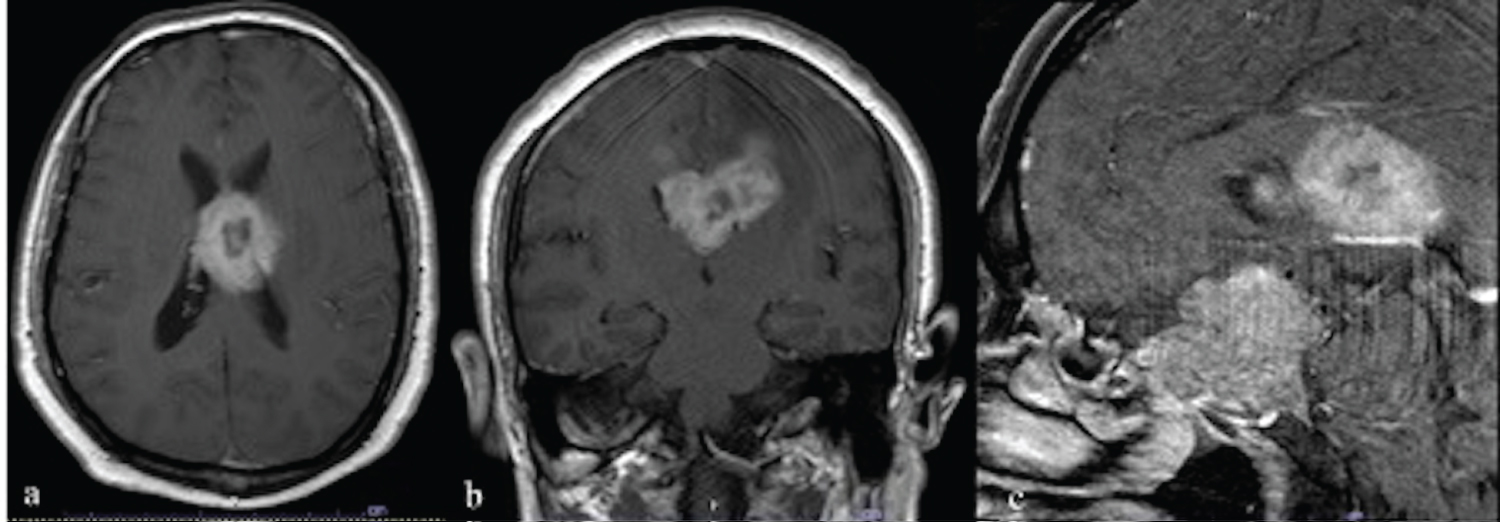 Figure 2: Contrast-enhanced T1-weighted MRI of the brain showing intraventricular tumor occupying in both sides of the lateral ventricles in axial (a), coronal (b), sagittal views (c).
View Figure 2
Figure 2: Contrast-enhanced T1-weighted MRI of the brain showing intraventricular tumor occupying in both sides of the lateral ventricles in axial (a), coronal (b), sagittal views (c).
View Figure 2
The intraventricular tumor was subtotally removed using the interhemispheric transcallosal approach. During the surgery, the tumor was soft and hypervascularized. It occupied in both lateral ventricles and was indistinguishable from the corpus collosum. A week later, the patient underwent the endoscopic transsphenoidal approach for the resection of the sellar tumor. A large soft tumor extending from the sphenoid sinus into the suprasellar area was found. The tumor was subtotally removed with the residual tumor in the cavernous sinuses. The histological findings indicated the diagnosis of GBM for intraventricular tumor with positive for glial fibrillary acidic protein (GFAP) and few positive for alpha-thalassemia/mental retardation, X-linked (ATRX) but negative for isocitrate dehydrogenase 1 (IDH 1) in the immunohistochemical staining (Figure 3). The sellar tumor was compatible with PA with positive staining for Ki 67 at 2% and negative for p53 and all pituitary hormones (Figure 4).
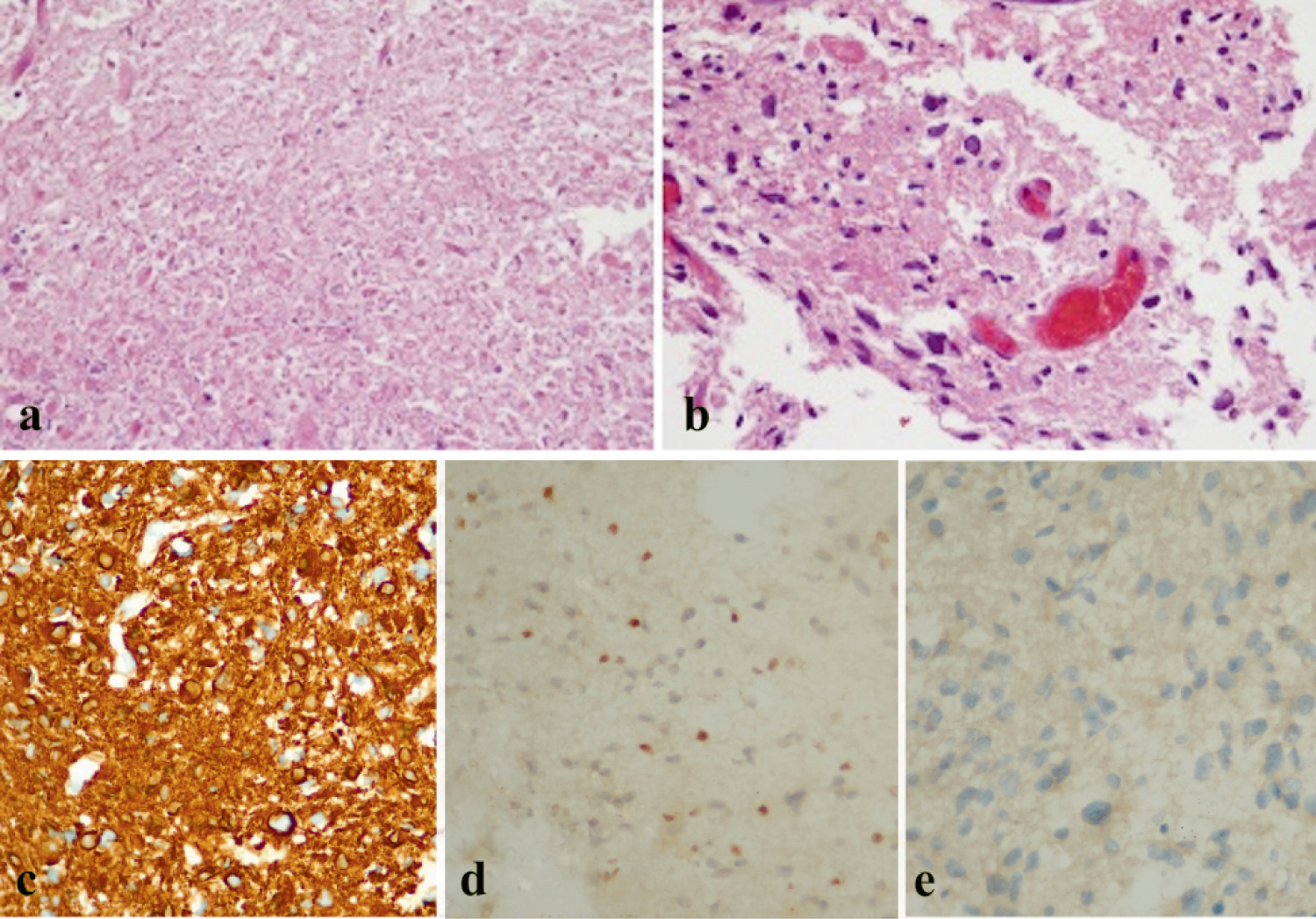 Figure 3: Histopathological appearance of the intraventricular tumor in Hematoxylin and Eosin (H&E) stain was compatible with the diagnosis of GBM: Area of necrotic cells (a), irregular hyperchromatic cells with high nuclear-to-cytoplasm ratio and mitosis (b), the immune markers were positive for GFAP (c) and few positive for ATRX (d) but negative for IDH 1 (e).
View Figure 3
Figure 3: Histopathological appearance of the intraventricular tumor in Hematoxylin and Eosin (H&E) stain was compatible with the diagnosis of GBM: Area of necrotic cells (a), irregular hyperchromatic cells with high nuclear-to-cytoplasm ratio and mitosis (b), the immune markers were positive for GFAP (c) and few positive for ATRX (d) but negative for IDH 1 (e).
View Figure 3
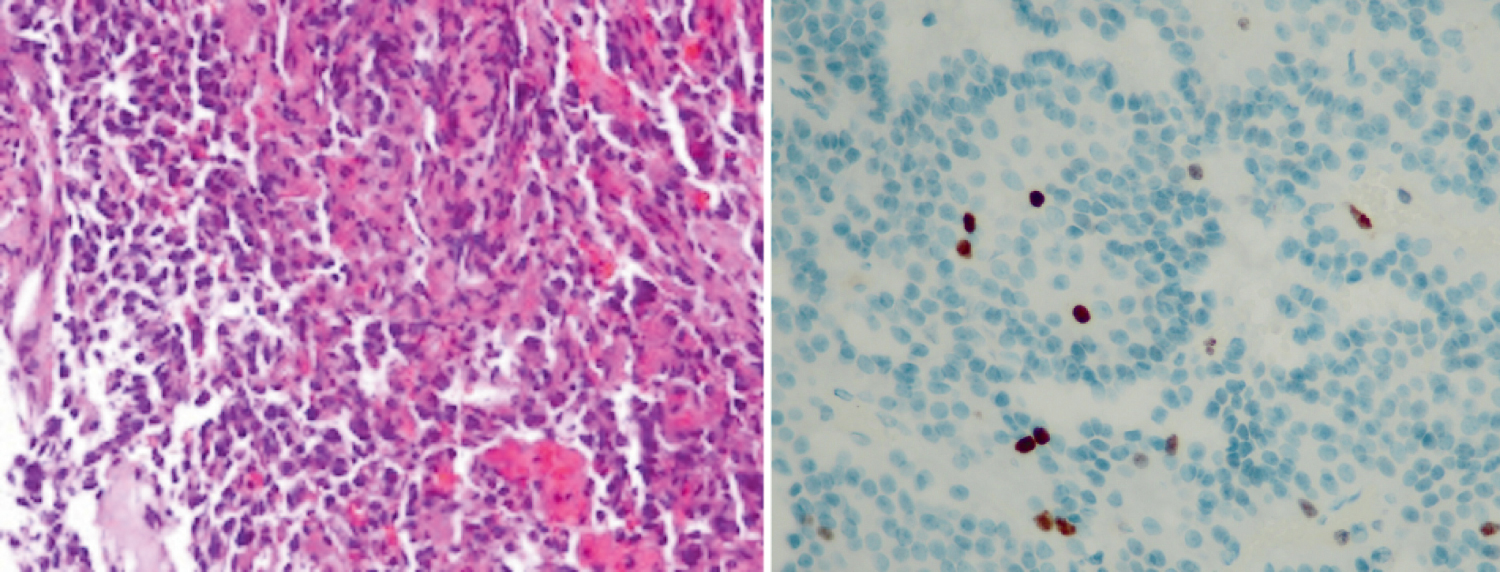 Figure 4: H&E stain of sellar tumor was compatible with the diagnosis of pituitary adenoma: Pleomorphic cells in nested growth pattern with dense nuclei, stippled chromatin, and moderate amount of acidophilic cytoplasm (left). The tumor was positive staining for Ki 67 at 2% (right).
View Figure 4
Figure 4: H&E stain of sellar tumor was compatible with the diagnosis of pituitary adenoma: Pleomorphic cells in nested growth pattern with dense nuclei, stippled chromatin, and moderate amount of acidophilic cytoplasm (left). The tumor was positive staining for Ki 67 at 2% (right).
View Figure 4
After surgery, his vision was improved but the level of weakness remained unchanged. Conventional external beam radiotherapy with a total dose of 60 Gy in 30 fractions and adjuvant Temozolomide were given for the treatment of GBM. The genetic testing revealed no chromosomal abnormalities and no mutations of neurofibromatosis (NF) 1 and 2, tuberous sclerosis complex (TSC) 1 and 2, von Hippel-Lindau Disease (VHL), and multiple endocrine neoplasia type 1 (MEN1) genes. The patient died 4 months later due to the pulmonary embolism.
Coexistence of multiple types of brain tumor is extremely rare. Several studies suggested that the most common coincidences were meningioma-glioma, meningioma-PA, and meningioma-neurinoma [1-3]. Among these, a number of cases with silent meningioma and pituitary adenoma have been reported, 0.3%-1.0% of the population [4-6]. Most of the cases have benign clinical courses without malignant transformation [4,5,7].
This case report is a clear example of concurrent PA with GBM. PA is often found as an incidental finding in radiographic imaging, [8] whereas GBM is one of the most common primary CNS tumors. However, this coexistence is rarely reported in the pertinent literature [9]. To our knowledge, only five cases of this coexistence have been previously reported [1,3,9-11]. Among these, three cases were prolactinomas, and the remaining cases were nonfunctioning PA. All of GBMs from the five case reports located in the cerebral cortices which is the common location of GBM. Therefore, this patient was the first case to be reported on coexistence of intraventricular GBM and nonfunctioning PA.
For GBM, the mutations of phosphatase and tensin homolog (PTEN) loss, epidermal growth factor receptor (EGFR) amplification, and loss of heterozygosity (LOH) of chromosome 10 are associated with primary subtype whereas ATRX mutation, loss of p53, and LOH of chromosome 19 are common in secondary GBM [12]. The immune markers of GBM in this patient were in line with primary GBM which had a poor prognosis. In addition, the immunohistochemical studies of PA in this patient were compatible with null cell adenoma. Based on these findings, we could not find an association between the co-existing of GBM and PA in this patient.
Several studies proposed that the coexistence of intracranial tumors might be associated with genetic predisposing factors or neurocutaneous syndromes, for example, NF, VHL, MEN 1, familial adenomatous polyposis, Lynch syndrome [13-17]. The common genetic syndromes associating with GBM include type 1 NF, Lynch syndrome, and Li-Fraumani syndrome [13-15]. On the other hand, PA is related with TSC and MEN1 [13]. However, there are no clear data of the genetic abnormalities associating with the co-existing PA and GBM. Naydenov, et al. reported a case of PA co-occurring with GBM in nonfamilial Turcot's syndrome but there were no data regarding the genetic mutations [1]. Haciyakupoglu, et al. described a case of null cell PA co-existing with GBM and reported the immunohistochemical findings of both tumors [9].
Although, they concluded that both tumors were unrelated from each other, the results were based on immunostaining not a genetic testing. In our case, the patient did not have signs of neurocutaneous syndromes, and the genetic testing was unremarkable for the common neurocutaneous syndromes. Thus, PA and GBM which were concurrently found in this case might be independent. Nevertheless, this patient presented with multiple brain tumors in his fifth decade of life with a history of leprosy which was occasionally difficult to be precisely distinguished from cutaneous manifestation of, genetic predisposing factors which may have triggered tumor proliferation could not be excluded.
Although high-grade tumors and metastases are common in patients with multiple brain tumors, coexistence of different types of primary CNS tumors should be added to the differential diagnosis. Among these, the concurrent PA and GBM should be considered in patients presenting with sellar tumor and other brain tumor. According to the low incidence of concurrent multiple brain tumors, the data on their genetic profiles was limited. Further research should be performed in order to determine associated predisposing factor(s) or to gain insights for its early detection.
This study was conducted with the approval of the Medical Ethics Committee of Thammasat University in accordance with the tenets of the Declaration of Helsinki.
Informed consent was obtained from the patient.
Not applicable.
None.
We are grateful for histopathological image courtesy of Dr. Chatchai Thamwongskul, Department of Pathology and Forensic Medicine, Thammasat University Hospital, Pathumthani, Thailand.
None.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Chattrabongkot Chokaouychai: Conceptualization, writing of case report, editing, proof reading; Raywat Noiphithak: Editing, Proof reading.