Introduction: Glioblastoma is the most common intrinsic brain tumor. Albeit often located adjacent to the ventricular system, intraventricular glioblastomas are rare. We present a case of a third ventricular glioblastoma and discuss effective diagnostic and therapeutic options.
Case description: A 72-year-old woman presented with forgetfulness, dizziness and nausea. Magnetic resonance imaging revealed a mass in the third ventricle with infiltration of the posterior corpus callosum and obstructive hydrocephalus. Endoscopic biopsy and third ventriculostomy were performed in a single procedure. The histopathological diagnosis was glioblastoma. Postoperatively, the obstructive hydrocephalus regressed and the patient was clinically improved.
Discussion and conclusion: Glioblastomas in third ventricle are rare. Because results have been unfavourable in previous attempts, radical excision in most cases is not recommendable. Endoscopic third ventriculostomy with simultaneous tissue sampling is less invasive and therefore should be preferred over a larger microsurgical approach and ventriculoperitoneal shunt implantation.
Glioblastoma, Third ventricle, Hydrocephalus, Third ventriculostomy, Biopsy
Gliomas are the most common malignant primary tumors of the central nervous system (CNS).
They usually occur in the cerebral hemispheres, especially in the frontal and temporal lobes.
Third ventricular glioblastomas are rare and challenging due to their location close to and possibly infiltrating eloquent adjacent neuronal structures. Complete microneurosurgical removal is associated with significant morbidity.
Endoscopic access to the third ventricle is an alternative method which allows not only for tumor excision and histological diagnosis but also for simultaneous treatment of occlusive hydrocephalus by means of ventriculostomy, septostomy, or aqueduct stenting. Operative time and morbidity rates are lower with endoscopic access to the third ventricle than with conventional access.
Lesions in the third ventricle often cause occlusive hydrocephalus due to blockage of the foramina Monroi and the cerebral aquaeduct.
In some of these cases, clarification of diagnosis and grade of malignancy to devise an optimal therapeutic strategy is necessary. Obviously, a combination of diagnostic biopsy and treatment of the hydrocephalus in a single procedure would be desirable in these cases. We report a case were this strategy has been followed, and discuss clinical, radiological, diagnostic and therapeutic implications along with a review of the literature.
We take over a 72-year-old female Patient from another Clinic with deterioration of general condition, dizziness, nausea and disorientation. The CT and MRI of the neurocranium showed widening of the ventricles with an unclear mass in the third ventricle.
On neurological examination was the patient awake and all around oriented. Gait was very unsteady. There was no obvipus deficit in any extremies.
Because of the clinically and image-morphologically confirmed hydrocephalus, we indicated endoscopic third ventriculostomy and simultaneous endoscopic biopsy to confirm a histologic diagnosis.
On histopathology, the diagnosis of glioblastoma was established. After staining, the neoplastic tissue showed atypical cells, proliferation, and necrosis on microscopy. On a molecular level, the tumor expressed S 100 proteine, CD34 as well as Olig-2. Some of the tumor cells showed labeling for pancytokeratines AE1/AE3. The tumor was negative for BRAF V600 and R132 mutations. Methylation of the MGMT promoter was not present. IDH-1, ATRX, H3K27 were wild type, tumor cell were without significant p53 expression (Figure 1 and Figure 2).
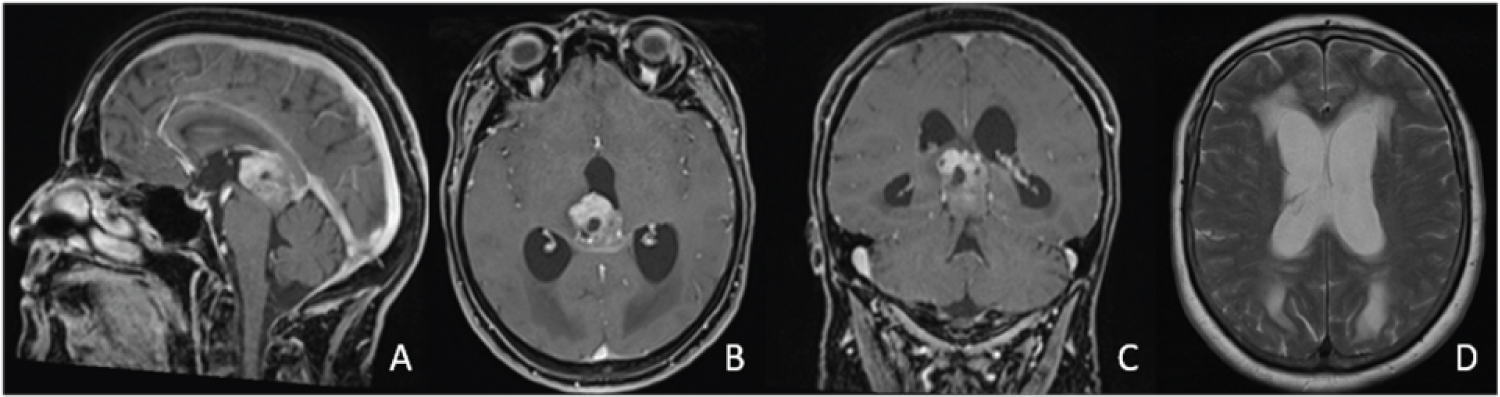 Figure 1: A,B,C) Inhomogeneously contrast-enhancing tumor predominantly located in the third ventricle with infiltration of splenium corporis callosum and obstruction of the aqueduct; D) Causing occlusive hydrocephalus.
View Figure 1
Figure 1: A,B,C) Inhomogeneously contrast-enhancing tumor predominantly located in the third ventricle with infiltration of splenium corporis callosum and obstruction of the aqueduct; D) Causing occlusive hydrocephalus.
View Figure 1
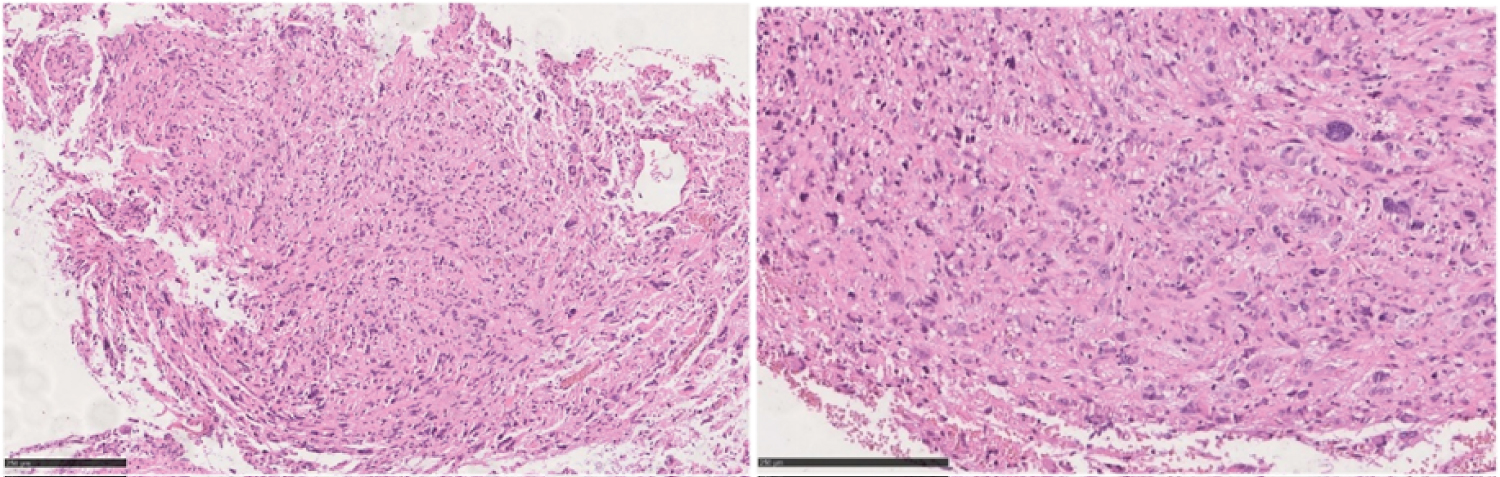 Figure 2: A, B) Microscopic appearance of the tumor shows atypical cells, necrosis and endothelial proliferation.
View Figure 2
Figure 2: A, B) Microscopic appearance of the tumor shows atypical cells, necrosis and endothelial proliferation.
View Figure 2
The WHO CNS5, the fifth edition of the WHO Classification of Tumors of the central nervous system (CNS), published in 2021, has taken a new approach to classifying gliomas, glioneuronal tumors, and neuronal tumors, dividing them into six distinct families. Glioblas-tomas as IDH wild-type are classified alongside IDH-mutant astrocytoma, oligodendroglioma, IDH-mutant, and 1p/19q-codeleted under the adult type diffuse gliomas family. Usually, these gliomas are found in the cerebral hemispheres, especially in the frontal and temporal lobes, and rarely in the ventricles. Review of the literature revealed few cases in which the glioblastoma originated in the third ventricle [1,2]. In the comprehensive review of 987 glioblastoma neoplasms performed by Kleihues not a single third ventricular glioblastoma was detected.
Differential diagnoses of tumors located in the third ventricle include colloid cysts, meningiomas, germinomas, craniopharyngiomas, lymphomas, choroid plexus papillomas, subependymal giant cell astrocytomas, chisasmatic and hypothalamic benign astrocytomas.
The cellular origin of glioblastomas located purely in the third ventricle is still unknown. It is believed that they may originate from the subependymal glial tissue surrounding the ventricle Prieto, et al. [3].
In our case, it was assumed that the tumor originated in the third ventricle and only secondarily spread into surrounding anatomical structures.
Patients with third ventricular glioblastomas develop symptoms such as vomiting, nausea and severe headaches that can be attributed to obstructive hydrocephalus. Our patient had increased intracranial pressure symptoms, accompanied by nausea, vomiting, headache and disorientation, corresponding to obstructive hydrocephalus.
Enhanced MRI of the brain with gadolinium is the best diagnostic imaging tool for the evaluation of the ventricular glioblastomas. The presence of necrosis and ring enhancement are suggestive signs of glioblastoma, yet not pathognomonic.
Glioblastomas are classically treated with surgical tumor resection followed by combined radiochemotherapy Gacic, et al. [4].
Glioblastomas in the third ventricle pose a major challenge to neurosurgeons in terms of the degree of tumor resection due to the adjacent eloquent structures. Various approaches to the third ventricle have been described in the literature, e.g., the frontal-transcortical-transventricular approach, the subfrontal-interhemispheric approach, the pterional approach, and the infratentorial-supracerebellar approach Prieto, et al. [3].
The endoscopic approach, which is relatively new in the treatment of third ventricular tumors, allows for simultaneous relief of obstructive hydrocephalus caused by the tumor and access to the tumor itself. Reported operative time and morbidity rates are lower with endoscopic approaches to the third ventricle than with microsurgical approaches. While the degree of resection may be higher with the microsurgical approach than the neuroendoscopic approach, the risk of major neurological deficits is also higher.
Although third ventricular glioblastomas are very rare, the entity needs to be considered as an important differential diagnosis in lesions of the third ventricle. A neuroendoscopic approach is a safe and effective approach to provide both histopathological diagnosis and treatment of obstructive hydrocephalus.