Over the last decades, there has been a progressive delay in the mean maternal age of childbirth in industrialized countries due to multifactorial causes. The proportion of women giving birth for the first time at 35 years or older is now higher than decades ago. Pregnancy in this age group is considered advanced age pregnancy. As age increases, there is a rising risk of infertility, mainly due to the inability to conceive, as well as gestational and perinatal complications, which can potentially become an emotional and economic burden for couples. Hence, strategies to preserve fertility and delay physiological aging, as much as possible, are needed.
While possible sub-fertility causes are being determined and Assisted Reproductive Techniques (ARTs) are being considered, it might be worth maximizing the opportunities of a natural pregnancy in those patients that still have good follicular reserve. In this regard, some food supplements that have been shown to improve fertility, reduce oxidative stress and increase oocyte quality can help to achieve a natural pregnancy. Here we present a series of clinical cases that are representative of the current tendency to delayed parenthood and that show how supplementation with a multi-component food supplement might help to increase the pregnancy rates in this population.
Advanced maternal age (AMA) is defined as childbearing by a woman over the age of 35 [1]. This population group has been increasing over the last decades in industrialized countries due to multifactorial reasons, many of them being due to societal changes such as the incorporation of women into the labor market, the usage of contraceptive methods, and the prioritization of education and careers, as well as increasing economic instability [1-5]. Delayed first pregnancy partially explains the declining birth rate in advanced countries, as older motherhood has an impact on fertility, affecting population structure and family size [6].
As age increases, there is a reduction in fertility due to multifactorial causes, including reduction of ovarian reserve, oocyte quality, increased chromosomal abnormalities, increased miscarriage rate, reduced implantation rates, increased stillbirth rates and/or metabolic abnormalities [7,8].
These profiles of patients normally ask for medical advice after some period of seeking a pregnancy without success. In most cases, these patients have no risk factors other than AMA and still have a good follicular reserve [9]. For that reason, it is worth using some food supplements that have been shown to improve fertility, reduce oxidative stress and increase oocyte quality [10-12], increasing the chances of having a natural pregnancy while doctors are determining possible causes of sub-fertility, or deciding if ART are needed or which is the most adequate approach for a particular case.
In this sense, some supplements have shown evidence-based data in increasing fertility. Folic acid and vitamin D are the most studied due to their effects on pregnancy rates and/or gynaecological parameters [13-18]. Supplementation with inositol has also been shown to have a positive effect on human reproduction [19-21]. Different inositol isomers exist, each with different effects on human physiological functions (Figure 1). Recent clinical trials have shown that A specific ratio (3.6:1) of Myoinositol: D-Chiro-Inositol (MYO:DCI), the most important inositol isomers found in humans, can improve pregnancy rates, number of live births, and oocyte quality [22-24]. Some antioxidants such as melatonin or coenzyme Q10 have also been clinically demonstrated to have a positive effect on fertility [25-27]. Antioxidant supplementation may be particularly relevant in cases of AMA, as it is well known that ovarian aging is caused by the increased production of reactive oxygen species (ROS) in the ovary, which in turn impacts fertility.
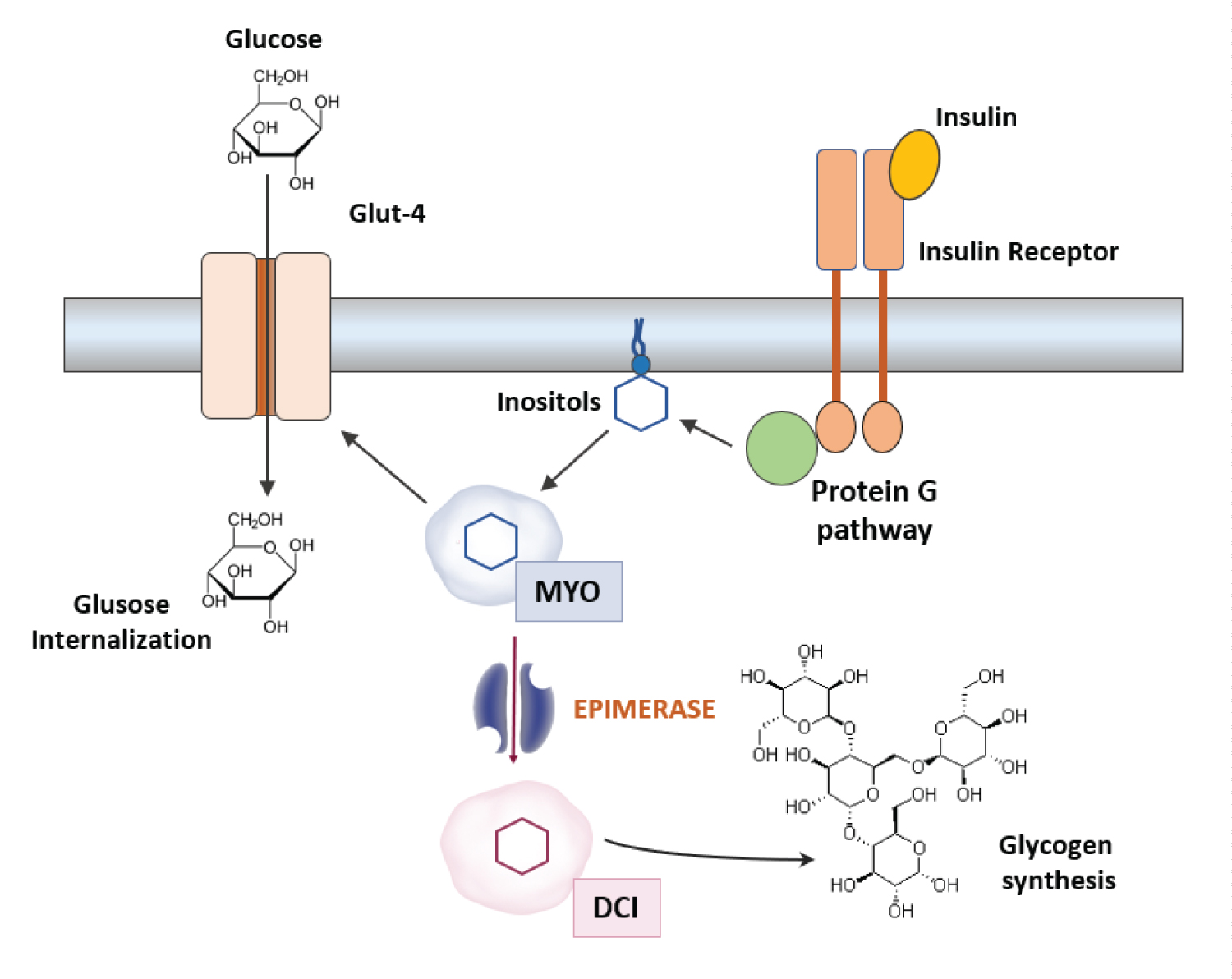 Figure 1: MYO and DCI have different functions in cell metabolism. After Insulin binds to the Insulin receptor (IR), inositol-containing lipids are hydrolyzed from the lipid membrane, releasing myoinositol which induces glucose internalization and consumption through the Glut-4 receptors. On the other hand, the epimerase enzyme catalyzes the isomerization of MYO to DCI, which induces glucose storage through glycogen synthesis.
View Figure 1
Figure 1: MYO and DCI have different functions in cell metabolism. After Insulin binds to the Insulin receptor (IR), inositol-containing lipids are hydrolyzed from the lipid membrane, releasing myoinositol which induces glucose internalization and consumption through the Glut-4 receptors. On the other hand, the epimerase enzyme catalyzes the isomerization of MYO to DCI, which induces glucose storage through glycogen synthesis.
View Figure 1
In this series of clinical cases, we provide preliminary evidence that a combination of a specific 3.6:1 MYO:DCI ratio with, antioxidants, probiotics, vitamins, and minerals may contribute positively to female fertility in AMA. With these clinical cases, we aim to stimulate interest in these food supplements as a possible aid in female fertility, providing a novel tool that could be used by a general gynaecologist before undergoing ART.
Here we present a series of 5 clinical cases of women who are representative of this tendency of delayed conception seen in industrialized countries. Their general clinical data are summarised in Table 1. These women received supplementation with a multi-component food supplement with a specific 3.6:1 MYO:DCI ratio, antioxidants, vitamins, and minerals between 8 and 12 weeks before conception.
Table 1: Here we present a series of 5 clinical cases of women who are representative of this tendency of delayed conception seen in industrialized countries. View Table 1
A 38-year-old patient came for consultation, referring 8 months of subfertility, after frequent unprotected sexual relations. Her clinical history included menarche at 13-years-old, with regular cycles and 3-4 days of bleeding (menstrual formula 3-4/35), and nulliparous (G0; P0; A0). The patient did not have any relevant clinical background, having only had surgery for adenoids and appendicitis during her childhood. The clinical exploration determined a weight of 98 kg and 165 cm height, with a BMI of 32. A transvaginal echography showed an anteverted uterus with an endometrial lamina of 12 mm and a homogeneous appearance, without any gynaecological alterations, and a normal oocyte number for a woman her age.
After the exploration, a sterility study was conducted including serologies, hormonal profile [including Anti-mullerian hormone (AMH)), Rh-group, and spermogram for her partner. None of the analyses found alterations as all test results were within the normal values. Additionally, a liquid-based cytology study was performed showing no cytological alterations.
Given these results, the patient was advised to increase physical activity, and implement a diet in order to lose weight, as well as supplementation with a multi-component food supplement with a specific inositol ratio (3.6:1 MYO/DCI), antioxidants, vitamins, and minerals with a posology of 2 capsules/day for 6 months. After 3 months of supplementation, the patient referred a positive pregnancy test. On physical examination, her BMI was now found to be 27 and an echography control showed an intrauterine gestational sac with vitelline vesicle and embryonarian echo of crown–rump length (CRL) of 5.6 mm (6+1 sg) with positive cardiac activity. The pregnancy had a normal evolution with the patient giving birth to a 3220 g baby without any major complications.
A 38-year-old patient came for consultation referring 2 years of subfertility without any relevant background. The patient indicated menarche at 13-years-old, with regular 28 day cycles and 5 days of bleeding. She was nulliparous (G0; P0; A0) with gestational desire. The clinical exploration found normal weight, without any gynaecological alterations. Contrast salpingography showed normal permeable fallopian tubes, and echographic study found a normal uterus, regular endometrium, with adequate thickness, ovaries with normal size and morphology with a small number of follicles. Analytics showed all values within the normal range, vitamin D 25 U.
After that, the patient was prescribed 4 months of supplementation with a multi-component food supplement with a specific inositol ratio (3.6:1 MYO/DCI), antioxidants, vitamins, and minerals. Two months after the start of supplementation, the patient came in with amenorrhea and a positive pregnancy test. An echography was performed finding a 3-week gestational sac. The echography was repeated 3 weeks later, confirming a viable 5-week embryo with normal cardiac activity. The supplementation was maintained until week 12 of pregnancy. The patient gave birth to a healthy baby after a pregnancy of normal length and without any relevant obstetric-gynecological complications.
A 43-year-old woman came in for consultation referring 5 years of subfertility while having unprotected sexual relations. Her gynaeco-obstetric medical history included two previous pregnancies with the current partner (G2; P2; A0) and she now expressed gestational desire. The patient had menarche at 14-year-old, with regular cycles of 28 days. The patient was taking Yodocefol® (200 mg Iodine, 400 mg folic acid and 2 mg Vitamin B1) on alternate months. She had no other relevant medical history.
The clinical exploration showed a BMI of 25.6, no toxic habits, nor any gynaecological alteration or relevant medical condition. Given this profile, Yodocefol® was substituted by supplementation with a multi-component food supplement with a specific inositol ratio (3.6:1 MYO/DCI), antioxidants, vitamins, and minerals. After 3 months of supplementation, the patient referred a positive pregnancy test. Exploration by echography showed an intrauterine gestational sac, a normo-evolutive gestation with a 9-week-old embryo with cardiac activity and normal movement. The patient was advised to maintain the supplementation during the whole gestational period. A new echography was scheduled on week 12 of pregnancy, which resulted normal, as well as a triple screening analysis, which showed no chromosomic alterations. The patient gave birth to a healthy baby weighing 3250g after a 40-week and 3-day gestation period (Figure 2).
 Figure 2: Sagittal echography image corresponding to a normo-evolutive foetus at week 12. Images shows no alteration and normal amniotic liquid proportion.
View Figure 2
Figure 2: Sagittal echography image corresponding to a normo-evolutive foetus at week 12. Images shows no alteration and normal amniotic liquid proportion.
View Figure 2
A 37-year-old patient came for consultation referring 6 months of subfertility, the patient had a medical history of endometriosis and uterine myomitosis. The patient indicated menarche at 12-years-old, with regular 28 day cycles and 5 days of bleeding. She had no previous pregnancies (G0; P0; A0) and currently expressed gestational desire. Her medical history did not contain any other relevant medical background. Clinical exploration found a BMI of 22.6, and the aforementioned gynaecologic alterations (endometriosis and uterine myomitosis). The patient was being treated with Levedol® (300 mg N-acetylcystein, 100 mg Alpha-lipoic acid, 12.5 mg Bromelin, 5 mg Zinc) to control the pelvic pain associated with the endometriosis.
Given the patient´s profile, she was prescribed 6 months of supplementation with multi-component food supplement with a specific inositol ratio (3.6:1 MYO/DCI), antioxidants, vitamins, and minerals. Two months after the medical visit and supplementation, the patient came for consultation as she presented with amenorrhea and a positive pregnancy test. At that point she was at week 29 of gestation and the pregnancy evolved without any gynaecological alterations, although the patient was followed due to a short cervical neck, implying an increased risk of pre-term birth.
A 36-year-old patient came for consultation referring 7 months of subfertility, with alpha-thalassemia as a medical background. The patient indicated menarche at 13-years-old, with regular 28 day cycles and 7 days of bleeding. She had one previous pregnancy without complications (G1; P1; A0), and currently expressed pregnancy desire. The clinical exploration found a BMI of 21.2, without any gynaecological alterations. Analyses showed all values within the normal range, with an FSH 14 mU/ml, and LH 26 ng/ml. Spermogram analysis showed all parameters within the normal values (sperm count, motility, morphology, and vitality).
In view of this profile, it was decided to substitute folic acid supplementation for a 6-month supplementation with a multi-component food supplement with a specific inositol ratio (3.6:1 MYO/DCI), antioxidants, vitamins, and minerals. Two months after the consultation and supplementation, at the second menstrual period, the patient came with amenorrhea and a positive pregnancy test. The patient was explored, and echography exploration determined that she was at week 9 of gestation. The pregnancy evolved without any gynaecological alterations.
Multiple elements have an impact on female fertility such as age, body weight, low insulin sensitivity, inadequate dietetic habits, stress, and/or hormonal factors [15,28,29]. Currently, in developed societies, there is an increased tendency to delay maternity. However, this can negatively affect fertility due to the impact of aging [3,30]. The number of women over 35, with no risk factors other than age, coming for consultation due to difficulties getting pregnant is increasing [9]. Nonetheless, subfertility is defined as a year of having unprotected sexual relations without achieving pregnancy [31]. In patients older than 35, who have no risk factors other than age, certain food supplements could be a valuable tool that can be prescribed while sterility studies are performed on the couple. Being overweight is a frequent factor affecting fertility in developed countries [32]. It implies a longer time for conception and a higher risk of infertility [32,33]. Moreover, being overweight increases the incidence of adverse pregnancy outcomes, such as gestational diabetes or hypertension [34]. Some molecules are well known for their insulin-sensitizing properties, which improve fertility, such as metformin and inositols. There are 9 different inositol stereoisomers, with MYO and DCI being the two most relevant ones in the human body [35-38]. These two isomers have different functions. MYO stimulates glucose intake and consumption (mainly through de Glut-4 glucose transporter protein). Hence, tissue with high metabolic activity tends to have higher MYO concentrations. On the other hand, DCI stimulates glucose internalization and glycogen synthesis, as a consequence tissues that tend to accumulate glycogen have higher DCI concentrations. Importantly, although the biological functions are different, supplementation with a combination of both isomers has synergistic effects [39]. Recent studies showed that the combination of MYO and DCI is more effective in increasing the oocyte quality compared to supplementing with one of the isomers alone [40,41]. Since then, different ratios of MYO and DCI have been studied, but there is no consensus regarding which ratio should be used. It is likely that these ratios are particularly relevant depending on the context. A recent study found that supplementation with a ratio of 3.6:1 MYO:DCI was more effective in increasing direct parameters, such as the number of living births, compared to the most frequently used 1:40 ratio. In a different study, it was found that the 3.6:1 MYO:DCI ratio was also more effective in increasing different parameters related to oocyte quality, such as the cytoplasm properties, which may explain the better performance in those patients receiving this ratio. Supplementation with this 3.6:1 MYO:DCI ratio could also be effective in different populations such as those with anovulation problems, altered hormonal profiles, or those with overweight status and some degree of insulin resistance in which this 3.6:1 MYO:DCI ratio has been successfully used to regularize menstrual cycles and improving insulin resistance [42]. Additionally, an important proportion of the population in developed societies suffer from prediabetes, in which a certain level of insulin resistance is present. This condition is widely overlooked as it is asymptomatic, so it is estimated that 80% of cases are not diagnosed [43].
This situation could align with clinical case number 1 in which the patient shows a BMI of 32 that dropped to 27 after combining diet, physical exercise, and supplementation with 3.6:1 MYO:DCI. It is possible that the synergistic effect of 3.6:1 MYO:DCI supplementation with diet and exercise is particularly useful in patients with some degree of insulin desensitization. This could be of special interest in this population due to the fact that under decreased insulin sensitivity conditions, the activity of the insulin-dependent epimerase which converts MYO to DCI is reduced and, consequently, a lower DCI production is obtained [22-24]. As DCI has got higher insulin sensitizing activity than MYO, it is possible that a 3.6:1 ratio could outperform other ratios containing less DCI in this profile of patients.
Aging is well known to affect fertility through different mechanisms, including hormonal changes that have an impact on oocyte quality [7,8]. In this regard, it seems that DCI positively impacts oocyte quality at the ovarian level, affecting follicular fluid composition or the oocyte itself. Although the mechanism is not fully understood, it could be through the modulation of PI3Ks, an important pathway for the oocyte development and quality [22,44]. On the other hand, it is well known that in the context of PCOS, inositols can improve oocyte quality as well as hormonal profiles [23,45]. Hence, we could infer here that a specific ratio of 3.6:1 MYO:DCI could be having a positive impact on fertility by improving the hormonal profile and oocyte quality. Clinical case 3, could be considered illustrative of an advanced age conception, in which age-related changes might have had an impact on oocyte quality. This type of patient would typically be recommended ART. However, given her profile and with two previous births, it was considered that supplementation with Ovosicare® Fertility, while considering other options, would represent an advantage for this patient. It would be valuable to have new prospective studies evaluating the effect of this food supplement on hormonal profiles and oocyte quality in the general population to confirm this hypothesis.
Importantly, aging is also associated with increased production of reactive oxygen species (ROS), which take part in the ovulation process and regulation of follicular maturation [46-48]. However, an excess of ROS contributes to the progressive loss of fertility [46,47]. After 32 years of age, there is progressive ovarian aging due to the mitochondrial accumulation oxidative stress-related damage [49,50], which also has an impact on oocyte quality, increasing the number of chromosomic alterations and aneuploids, all these changes being related to subfertility problems [51,52]. The clinical cases described here are representative of the current trend in developed countries to delay childbearing [2], hence being a population with increased oxidative stress damage [47]. In all these cases, patients were supplemented with Ovosicare® Fertility, a food supplement that includes different antioxidants such as melatonin, which has scavenger activity against ROS, increasing the oocyte quality. Moreover, melatonin has been shown to increase the expression of certain genes such as superoxide dismutase 2 which neutralises the ROS, protecting against mitochondrial oxidative damage and age-induced fertility decline [53]. Ovosicare® Fertility also contains pomegranate extract (Pomanox®) which is a well-known antioxidant. It has been described that polyphenols present in the pomegranate extract have scavenger activity that can have a beneficial effect in preventing ovarian oxidative stress [54,55]. Importantly, numerous reports have shown a relationship between increased ROS and inflammatory factors such as IL1-β, which are intimately linked to ovarian aging [56,57]. Some studies have shown that pomegranate extract can effectively hamper the activity of inflammatory factors such as IL1-β [58]. Altogether, supporting the potential beneficial effect of antioxidant supplementation in women older than 35 seeking pregnancy.
Furthermore, the food supplement prescribed to these patients also contains other relevant supplements such as folic acid and vitamin D. Numerous medical guidelines recommend starting the supplementation with folic acid at least 4 weeks before gestation. Thus, if the patients present a hypofunction of the enzyme methyl tetrahydrofolate reductase (MTHFR) (generally due to a mutation, which is present in up to 70% of the population in some areas of Europe), the active form present in this food supplement (5-methyl-tetrahydrofolate, Quadrefolic®) can be administered. Deficiencies in folic acid have been linked to increased obstetric and gynecological morbidity such as defects in the neural tube [59]. Lastly, supplementation with vitamin D, present in the formula, is particularly relevant as a deficiency in vitamin D is found in up to 80% of the total population, pointing to the need to assess its levels, especially in these women seeking a pregnancy [60] as it has been described to contribute to the embryo implantation [61].
To summarize, this series of clinical cases represent a frequent female profile in fertility clinics in developed countries; women over 35-years-old with gestational desire, who in general have no risk factors other than age. In all these cases, a natural pregnancy was achieved after supplementation with a specific ratio of 3.6:1 MYO:DCI food supplement containing, antioxidants, vitamins, and minerals which addresses some of the main factors undermining female fertility in this type of patient. This preliminary data points towards the effectiveness of these food supplements in women over 35-years-old with gestational desire. However, new clinical studies are needed to confirm this data and unleashed the potential of this new tool.
The authors declare that they have no conflicts of interest.
All authors have contributed equally to the work.