Synchronous detection of different types of cancer at the pelvic level is a rare finding. Due to its low incidence, the actual knowledge of this disease is difficult since it is based on articles published on small series of cases. We present the clinical, surgical, and anatomopathological findings of a patient with a synchronous endometrial cancer with a colorectal cancer.
Synchronous cancer, Pelvic synchronous cancer, Endometrial cancer, Colorectal cancer
Synchronous detection of different types of pelvic cancer in women is a rare finding in gynecologic oncology. Synchronous primary tumors are those that occur in the same subject simultaneously or in less than 6 months after the surgery of a first tumor.
For two tumors to be classified as synchronous, they must meet the following criteria: [1-5]
- It must be excluded that one tumor is metastasis of the other.
- There must be definite patterns of malignancy with different histology and absence of histological signs that indicate tumor invasion of one cancer in the seat organ of the other.
- There must be aneuploidies or karyotypes with different genetic abnormalities.
The description of multiple primary cancer dates from the late nineteenth century when Warren and Gates established anatomo-clinical criteria for diagnosis. The frequency of clinical presentation is 1.5% to 5.4% of all cancers. In recent years, there has been an increase in early diagnoses of second tumors, perhaps due to better staging, patient follow-up and better prognosis of the disease since the diagnosis of the primary tumor. [2,6]
Endometrial cancer is the third cause of cancer death in women of the Spanish population and the third in incidence after breast cancer and colon cancer. Women, who have endometrial cancer, have a 1.5-3 times higher risk of colon cancer [6-8]. An analysis, conducted by David, et al., has shown that endometrial cancer, in women under 50 years of age and ovarian cancer, in women under 60, should be considered as high-risk factors for developing colorectal cancer, their risk is similar magnitude if they had a first-degree familiar affected by colon cancer [7].
Below, there is an unusual case of a synchronous endometrial cancer with rectal cancer.
A 67-year-old female patient with no family history of cancer. Morbid obesity, with a body mass index of 45, and associated type-II diabetes mellitus. After consulting for a metrorrhagia in the postmenopause age, a diagnostic hysteroscopy is performed with resection of an endometrial polyp whose pathological anatomy reports well differentiated endometrioid adenocarcinoma. The scan’s study reports a stage IA endometrial cancer of the FIGO (International Federation of Gynecology and Obstetrics) and, in turn, a neoformation of the distal rectum that extends to the anal canal, of predominantly right anterior and no infiltration, that is biopsied with a anatomopathological diagnosis of adenocarcinoma of the rectum (pT2N0) The tumor cells show an intense expression of CK 20 and do not express CK7 this immunohistochemistry’s profile suggests a primary intestinal origin (Figure 1).
 Figure 1: Transversal section of CT showing the rectal tumor.
View Figure 1
Figure 1: Transversal section of CT showing the rectal tumor.
View Figure 1
With the diagnosis of endometrial adenocarcinoma on endometrial polyp and synchronous rectum adenocarcinoma is surgically intervened. A hysterectomy is performed with bilateral adnexectomy and an abdominoperineal amputation. It is accessed laparoscopically, showing an enlarged uterus and a tumor in the posterior region of the rectal ampulla. The recto-sigma release is performed up to the level of the elevator muscles, mesenteric vessel ligation and ruled hysterectomy with ligature of the pedicles of the uterine and ovarian arteries and colostomy in the left vacuum.
In a second surgical time in prone (Figure 2), the perineum was opened with extraction of rectum-sigma and mesh implantation in perineal orifice (Figure 3).
 Figure 2: Patient in prone and perianal incision.
View Figure 2
Figure 2: Patient in prone and perianal incision.
View Figure 2
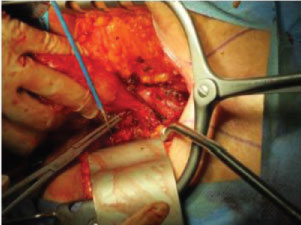 Figure 3: Perineal Opening with recto-sigma extraction.
View Figure 3
Figure 3: Perineal Opening with recto-sigma extraction.
View Figure 3
The final pathological anatomy of the piece confirms the previous diagnosis and discards the genetic component of the synchronous appearance of both tumors at the pelvic level.
Synchronic gynecological pelvic cancers are statistically infrequent in the oncological casuistry of any hospital and the cases reported in the literature are limited.
The case described was classified as a synchronous cancer of the endometrium and rectum due to the differences in the pathological anatomy-immunohistochemistry of the tumors. Also, emphasize the importance of image tests after the diagnosis of the first cancer, which was the endometrial one, since without them we would not have noticed the second neoplasia.
Although infrequent, these synchronous tumors must be taken into account so that they do not go unnoticed, especially in patients with risk factors like family cancer history or carriers of some genetic syndromes.