Membranous Dysmenorrhoea is defined as sudden sloughing of thickened endometrium as a whole with the shape of the uterine cavity, which may be associated with severe abdominal cramping. Although not rare, there are few cases described. It's more common in young females who were on either combined or progesterone only contraceptive pill, causing the decidualization of the endometrium. Due to its similarities to a gestational sac, miscarriage is the main differential diagnosis.
The authors report a case of a 43-year-old woman under no hormonal medication presenting her first episode of Membranous Dysmenorrhea with no other symptoms besides the loss of decidual cast.
Decidual cast, Membranous dysmenorrhoea, Progesterone
MD: Membranous Dysmenorrhoea
A 43-year-old woman who came to emergency department because of a sudden genital passage of a heterogeneous mass during the expected time for menstrual bleeding.
The patient had had 5 previous pregnancies with 5 term vaginal deliveries, she had been previously submitted to female laparoscopic tubal ligation, she had no relevant past medical records or chronic medication and had regular menses. For more than 5 years she had not been under any hormonal medication.
This was the first episode and the patient had no symptoms other than a sudden loss of a heterogeneous mass with 45 × 58 mm resembling a gestational sac, with the shape of the uterine cavity (Figure 1 and Figure 2).
 Figure 1: Decidual cast with the shape of the uterine cavity, resembling a gestational sac.
View Figure 1
Figure 1: Decidual cast with the shape of the uterine cavity, resembling a gestational sac.
View Figure 1
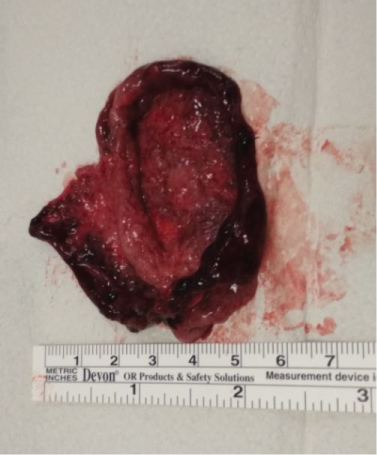 Figure 2: Decidual cast with the shape of the uterine cavity, resembling a gestational sac.
View Figure 2
Figure 2: Decidual cast with the shape of the uterine cavity, resembling a gestational sac.
View Figure 2
Transvaginal ultrasound showed empty uterine cavity, thin endometrium and no adnexal masses. Urine pregnancy test came negative. The patient was discharged and a medical appointment was scheduled 3 weeks later. The patient remained asymptomatic. Histological examination of the product revealed an endometrium with exacerbated decidualization of the stroma and vascular congestion (Figure 3).
 Figure 3: Microscopic examination revealing endometrium with exacerbated decidualization of the stroma and vascular congestion (A - 40x magnification; B - 400x magnification).
View Figure 3
Figure 3: Microscopic examination revealing endometrium with exacerbated decidualization of the stroma and vascular congestion (A - 40x magnification; B - 400x magnification).
View Figure 3
This is case of an atypical presentation of Membranous Dysmenorrhoea (MD). Membranous Dysmenorrhoea, or passage of decidual cast is a rare event defined as sudden sloughing of thick endometrium as a whole with the shape of the uterine cavity, which may be associated with severe abdominal cramping, thus the name Dysmenorrhoea. There are few cases described, the great majority were in adolescents or young female adults who were on either combined or progesterone only contraceptive pill [1-4]. Its exact pathophysiology is unknown. It is believed to be related to the use of exogenous progesterone, as this hormone is the primary decidualizing factor of the endometrium [5]. The usual clinical presentation is loss of decidual cast, which may resemble a gestational sac, so miscarriage must always be excluded. Other causes of tissue passed per vagina include polyps and neoplasms. In young girls, fibroepithelial polyps and sarcoma botryoides are the most common [6,7].
If the patient is seen before expulsion, at ultrasound there may be a heterogeneous mass resembling a polypoid intrauterine lesion [8], but usually women search medical care afraid of a miscarriage because of the unusual vaginal loss with the shape of the uterus, similar to a gestational sac. The diagnosis may be confirmed after histological examination and a negative pregnancy test.
Membranous Dysmenorrhoea is self-limited so no treatment is required besides adequate analgesia. As benign entity, women must be reassured and advised that it may recur [9].
This patient presented with a sudden genital passage of a heterogeneous mass resembling a gestational sac, but there was no pain which is characteristic. Also, the patient was in her 40's while MD is quite more common during adolescence and young females. MD is caused by exacerbated decidualization, which is produced by the effect of progesterone. Our patient was not under any kind of hormonal medication, so the decidualization was caused by endogenous progesterone of her natural cycle.
The importance of this case relies on the call of health professional's attention to this entity, although quite common, there are quite few reports in international literature. Most of the women think they are suffering a miscarriage, which indeed is its main differential diagnosis, thus the importance of the pregnancy. Once the patient is reassured that she is not pregnant, and if bleeding and pain are controlled, there is no need for additional measures and the presumptive diagnosis of MD must be considered. Histological examination confirms the diagnosis.
Membranous Dysmenorrhea is defined as sudden sloughing of thickened endometrium as a whole with the shape of the uterine cavity, resembling a gestational sac. Despite its high frequency, health professionals may not be aware of this entity. Classically described in adolescents and young women, it may affect any women in reproductive age. Although usually associated with progesterone only or combined pill, it may occur in non-medicated women. Despite its name, it may happen without pain. After excluding a miscarriage, patients' pain and bleeding must be controlled and histological examination may confirm the diagnosis.
The authors thank Dr. Jennifer Costa from LAP - Laboratório de Anatomia Patológica - for performing the histological examination and providing the microscopy pictures.
The authors report no conflict of interest.