Giant ovarian tumours are rare nowadays due to early recognition of these tumours in clinical practice. Management of these tumours depends on age of the patient, size of the mass and its histopathology. We are reporting a rare case of torsion of hemorrhagic ovarian cyst presented to us with acute abdomen. 22-year-old, unmarried girl came to our outpatient department with complaints of lower abdominal pain for 3 days. Patient was apparently normal before 3 days after which she developed lower abdominal pain which was spasmodic in nature more on the right side. The abdominal pain was progressive, non-radiating aggravated on routine activities and relieved with analgesics. Patient also had history of vomiting 3 to 4 episodes per day for the past 2 days. Abdominal examination showed distension of lower abdomen with tenderness over right iliac region. Cystic mass 5*5 cm felt on palpation which was extending from iliac region to hypogastrium with ill defined borders. Bed side ultrasound abdomen and pelvis showed two right adnexal hemorrhagic cystic masses of size 8.4*5.3*5.2 cm and 5.2*4.1*3 cm respectively without vascularity in doppler study. Right ovary could not be visualized separately. With clinical suspicion of torsion, MRI pelvis was done immediately which confirmed torsion of cysts. Patient was posted for emergency laparotomy. Two huge hemorrhagic mass of size 8*6 cm and 5*3 cm was identified on the ride side of uterus which was necrotic and gangrenous. Right ovary could not be visualized seperately. The hemorrhagic ovarian cysts had undergone torsion. Detorsion of the cyst was done. As there was no evidence of viability, cystectomy followed by right salphingo oophorectomy was done.
Giant ovarian tumours are rare nowadays due to early recognition of these tumours in clinical practice. Management of these tumours depends on age of the patient, size of the mass and its histopathology [1]. Large ovarian masses also cause psycho-social stress due to fear of malignancy among the patients. Large ovarian masses cause compressive symptoms on Urinary, respiratory and gastro-intestinal tract. So an ideal comprehensive approach to the management of these mammoth ovarian tumors is much needed to ameliorate the secondary effects along with the primary treatment [2].
Here, we are reporting a rare case of torsion of hemorrhagic ovarian cyst presented to us with acute abdomen.
22-year-old unmarried girl came to our outpatient department with complaints of lower abdominal pain for 3 days. Patient was apparently normal before 3 days after which she developed lower abdominal pain which was spasmodic in nature more on the right side. The abdominal pain was progressive, non-radiating aggravated on routine activities and relieved with analgesics. Patient also had history of vomiting 3 to 4 episodes per day for the past 2 days. She had regular menstrual cycles. No significant past illness.
On examination,
Patient was conscious, oriented, afebrile.
Vitals
• Temp: Normal
• Pulse rate: 76 bpm
• Blood pressure: 100/70 mmHg
• Respiratory Rate: 16/min
Abdominal examination showed distension of lower abdomen with tenderness over right iliac region. Cystic mass 5*5 cm felt on palpation which was extending from iliac region to hypogastrium with ill defined borders. A Tender right adenexal mass was felt, on per rectal examination (Figure 1).
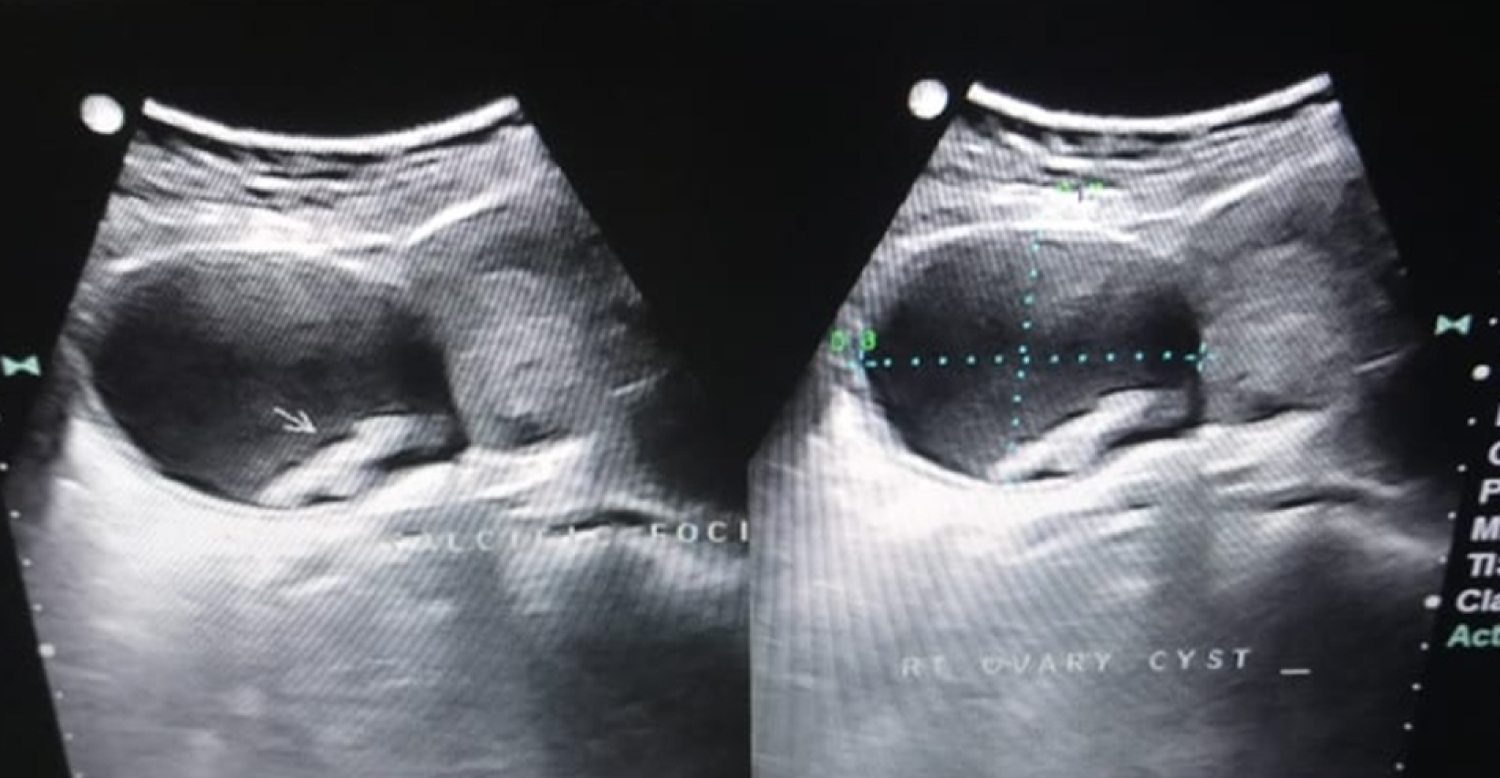 Figure 1: USG pelvis showed Right hemorrhagic ovarian cysts.
View Figure 1
Figure 1: USG pelvis showed Right hemorrhagic ovarian cysts.
View Figure 1
Routine blood investigations (Complete blood count, Liver and renal function tests) were within normal limits. Bed side ultrasound abdomen and pelvis showed two right adenexal hemorrhagic cystic masses of size 8.4 *5.3*5.2 cm and 5.2*4.1*3 cm respectively without vascularity in doppler study. Right ovary could not be visualised separately. Left adenexa was normal. With clinical suspicion of torsion, MRI pelvis was done immediately which confirmed torsion of cysts (Figure 2).
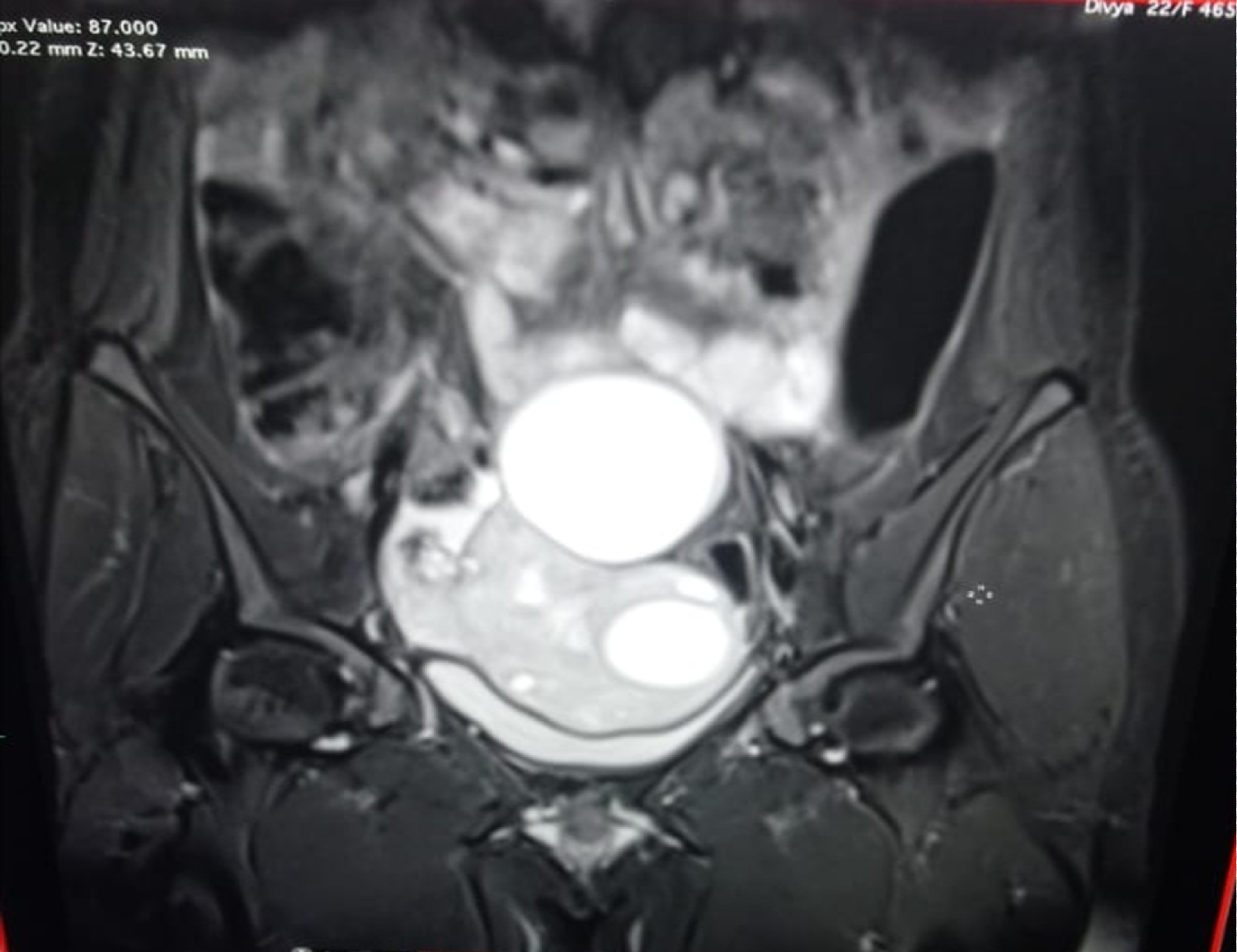 Figure 2: MRI pelvis: Two Hemorrhagic ovarian cysts with features suggestive of Torsion.
View Figure 2
Figure 2: MRI pelvis: Two Hemorrhagic ovarian cysts with features suggestive of Torsion.
View Figure 2
Patient was posted for emergency laparotomy. Under general anaesthesia, laparotomy was proceeded with suprapubic transverse incision. Two huge hemorrhagic mass of size 8*6 cm and 5*3 cm was identified on the ride side of uterus which was necrotic and gangrenous. Right ovary could not be visualised seperately. The hemorrhagic ovarian cysts had undergone torsion. Detorsion of the cyst was done. As there was no evidence of viability, cystectomy followed by right salphingo oophorectomy was done.
Post-operative period was uneventful. Patient was discharged with advice to follow up. Histopathology of excised cyst showed right sided simple haemorrhagic cyst with necrosed ovarian tissue and fallopian tube (Figure 3).
 Figure 3: Haemorrhagic Ovarian cysts with Gangrenous fallopian tubes.
View Figure 3
Figure 3: Haemorrhagic Ovarian cysts with Gangrenous fallopian tubes.
View Figure 3
Hemorrhagic ovarian cyst (HOC) is an adnexal mass formed because of bleeding into a follicular or corpus luteum cyst or a theca lutein cyst. Most of HOCs are functional, few of them can be neoplastic but they are universally benign. Mostly seen in young women of reproductive age group though also reported rarely in perimenopausal women [3]. HOCs typically develops in ovulating women.
Secondary to hormonal response, the stromal cells surrounding a maturing Graafian follicle become more vascular and after the oocyte has been expelled, the Graafian follicle develops into a corpus luteum with a highly vascular and fragile granulosa layer, which ruptures easily, forming hemorrhagic ovarian cysts (HOCs).
Ovarian torsion is considered as one of the complication of large ovarian cysts. Ovarian torsion in women can present as acute abdomen in the emergency room. Rapid diagnosis is often needed to retain the tubo-ovarian function and to avoid significant morbidity and mortality [4]. There may be partial or complete rotation of adenexa with associated ischemia. Ovarian torsion is usually seen in 2%-15% of patients who had previous surgeries for adnexal masses [4]. It presents with acute onset of pelvic pain, followed by nausea and vomiting.
Torsion of ovary is considered as a gynecological emergency [5-7]. Torsions more commonly involve both the ovary and fallopian tube, and there are fewer cases of isolated torsion involving either one (one in 1.5 million women) [8-10].
Nearly 80% of patients with torsion ovary had ovarian masses of 5 cm or larger [11,12]. The sizes of ovarian masses are correlated with the risk of the torsion. However, Ovarian torsion can occur with any masses with size ranging from1 to 30 cm (mean 9.5 cm) [13]. Large follicular cysts as result of ovulation induction in infertility treatment may carry an increased risk for torsion [14].
In ultrasonography a torsed ovary may be rounded and enlarged compared with the contralateral ovary, because of edema or vascular and lymph engorgement [15,16]. Whirlpool sign is highly sensitive for ovarian torsion [17,18]. The whirlpool sign shows a twisted vascular pedicle, and a Doppler sonogram reveals circular vessels within the mass.
Ultrasound is considered the cornerstone in the diagnosis of HOCs irrespective of the clinical condition of the patients often misdiagnosed due to their variable sonographic appearance, mimicking other organic adnexal masses like dermoid.
Sonographic morphological patterns of hemorrhagic ovarian cysts (HOC)
1. Thin wall,
2. The internal echogram shows diffuse solid pattern,
3. The internal echogram shows mixed cystic and solid pattern,
4. The internal echogram shows a sponge-like pattern (lace like reticular pattern),
5. Color Doppler of HOC shows peripheral or circumferential blood flow in the cyst wall typical. Clot may adhere to the cyst wall mimicking a nodule, but has no blood flow on Doppler imaging retracting clot may have sharp or concave borders.
Magnetic resonance imaging (MRI) can be used to diagnose torsion if findings on ultrasound are equivocal [19-23]. MRI can demonstrate the components of a mass in more detail than an ultrasound. Pelvic MRI may be performed to confirm the diagnosis.
Signal characteristics can vary depending on the age of the haemorrhage.
T1: high signal
T2: high signal
"T2 shading" is suggestive of chronic blood products and is more typical of endometrioma.
A laparoscopic approach has become a popular procedure for ovarian cysts. However, if cancer of the ovary or fallopian tube is suspected, a laparotomy should be done [24].
Once ovarian torsion is suspected, surgery or detorsion is the mainstay of treatment.
The following are the risk factors of developing torsion ovarian cysts
1. Cyst more than 5 cm
2. Elongated infundibulopelvic ligaments
3. Premenarchal girls and postmenopausal women
4. Ovarian cyst along with pregnancy
Most of Hemorrhagic ovarian cysts disappear spontaneously with follow-up. Only conservative treatment with analgesics and anti-inflammatory is needed. Follow up with USG is done once in 3 months. Surgical intervention is required in HOC > 5 cms, intractable pain (Rupture, Hemorrhage, Torsion), leukocytosis and anemia.
Thus torsion of ovarian cysts usually present with acute abdomen but occasionally presentation may be a typical which leads to significant delay in its diagnosis. Hence, a high level of clinical suspicion is often needed to prevent morbidity and mortality.
Nil.