• Uterine fibroids are benign smooth muscle tumours of the uterus.
• Its prevalence during pregnancy has been reported to be 1-4% [1].
• Pregnancy along with a fibroid is a high risk pregnancy which may lead to complication with unequal gravity.
• Their presence has been linked to spontaneous abortion, intrauterine growth restriction (IUGR), anemia, multiple blood transfusions, infection, pain, degeneration, malposition of foetus, premature labour, uterine inertia, placental abruption, postpartum hemorrhage, retention of the placenta, increased rates of cesarean section, hysterotomy, obstetric hysterectomy [2-6].
• We present a case report of a patient with pregnancy with multilobulated fibroid (subserosal) (broad-based, not pedunculated) occupying whole lower uterine segment.
• Details of patient and challenges faced -
Age - 30 years
Obstetric history - Married since 1 and half years; Spontaneous Conception
• Patient was diagnosed fibroid with pregnancy at 8 weeks of gestation with MRI suggestive of huge subserosal multilobulated fibroid arising from anterior wall of uterus extending in abdomen up to epigastric region, total mass measuring 10 × 19 × 23 cm with areas of degeneration (cystic).
• Anteriorly, it reaches up to anterior abdominal wall, postero-superiorly pressing over retroperitoneum causing mass effect over aorta & IVC postero-inferiorly causing mass effect over endometrial cavity, inferiorly causing mass effect over urinary bladder.
• At her town place, primarily she was advised termination. She was also explained regarding need of myomectomy after MTP and SOS chances of hystrectomy. But she wanted to continue the pregnancy.
• She presented to us at 22 weeks of gestation after anomaly scan, which was normal, with maternal weight 34 kg.
• Routine obstetric care given.
• Patient presented with pain in abdomen at 24 weeks of gestation. USG done and was found normal. Size of multilobulated fibroid being 13 cm and 10 cm respectively, extending into lower uterine segment.
• Complete blood count and CRP done which was suggestive of infection. Conservative management with IV antibiotics. We counselled her regarding need of conservative management till viable age of fetus.
• After 3 weeks (at 27 weeks), patient was posted for cesarean section due to persistent complaint of pain in abdomen and discomfort.
• 2 units of blood transfused.
• A high risk informed consent with arrangement of multiple blood products and SOS chances of cesarean hystrectomy, chances of ICU admission and fetal risk were explained.
• MRI done which showed mass of 14.5 × 12.8 × 24 cm arising from anterior wall of uterus, displacing it to right half of abdomen, extending in abdomen up to epigastric region, inferiorly displacing the urinary bladder.
• Under spinal anesthesia, right para-median vertical skin incision was given. Mass was multilobulated occupying entire anterior surface of the uterus.
• Manipulation of the mass was done in order to find the space for the incision.
• Entire anterior surface of the uterus was occupied by the mass except a long 4-5 cm strip like area on right lateral wall just below the round ligament.
• Vertical incision was taken on the mass free area.
• As the cavity was not reached, finger was inserted, amniotic sac palpated and ruptured with long artery forceps.
• Baby delivered with the help of fundal pressure. (Weight of the baby - 1.1 kg). Baby cried immediately after birth.
• Bilateral uterine artery ligation done.
• Myomectomy done. Fibroid of 2.4 kg removed.
• 2 units of blood transfused.
• Hemorrhage was within manageable limits and a cesarean hystrectomy was avoided.
• Baby was on ventillator after birth, weaned off on day 8 of life and was continued on RT feed.
• She had an uneventful post-op recovery.
• The histopathology of fibroid showed hyaline degeneration without mitotic figures.
• Barrier method was advised strictly for 3 years (Figure 1, Figure 2 and Figure 3).
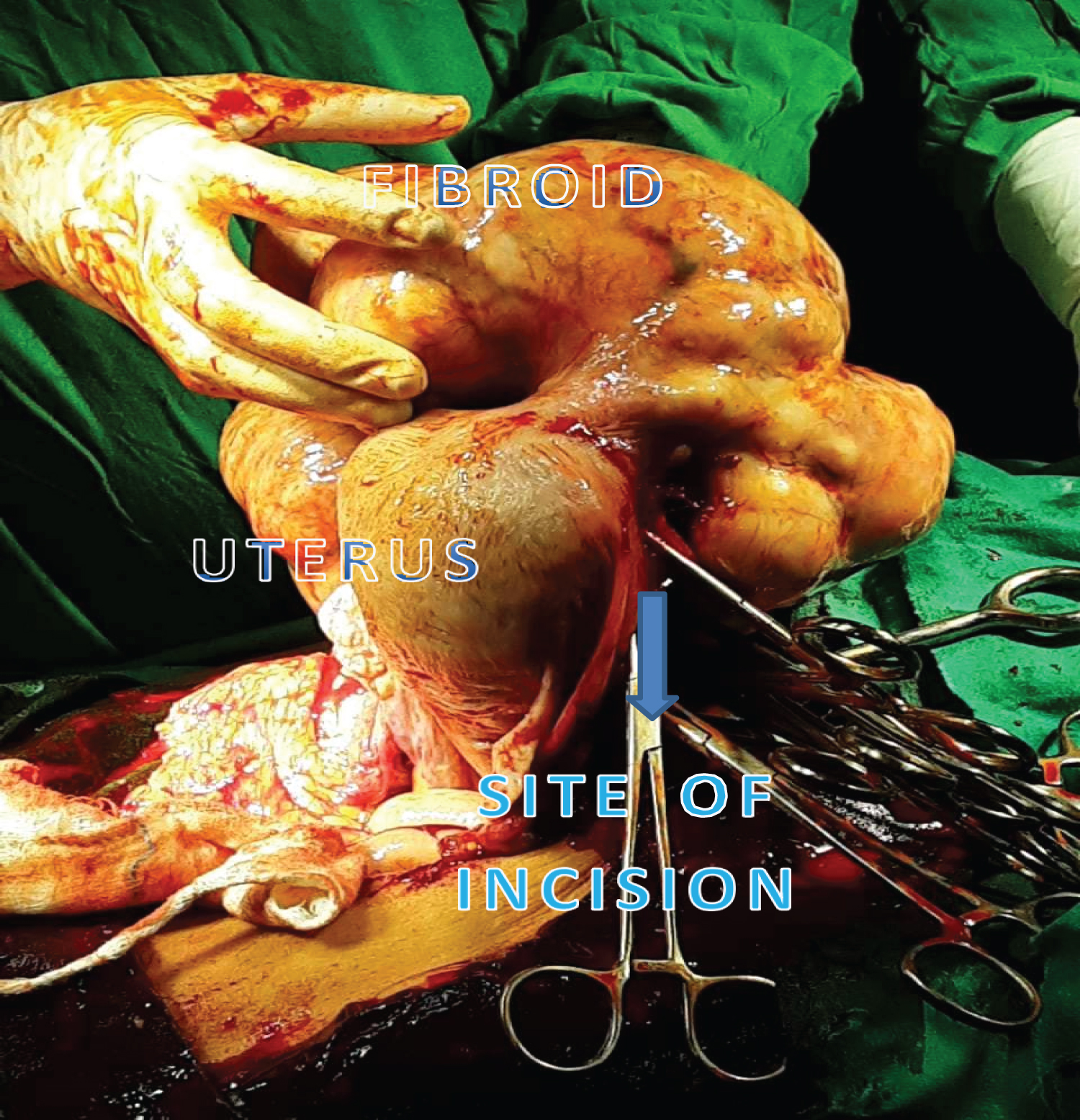 Figure 1: Uterus with fibroid after delivery of baby - vertical uterine incision taken. View Figure 1
Figure 1: Uterus with fibroid after delivery of baby - vertical uterine incision taken. View Figure 1
 Figure 2: Uterus after myomectomy and bilateral uterine ligation. View Figure 2
Figure 2: Uterus after myomectomy and bilateral uterine ligation. View Figure 2
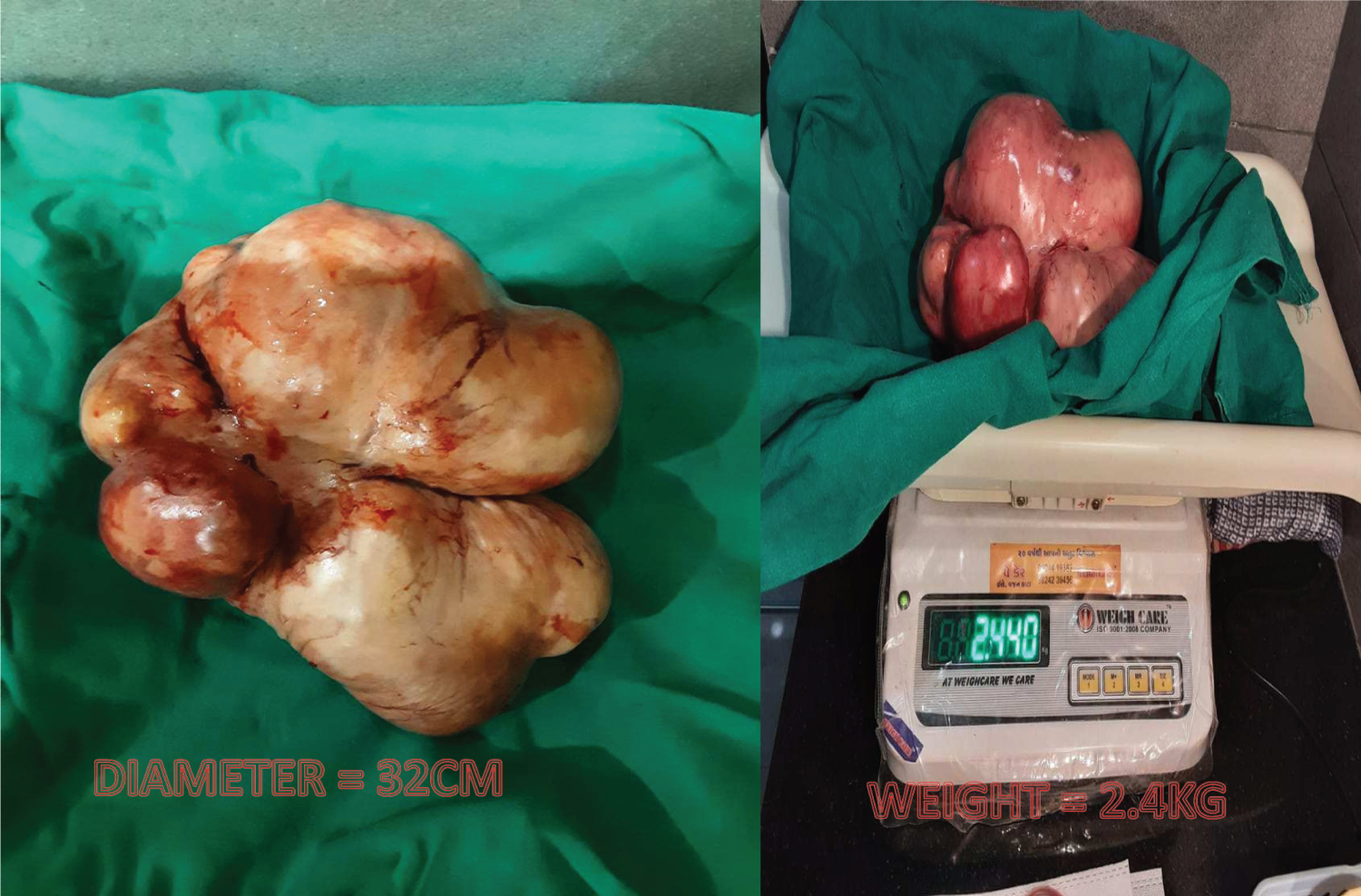 Figure 3: Fibroid with diameter and weight. View Figure 3
Figure 3: Fibroid with diameter and weight. View Figure 3
• The relationship of fibroids and adverse outcomes in pregnancy are not clearly understood [7].
• Mostly the fibroids are asymptomatic with only 9% of large fibroids showing any symptoms; mainly lower abdominal pain in the 2nd or 3rd trimester s suggestive of red degeneration.
• Vice versa around 10-30% fibroids have complications in pregnancy [8].
• Early miscarriages are more common with multiple fibroids [9,10].
• The risk of preterm labour is significantly increased with both multiple fibroids and with large fibroids (> 5 cm) [11].
• Multiple fibroids especially lower uterine segment increase chances of cesarean section [12,13].
• Blood loss at delivery is increased for fibroids > 5 cm.
• Myomectomy at the time of cesarean delivery causes severe hemorrhage and should be reserved only for subserous, pedunculated fibroids. However cesarean myomectomy with fibroids > 5 cm size in experienced hands in tertiary care centres with stepwise de-vascularisation has been found relatively safe [14-17].
• In this case, patient was unaware of fibroid before conception. It turned out to be a wise decision to continue her pregnancy as we were able to wait till weight of the baby reached 1 kg.
• Dilemmas in decision making-
1. Whether to continue pregnancy or to terminate the pregnancy and to do interval myomectomy pre-conception.
2. Whether to go for cesarean myomectomy or not. Subserosal, especially pedunculated, are definitely to be removed. For intramural fibroids, decision depends on surgical skill, location of the fibroid, size of the fibroid, availability of the infrastructure, blood and blood products, expert assisstants and intensive care.
1. Proper counselling of the patient and her relatives.
2. Co-operation on patient's side.
3. Dedicated team of gynecologist + physician + paediatrician + anesthetist.
4. Availability of blood and blood products.
5. Post operative care.
6. NICU care.
7. Strict contraception by barrier method in order to maintain adequate spacing and prevention of rupture of scar and uterus.