Objective: The purpose of this paper is to present the case of a pregnant woman with diagnosis of Buschke-Löwenstein tumor at the beginning of labor, exposing the management and performing a review of the literature on the matter.
Case report: A pregnant woman in the 37th week of gestation diagnosed with Buschke-Löwenstein tumor at the time of the delivery. Her medical history did not reveal any characteristics. Due to the predominantly perineal spread, with no warts in the vagina or birth canal, the labor progress was allowed and followed by a normal delivery with no further complications. Two months after delivery, a spontaneous partial reduction of the warts was observed; nevertheless, a surgical treatment was performed. There have not been any recurrence signs during postoperative six-month follow-up period. There have not been clinical evidences of laryngeal papillomatosis in the infant, although at the moment the patient is under surveillance.
Conclusion: The diagnosis of Buschke-Löwenstein tumor during pregnancy must not contraindicate the vaginal birth on its own, unless there are other contraindications. If the tumor can cause an obstruction of the birth canal, it is advisable to assess a surgical treatment during the pregnancy, prioritizing minimally invasive procedures due to the favorable development of the tumor after the pregnancy.
Buschke-Löwenstein tumor, Delivery, Giant condyloma acuminatum, Pregnancy
Condylomata acuminata are a type of verrucous injuries that affect the genital area, caused by serotypes of human papillomavirus (HPV) considered of low-risk oncogenic potential (types 6 and 11 in 95% of the cases). HPV infection is one of the most prevalent sexually transmitted diseases, affecting 14.3% of sexually active women in Spain [1]. Regarding genital warts, the prevalence is substantially lower (0.15-1.18%), although this percentage could be underestimated since it is not a notifiable disease [2]. HPV infection involves an important psychosocial, health and economic impact [3].
The genital warts behavior is variable, from a spontaneous resolution to a stable maintenance of the lesions or to a striking progression and growth. One of the clinical presentations of the disease corresponds to the latter and it is called giant condyloma acuminatum or Buschke-Löwenstein tumor. This disease was described for the first time in 1925, and it affects approximately to 0.1% of general population [4]. It is characterized by a fast and invasive growth, with important recurrence after treatment [5]. Immunodepressed patients are more affected by condylomata acuminata. Physiological immunodepression states, such as pregnancy, favor the warts progression especially as gestational age increases [2].
The purpose of this paper is to present the case of a pregnant woman with diagnosis of Buschke-Löwenstein tumor at the beginning of labor, exposing the management and performing a review of the literature on the matter.
A 23-year-old pregnant woman (on her second pregnancy after a previous normal delivery) from Guatemala went to the Emergency Services of our center due to spontaneous labor at the 37th week of gestation. She referred to an appropriate prenatal care according to her country's protocol and follow-up with expectant management of multiple condylomata acuminata in the genital area, not providing any documentation.
Blood test, serologies, vaginal and endocervical cultures were performed with negative results, therefore the existence of other concomitant sexually transmitted diseases was discarded. An obstetric ultrasound was performed, showing the fetus with cephalic presentation and without further findings of interest.
The physical examination showed the presence of a large and irregular exophytic papillomatous lesion with a maximum diameter of 17 cm, affecting the whole perianal region surpassing the anus, with the presence of multiple small satellite lesions in the inguinal and vulvar regions. The Bishop score was performed, showing the active phase of labor.
After applying epidural block anesthesia, the spread to the birth canal was more appropriately re-evaluated. The absence of lesions inside the vagina and the predominantly perianal spread were determining factors for the decision of allowing the evolution to a vaginal delivery. The pregnancy finalized with a normal delivery three hours after the patient's hospital admission (Figure 1). The infant was a female, weighted 3,360 grams, with an Apgar score of 9-10. Progress was favorable, with home discharge after 48 hours and subsequent clinical follow-up.
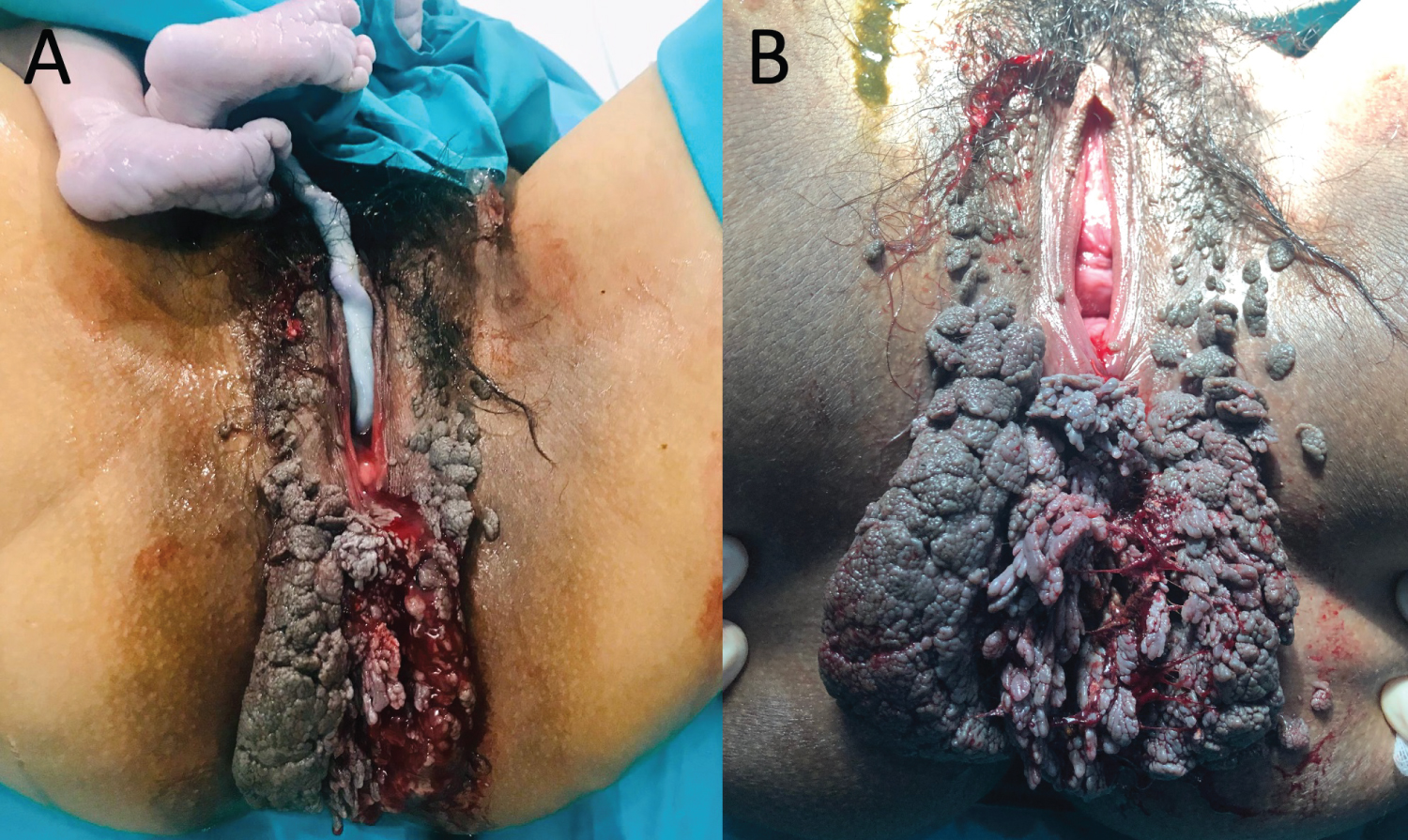 Figure 1: Buschke-Löwenstein tumor with a large perianal spread (A) First-degree tear on the posterior fourchette, without injuries on the tumor after the vaginal birth; (B) Stitching of first-degree perineal tear without complications.
View Figure 1
Figure 1: Buschke-Löwenstein tumor with a large perianal spread (A) First-degree tear on the posterior fourchette, without injuries on the tumor after the vaginal birth; (B) Stitching of first-degree perineal tear without complications.
View Figure 1
During the first follow-up visit (two months after delivery), it was observed that an important reduction in the size of the lesion had taken place spontaneously (Figure 2). One of the warts was taken for biopsy, which confirmed the diagnosis of condylomata acuminata presented as a Buschke-Löwenstein tumor. A cervical cytology was performed with negative result for malignancy and positive result for high-risk HPV (different from genotypes 16 and 18), and colposcopy study was normal.
 Figure 2: Clinical appearance of the tumor two months after delivery, without treatment.
View Figure 2
Figure 2: Clinical appearance of the tumor two months after delivery, without treatment.
View Figure 2
In spite of the spontaneous reduction of the global size of the tumor after delivery, since the main lesion was still present with some satellite lesions, surgical treatment was indicated. Four months after delivery, excision of all remaining warts was performed without complications. There were no evidence of recurrence of genital warts on the follow-up visits one and six months after the surgery (Figure 3).
 Figure 3: Six-month follow-up visit after surgery, with no evidence of recurrence.
View Figure 3
Figure 3: Six-month follow-up visit after surgery, with no evidence of recurrence.
View Figure 3
Regarding the infant progression, there have not been any complications on the parts of the upper airway that suggest the presence of laryngeal papillomatosis after one year of surveillance.
Buschke-Löwenstein tumor or giant condyloma acuminatum is a very rare disease, associated with HPV infection, that may appear particularly during pregnancy, such as the case on this paper. Physiological immunodepression associated with pregnancy and the increased viral replication, explain the susceptibility to progression of warts in pregnant women and the clinical presentation [2].
There is limited scientific evidence of pregnant women with this disease. To this date, only eight cases of Buschke-Löwenstein tumor have been published for this group [6-13].
Due to the tendency to growth and local invasion of tissues, one of the main problems is the possible spread to the birth canal, which conditions the mode of delivery decision [7]. The tumor spread must be assessed fully, mainly to the vaginal and perineal spread, but also to other organs - such as urethra or anus. The urethral spread is relatively common [7,8,10,11] and usually implies more spread and compromise of the birth canal. In these occasions, surgical treatment prior to the completion of the gestation may favor vaginal birth.
In four of the published cases, elective surgery was performed during the pregnancy [7-10]. Some options of treatment prior to delivery include the excision with cold [9] or thermal [8] scalpel, in order to unblock the birth canal and allow the vaginal delivery, as showed in Yavuzcan, et al. [8] after the complete excision of the warts with a harmonic scalpel. The main complication after this type of surgery is the appearance of stenosis caused by fibrotic tissue. Thus, the indication of surgical treatment must be assessed considering risks and benefits.
On the other four published cases, the completion of the gestation was performed via caesarean section [11-14], either since the tumor spread compromised the birth canal or/and the risk of bleeding due to the warts distribution. Tumor excision was performed to these patients at staggered times during postpartum.
After delivery, the natural progress is spontaneous regression of the tumor [7] which allows to perform less invasive surgical treatments.
Early diagnosis, as well as a proper clinical follow-up and multidisciplinary assessment of the patients, are key during pregnancy and delivery. If during the pregnancy, a lesion growth is identified, a stricter monitoring will be necessary in order to prevent an obstruction of the birth canal. Moreover, the spread to the posterior fourchette will have to be specially assessed, since the episiotomy or the appearance of small first-degree tears may cause a bigger problem due to the warts' high-risk of bleeding. In cases such as these, it is possible to previously identify the warts that may compromise the completion of gestation with vaginal birth, performing a selective excision of the affected lesions. Consequently, the risk of canal stenosis and bleeding of the warts is reduced at the delivery.
The mode of delivery (vaginal or abdominal) does not seem to influence the infection rates of the infant [15,16]. Although the transmission during delivery is possible, the highest risk factor for the development of laryngeal papillomatosis in the infant, is the exposition of the fetus to HPV during the pregnancy [2]. The infection is possible even during the postnatal period (breast feeding or close contact) [16].
Thus far, caesarian section has not been stablished as a protective factor to the development of laryngeal papillomatosis [15], therefore the vaginal birth should be the mode of delivery unless there are other contraindications. This would reduce maternal morbidity without increasing fetal morbidity or the risk of transmission.
Buschke-Löwenstein tumor diagnosis during pregnancy does not contraindicate vaginal birth on its own, which we recommend if there is not an obstruction of the birth canal or any other contraindications. If surgery is indicated, low invasive procedures are recommended, due to the favorable progress of the lesions after delivery.
The authors have no conflicts of interest relevant to this article.
All authors contributed equally.