Leiomyoma are the most common benign tumor of the reproductive tract in premenopausal women. Uterine artery embolization has been accepted as a minimally invasive option for the treatment of leiomyoma. While pelvic arterial embolization has shown promising safety and effectiveness in controlling postpartum hemorrhage, no studies have reviewed its clinical application for the prophylactic decrease of hemorrhage risk following minimally invasive therapies for fibroids. We present a case and discuss the utility of stepwise interventions for removing a prolapsing submucosal leiomyoma in a patient with complex pelvic arterial collateralization and significant risk for postprocedural hemorrhage.
Uterine artery embolization, Hysteroscopy, Myomectomy, Prolapsing leiomyoma, Hemorrhage, Complex pelvic arterial collateralization
A 40-year-old female was followed at our tertiary academic center with Cardiology and Pulmonary medicine teams for a complex cardiac history. Her history included complex aortic coarctation status post-surgical repair via left thoracotomy at two weeks of age followed by a revision with interposition Dacron graft placement at 4.5 years of age. She had known complex arch anatomy, abdominal coarctation, aberrant origin of the subclavian arteries, and occlusion of her femoral arteries. She had secondary pulmonary arterial hypertension improved symptomatically on pulmonary vasodilator therapy. Diagnosed with atrial flutter in 2017, she was placed on chronic anticoagulation with apixaban.
The patient presented to our outpatient Gynecology department with worsening abnormal uterine bleeding (AUB) and lower pelvic cramping. A 52 mg levonorgestrel-releasing intrauterine system (IUS) was placed in August 2018 for contraceptive coverage and management of her heavy vaginal bleeding (HVB). She reported amenorrhea following placement; however, she began to experience spotting and subsequent worsening to HVB over the previous four months. On examination in the office, the patient was noted to have significant blood in the vagina. The cervix was identified with a large protruding mass. The IUS strings were visible, and the anterior lip of the cervix was identifiable.
Magnetic resonance imaging (MRI) revealed an anteverted uterus measuring 5.0 × 7.5 × 10.7 cm. A 2.1 × 2.6 × 5.6 cm pedunculated intracavitary circumscribed mass (Figure 1) with a stalk was noted in the anterior lower uterine segment adjacent to the C-section scar and extended inferiorly through the cervical os. This mass's signal intensity was like background myometrium with homogeneous enhancement, no internal cystic foci, and a vascular stalk. The patient was also noted to have complex infrarenal arterial anatomy. Computed tomography (CT) angiogram (Figure 2), as well as MRI imaging (Figure 3), revealed stable diminutive caliber of the abdominal aorta (history of correction of aortic coarctation), stable appearance of infrarenal aortoiliac occlusion, extensive collateralization in the pelvis with reconstitution of the iliac arteries bilaterally, and extensive superior mesenteric artery to inferior mesenteric/epigastric territories collateralization.
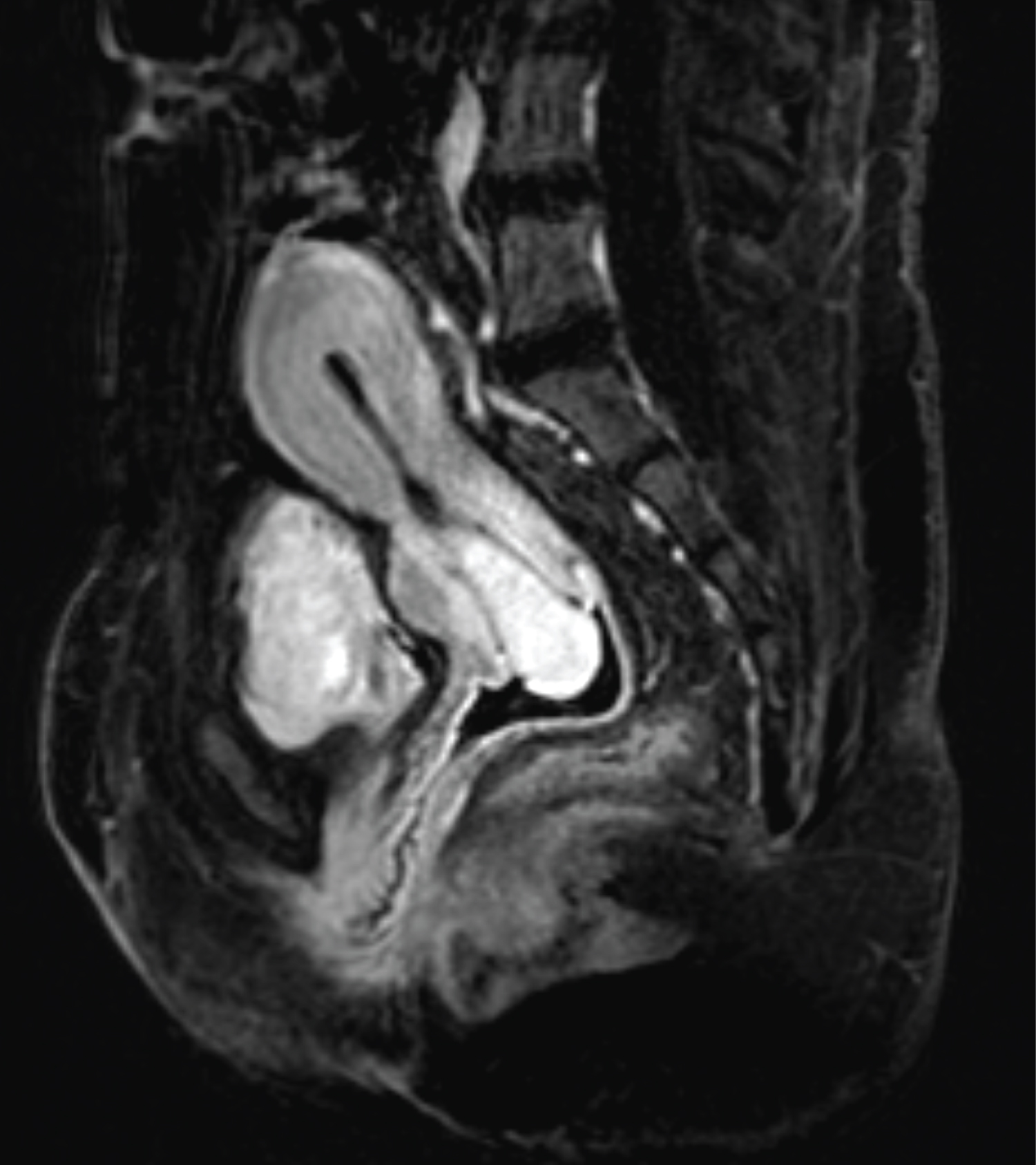 Figure 1: MRI of pedunculated intracavitary mass with vascular stalk.
View Figure 1
Figure 1: MRI of pedunculated intracavitary mass with vascular stalk.
View Figure 1
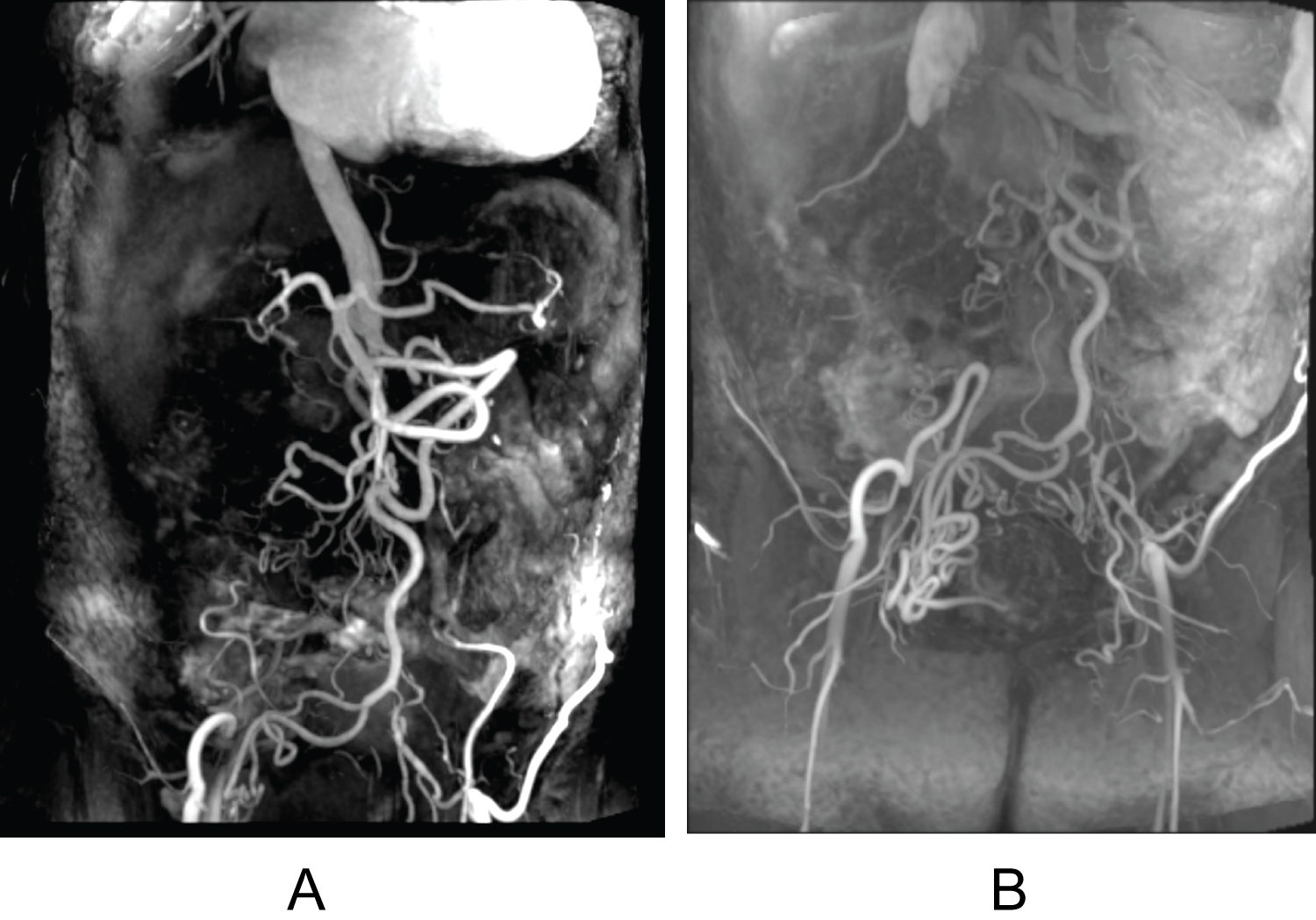 Figure 2: 3-D vascular reconstruction MRI of complex intrarenal arterial anatomy in patient with history of aortic coarctation.
View Figure 2
Figure 2: 3-D vascular reconstruction MRI of complex intrarenal arterial anatomy in patient with history of aortic coarctation.
View Figure 2
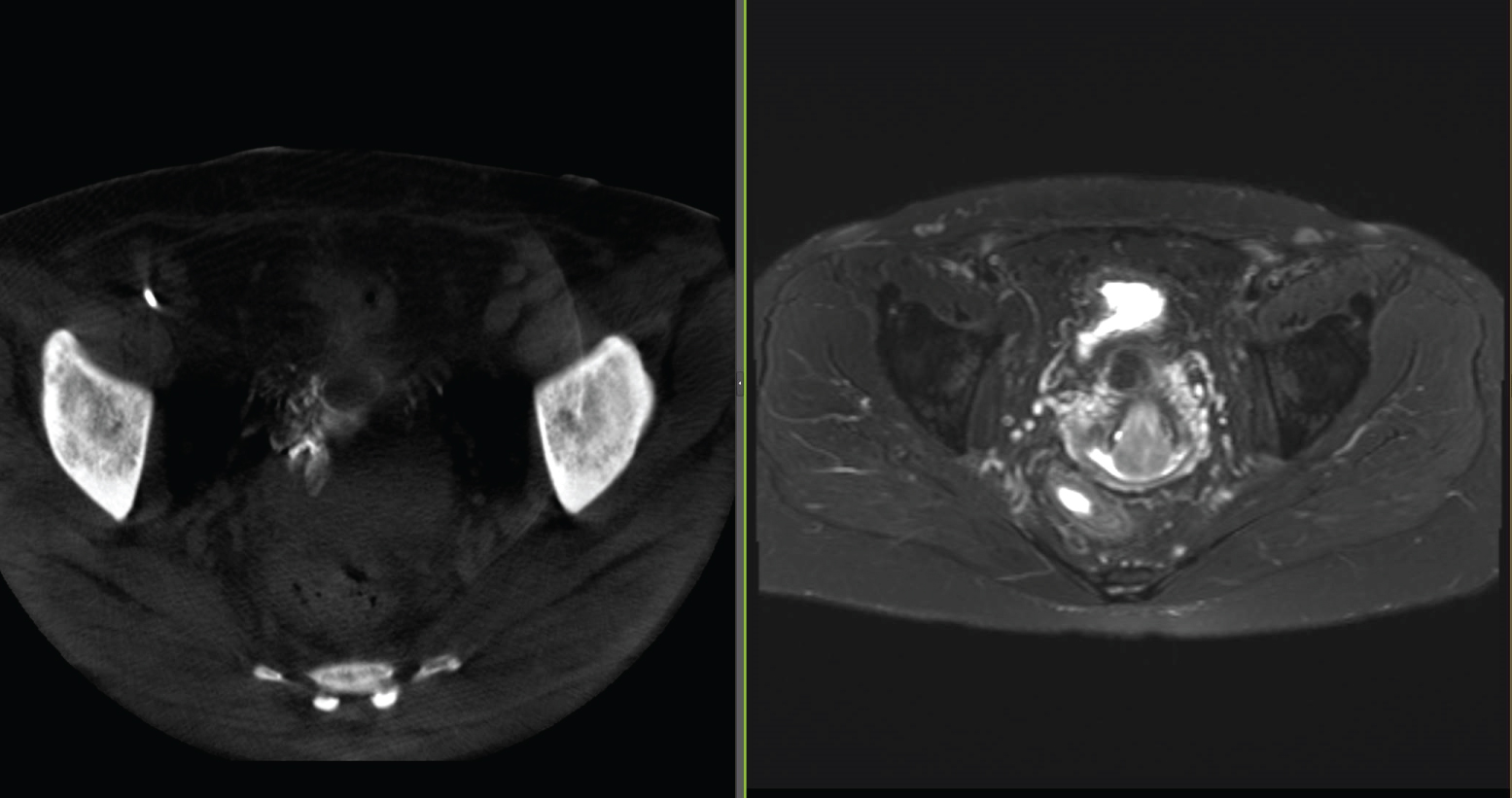 Figure 3: CT angiogram imaging with contrast showing infrarenal aortoiliac occlusion with extensive collateralization in the pelvis with reconstitution of the iliac arteries bilaterally and extensive SMA to IMA/epigastric territories collateralization.
View Figure 3
Figure 3: CT angiogram imaging with contrast showing infrarenal aortoiliac occlusion with extensive collateralization in the pelvis with reconstitution of the iliac arteries bilaterally and extensive SMA to IMA/epigastric territories collateralization.
View Figure 3
Following counseling, the patient elected to proceed with planned stepwise procedural interventions. Uterine artery embolization (UAE) was performed immediately before hysteroscopic myomectomy to decrease bleeding risk and anesthesia risks if emergent hysterectomy were needed.
The patient proceeded with UAE with our Interventional Radiology specialists. Under direct ultrasound guidance, a 21-gauge micropuncture needle was used to access the right common femoral artery. A wire was passed, and a 5 French sheath was placed. A Kumpe catheter was advanced to the confluence of the external and internaliliac arteries. Digital subtraction angiogram (DSA) imaging of the right internal iliac artery was performed. The artery and its branches were patent with a tortuous uterine artery.
A 2.4 French microcatheter was then advanced into the right uterine artery, and DSA and cone-beam CT were performed (Figure 4). This demonstrated arterial supply into the targeted fibroid seen on the previous MRI and the right cervicovaginal branch. The majority of the superior portion of the uterus was not supplied by the right uterine artery; however, the target fibroid was. These findings were confirmed on DSA imaging (Figure 5). The right uterine artery was embolized using Gelfoam tostasis, confirmed by subsequent DSA imaging.
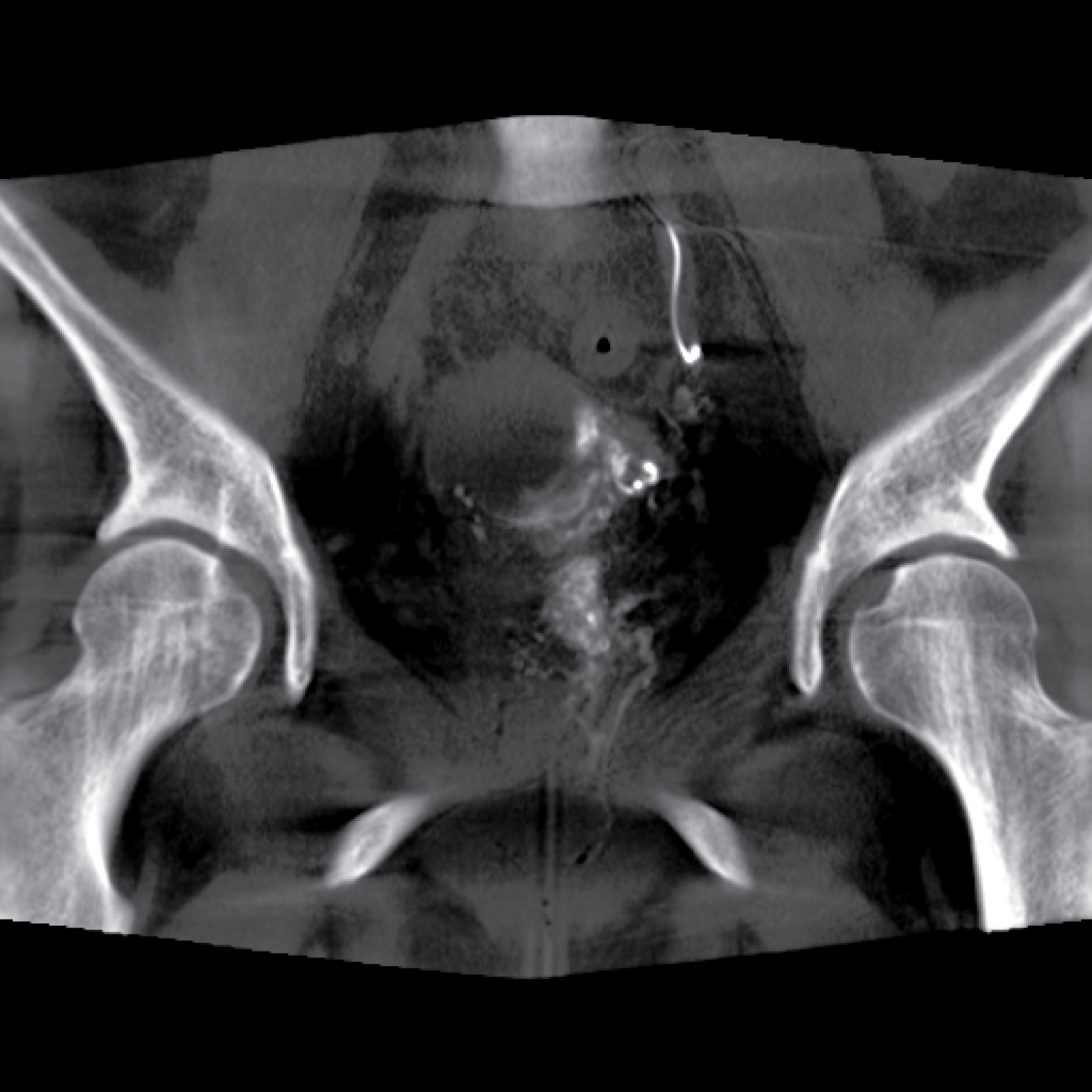 Figure 4: Come beam CT imaging of arterial supply into the targeted fibroid seen on previous MRI as well as the right cervicovaginal branch.
View Figure 4
Figure 4: Come beam CT imaging of arterial supply into the targeted fibroid seen on previous MRI as well as the right cervicovaginal branch.
View Figure 4
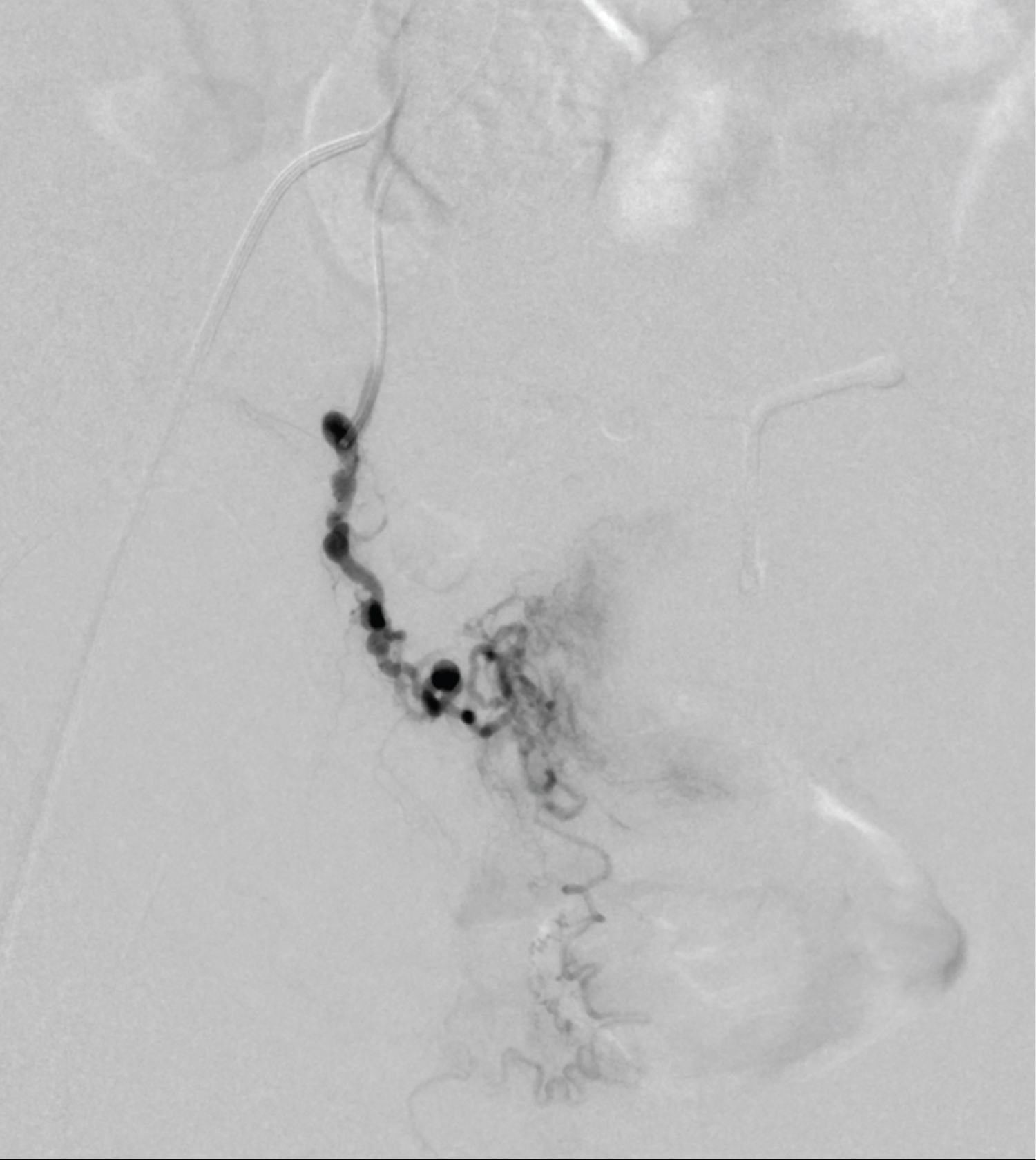 Figure 5: Digital subtraction angiogram (DSA) imaging of the right ovarian artery supplying the right side of the uterus.
View Figure 5
Figure 5: Digital subtraction angiogram (DSA) imaging of the right ovarian artery supplying the right side of the uterus.
View Figure 5
The left common femoral artery was then accessed using a 21-gauge micromotion needle under direct ultrasound guidance. A wire was passed, and the 4 French transitional sheath catheter was placed. A 2.4 French microcatheter was advanced into the external iliac artery through the transitional sheath catheter. DSA identified a patent internal iliac artery and uterine artery.
The left uterine artery was then selected after advancing into the iliolumbar vessel, forming a Waltman's loop, and entering the internal iliac artery. DSA and cone-beam CT were performed (Figure 6), which identified complete supply to the left half of the uterus with minimal supply to the cervicovaginal region. There was collateral flow to the right half of the uterus. No definite arterial supply was identified to the target fibroid. At that time, 250 μm and subsequently 400 μm Embozene™ Microspheres particles, as well as Gelfoam, were used to embolize the left uterine artery to stasis, confirmed by DSA imaging. A cone-beam CT was alp so erformed, which showed a reduction in the contralateral uterus supply. No supply was identified to the fibroid following these embolizations.
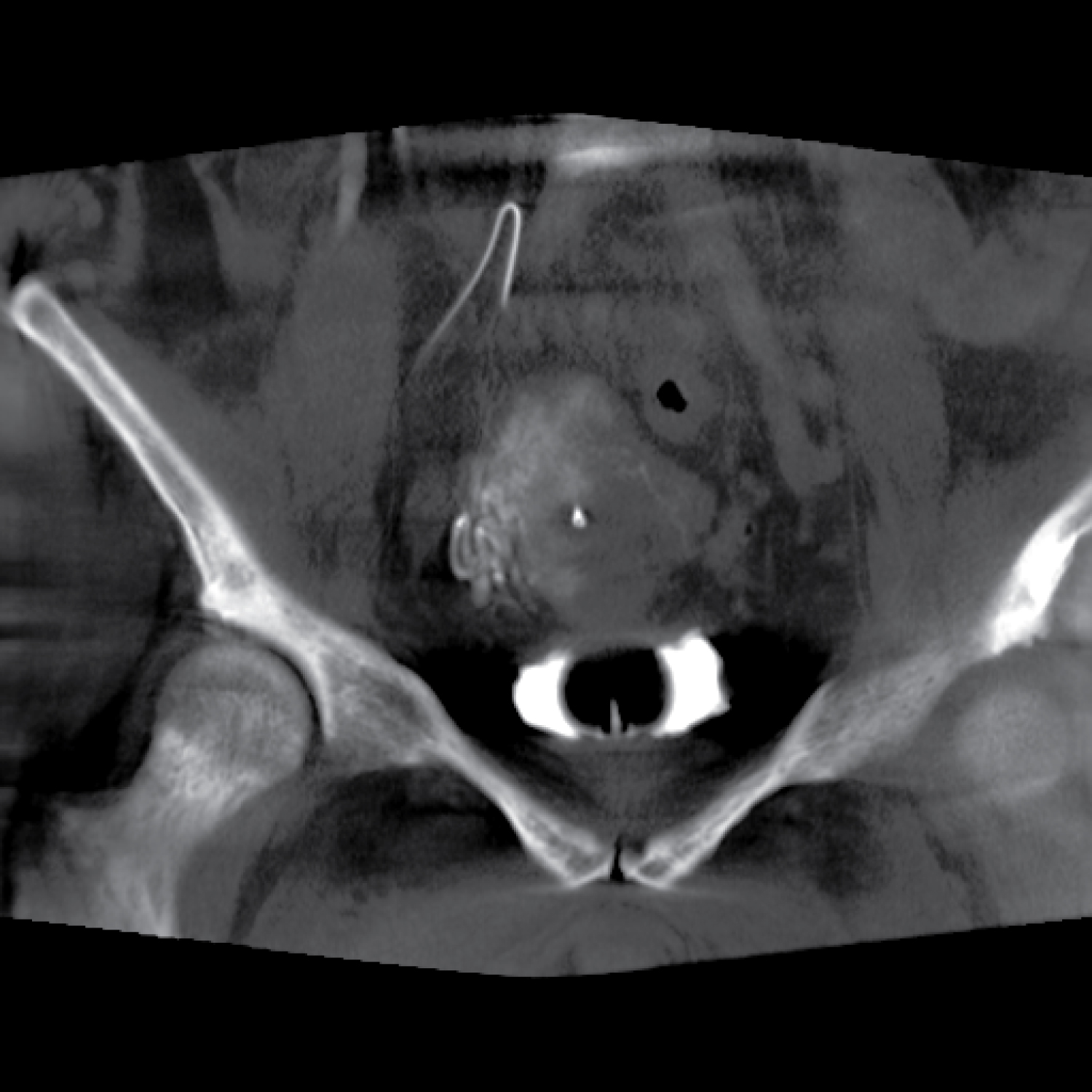 Figure 6: Cone beam CT imaging revealing complete supply to the left half of the uterus with minimal supply to the cervicovaginal region, and collateral flow to the right half of the uterus.
View Figure 6
Figure 6: Cone beam CT imaging revealing complete supply to the left half of the uterus with minimal supply to the cervicovaginal region, and collateral flow to the right half of the uterus.
View Figure 6
An exam under anesthesia performed immediately following the UAE revealed normal perineum and vulva. A 3 cm mass was noted to be prolapsing from the cervix on speculum exam. Bimanual examination revealed a normal cervix around the mass with a thin stalk. Ring forceps were used to grasp the IUS strings and remove the device to reduce the risk of iatrogenic infection after UAE. Ring forceps were then used to grasp the mass and gently twist until the mass was removed from the uterus (Figure 7a). A single tooth tenaculum was used to grasp the anterior lip of the cervix. No dilation was needed as the cervix was already dilated secondary to the mass. The hysteroscope with a twelve-degree scope was introduced through the cervical os. The canal of the cervix was noted to be free of lesions. The intrauterine cavity was reached, and inspection revealed no residual stalk or additional lesions (Figure 7b). The bilateral tubal ostia were inspected and normal. The bipolar resectoscope was used to coagulate the fibroid base, and appropriate hemostasis was confirmed before completing the hysteroscopic procedure.
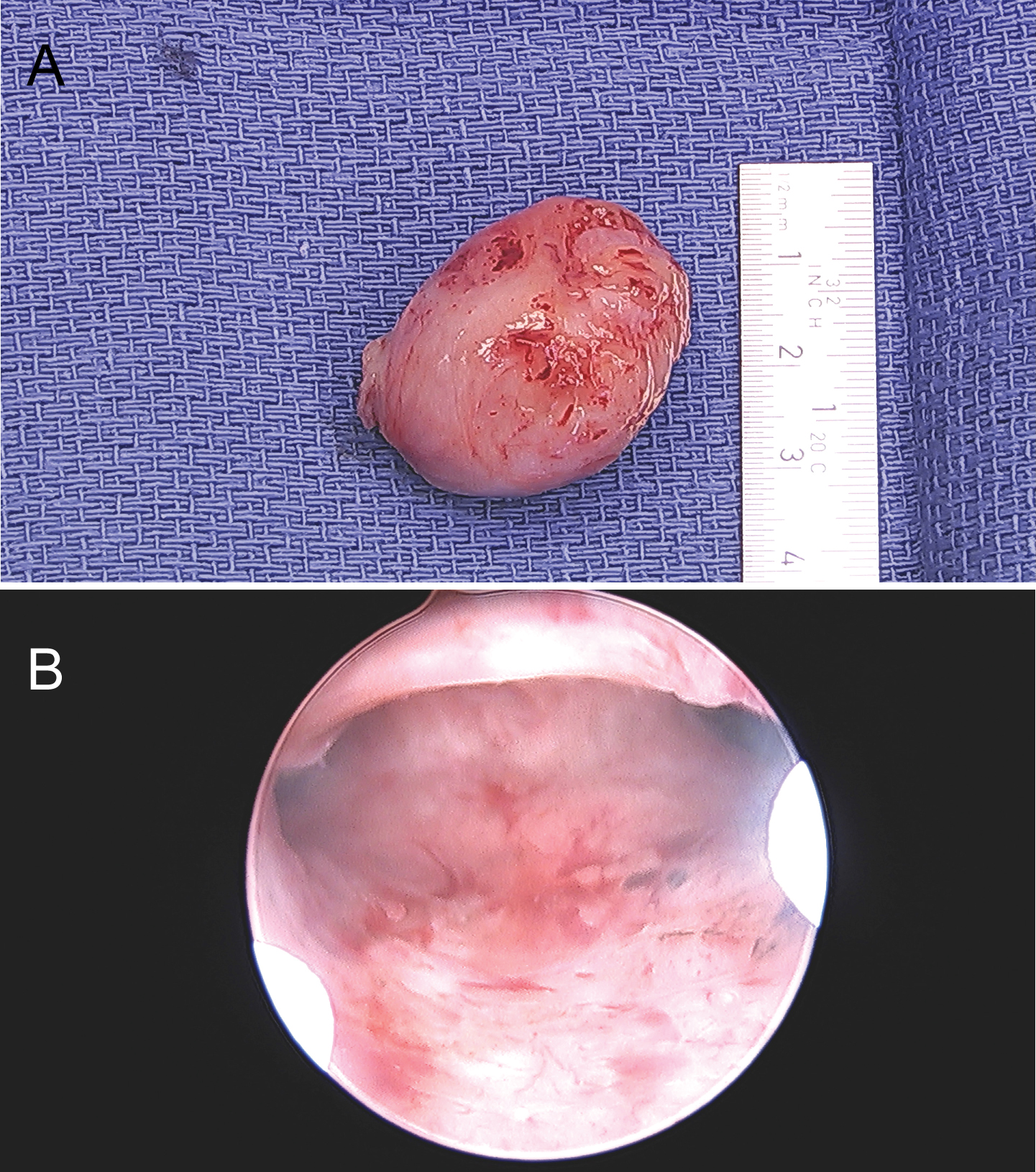 Figure 7: a) Gross section of intracavitary fibroid following removal; b) Intracavitary hysteroscopic review following resection of prolapsing intracavitary fibroid.
View Figure 7
Figure 7: a) Gross section of intracavitary fibroid following removal; b) Intracavitary hysteroscopic review following resection of prolapsing intracavitary fibroid.
View Figure 7
Following the above interventions, the patient was provided with norethindrone 5 mg once daily to decrease her HVB. Six weeks from her surgical procedures, a new IUS was placed. This was ultimately expelled by large clot formations, with a subsequent IUS placed four weeks later. The patient has done well since that time without the return of AUB/HVB.
Leiomyoma (also referred to as myoma or fibroids) are the most common benign tumor of the reproductive tract in premenopausal women. The most widely accepted classification, published in 2011 from the international federation of gynecology and obstetrics (FIGO), describes eight classes or subtypes based on their location and degree of myometrial involvement/invasion [1]. Subtypes 0 through 2, or submucosal leiomyoma, are located on the myometrium's innermost aspect and can be associated with abnormal or heavy uterine bleeding and reproductive difficulties. With the advancement of minimally invasive procedures, hysteroscopic myomectomy has become the gold standard for removing submucosal leiomyomas to normalize the uterine cavity [2].
Uterine artery embolization (UAE) has been accepted as an additional minimally invasive option for the treatment of leiomyoma. Pelvic arterial embolization has also shown promising safety and effectiveness in controlling postpartum hemorrhage [3,4]. A 2016 case series of 29 patients and a systematic review of the Medline and the Cochrane Libraries noted a success rate of embolization of 89% with uncommon significant complications (1.8%) [5]. Embolization was found to be a highly successful, safe, and minimally invasive treatment option for postpartum hemorrhage. There have been few case reports of the use of UAE to treat hemorrhage following laparoscopic myomectomy, most related to uterine artery pseudoaneurysm [6-12]. In their 2018 retrospective cohort study, Namkung, et al., reported successful and safe treatment of 8 patients with deep myometrial invading, submucosal myoma via UAE performed 3 to 15 months before hysteroscopy myomectomy [13]. The study determined that UAE was safe and effective in treating deep myometrial invading myomas, which can be challenging to treat with a one-step hysteroscopic removal. This therapy has yet, however, to be evaluated for prophylactic treatment in coagulopathic patients at high risk for hemorrhage following hysteroscopic myomectomy.
During this patient's UAE procedure, both permanent and temporary embolization agents were used. Gelfoam (Upjohn, Kalamazoo, MI), a temporary agent, is an absorbable gelatin sponge derived from a biologic substance made of purified skin gelatin [14]. The gelatin sponge is one of the most used agents in trauma [14]. When used for UAE, it has been shown to have minimal effect on subsequent fertility. Camacho, et al., reported in their 2019 retrospective study of eighteen patients with abnormal uterine bleeding related to recent gynecologic or obstetric events, that UAE with Gelfoam provided high technical and clinical success rates with minimal rates of complications [15]. Similarly, a recently published randomized controlled trial reviewed the clinical outcomes of non-resorbable calibrated hydrogel microspheres (Embozene-Varian Inc-700 & 900 microns) versus non-spherical polyvinyl alcohol, ns-PVA (Contour PVA-Boston Scientific-355-500 & 500-700 microns) for symptomatic uterine fibroids [16]. Superior fibroid infarction on MRI was noted using ns-PVA versus Embozenes, however there was no significant difference in clinic outcomes at 6 months for: Uterine Fibroid Symptom and Quality of Life questionnaire (UFS-QOL), percentage total and dominant fibroid infarction, uterine and dominant fibroid volume reduction, or volume of embolics [16].
The unique case presented reviews the utility of UAE in a staged procedure to prophylactically decrease hemorrhage risk associated with hysteroscopic myomectomy. Long-term data for uterine-sparing interventions are needed, notably whether these multidisciplinary approaches can reduce reintervention risk and improve quality of life outcomes.
This case report did not require IRB review or approval. All identifying features of the patient have been removed. Consent for release of imaging was obtained from the patient and is available upon request.
None.
None.