Most vertebral fractures are properly diagnosed by a simple radiography and a computed tomography (CT), but sometimes this type of preoperative study is insufficient to diagnose an inestable spine lesion [1,2].
We report a case of 19-years-old man who was brought to our Hospital after a bicycle accident. He had dorsolumbar pain, disability and anormal neurological examination. An X-ray and spine computerized tomography (CT) scan was performed and diagnosed a fracture at second vertebra lumbar. An unstable lumbar fracture which morphology was assessed on magnetic resonance (MRI), not looking like it in the preoperative X-ray and the tac. A completely rupture of the posterior ligamentary complex was evaluated on a MRI.
MRI is accurate in diagnosing posterior ligamentary complex rupture and has ability in the detection on unstable spinal injuries. MRI has the added advantages of detecting bone marrow edema and does not employ ionizing radiation [3].
MRI, Lumbar spine, Spine fracture, Posterior ligamentary complex, Unstable fracture
We report a case of 19-years-old man who was brought to our Hospital after a bicycle accident. He had dorsolumbar pain, disability and anormal neurological examination. It happened on a competition and he had a recording of his accident that showed us.
On radiographs and (CT), a simple L2 fracture was observed, which could be classified as AOSpine A1-type fracture with a Farcy kyphosis less than 16o and therefore make us think about the conservative treatment with corset (Figure 1 and Figure 2).
 Figure 1: (a) Sagittal rx (b) Frontal rx images demonstrates a fracture at L2 (A1), (AO classification).
View Figure 1
Figure 1: (a) Sagittal rx (b) Frontal rx images demonstrates a fracture at L2 (A1), (AO classification).
View Figure 1
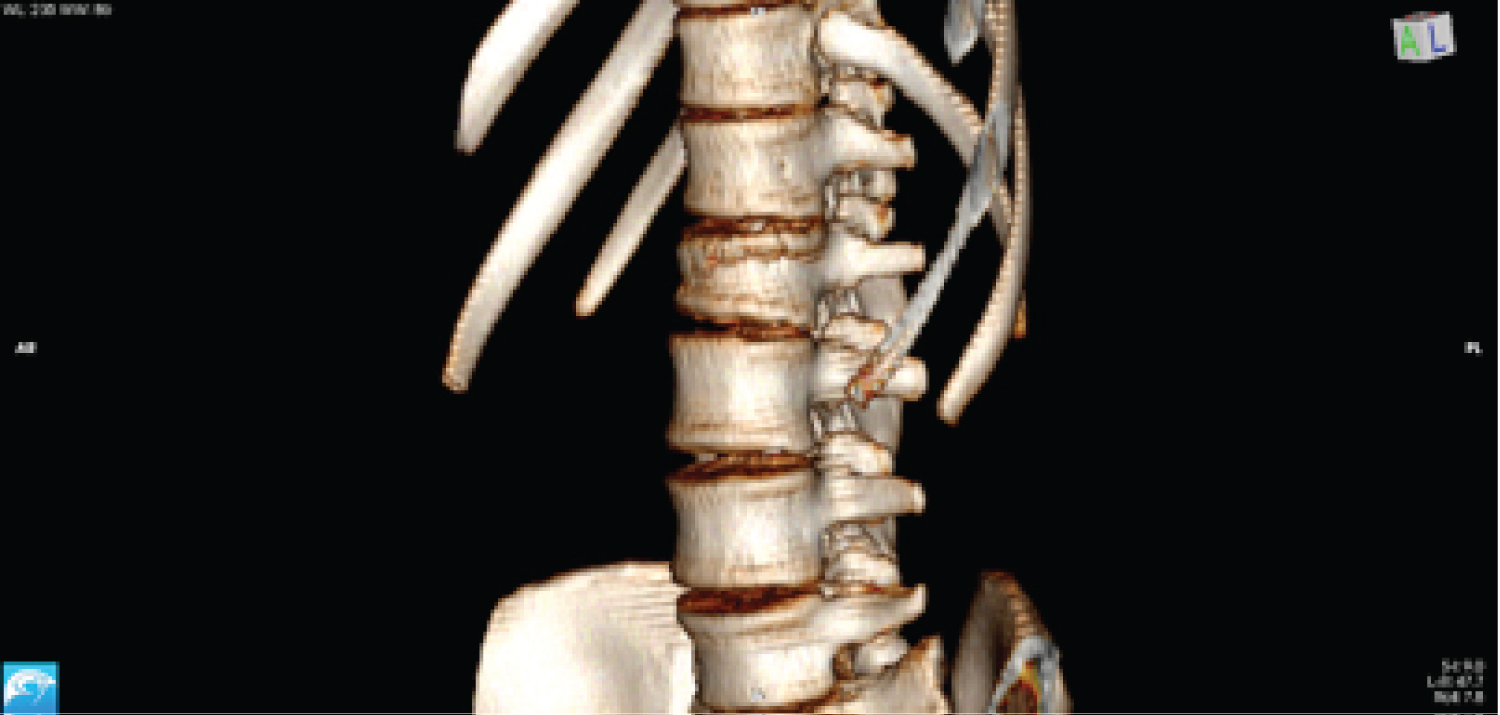 Figure 2: CT scan.
View Figure 2
Figure 2: CT scan.
View Figure 2
After carrying out the anamnesis, and observing the mechanism of production in the Video 1, we suspect a type B fracture, so a MRI was performed, where the lesion of the posterior ligament complex was confirmed, being then diagnosed as type B2 fracture of AO Spine, performing then the timely surgical treatment (Figure 3, Figure 4 and Figure 5).
 Figure 3: Image of the accident.
View Figure 3
Figure 3: Image of the accident.
View Figure 3
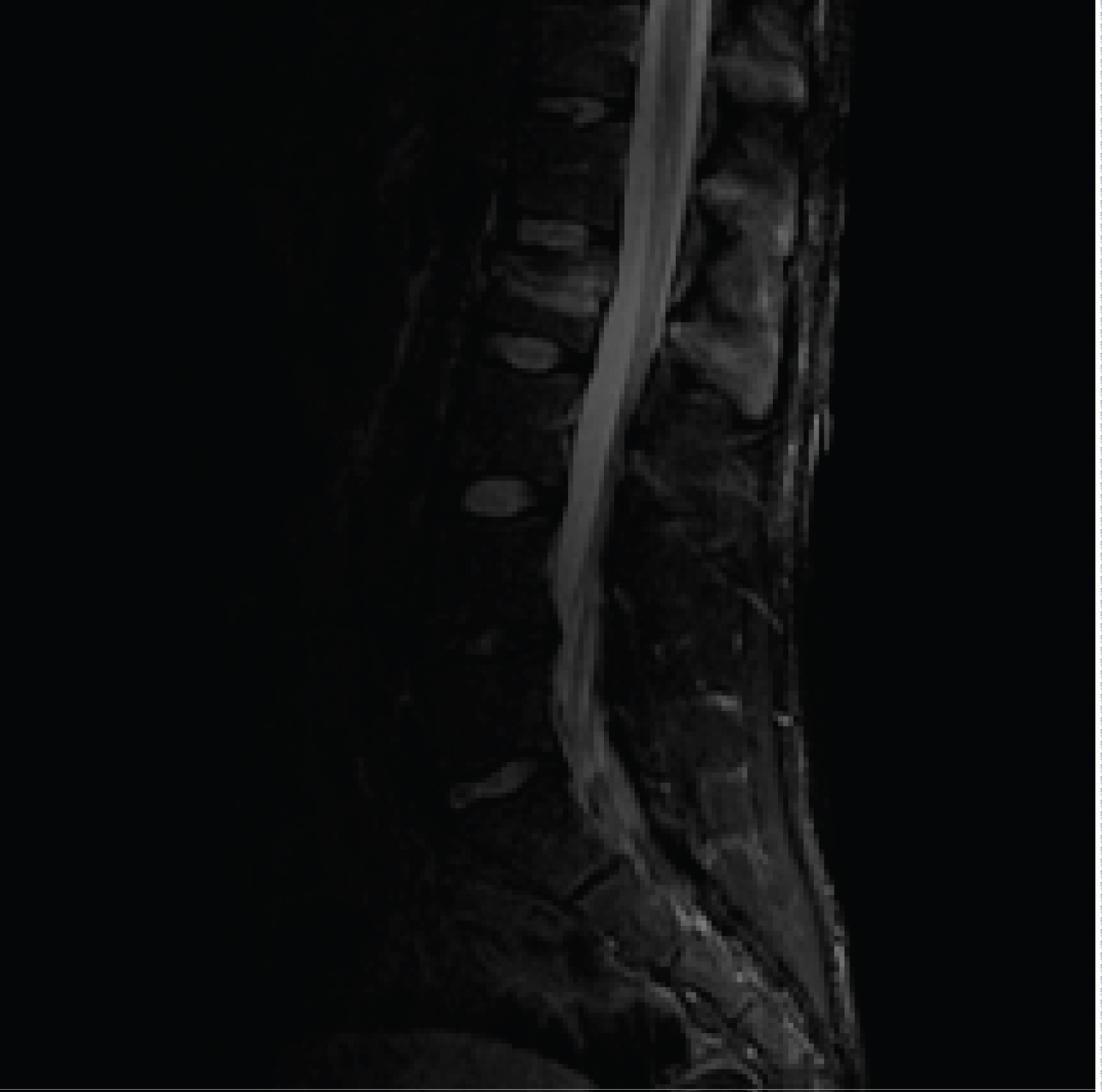 Figure 4: Fracture L2 level (a) Sagittal MRI image completely rupture of the posterior ligamentary complex was evaluated.
View Figure 4
Figure 4: Fracture L2 level (a) Sagittal MRI image completely rupture of the posterior ligamentary complex was evaluated.
View Figure 4
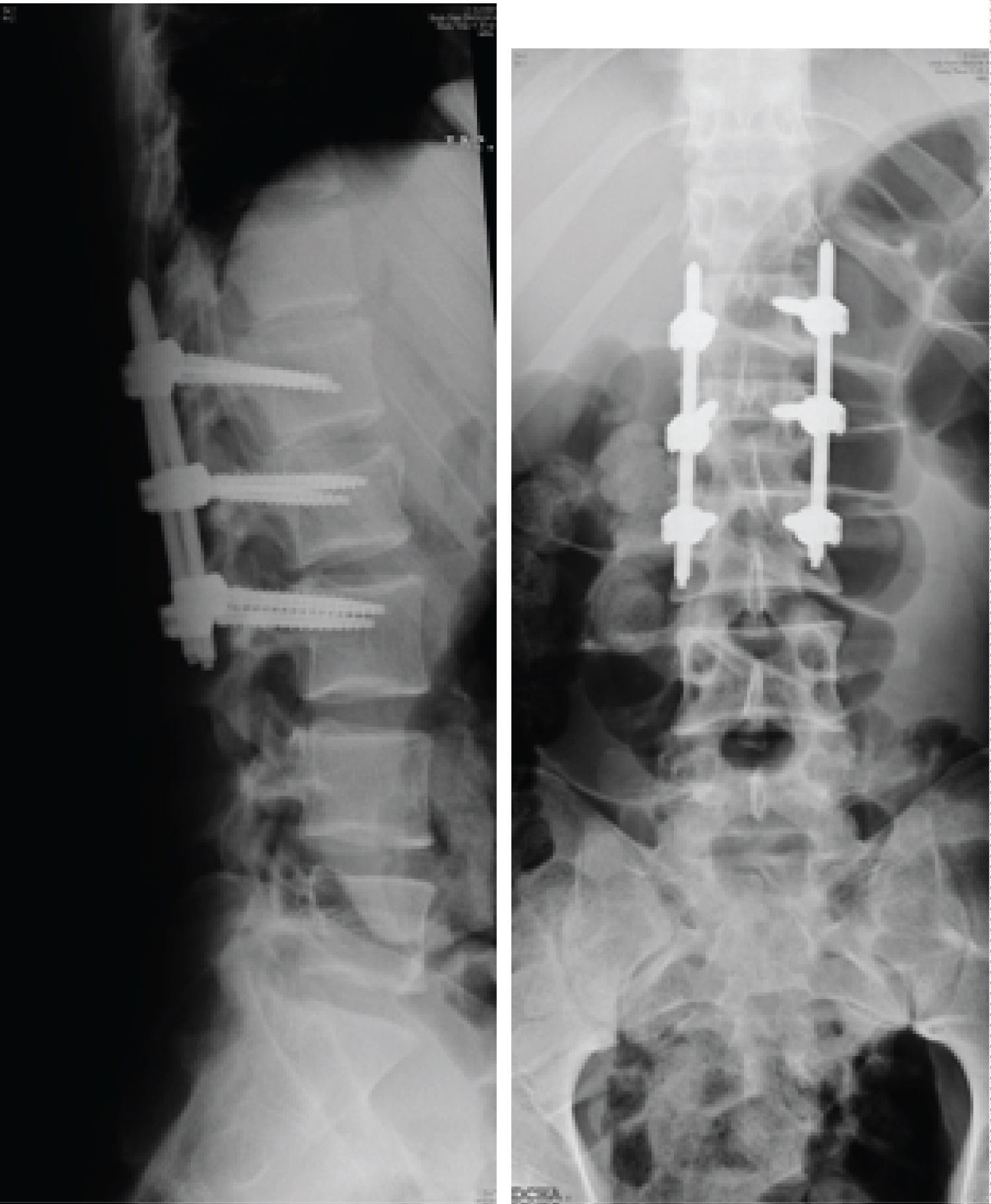 Figure 5: (a) Anteroposterior spine radiograph after surgery; and (b) Lateral spine radiograph illustrating the posterolateral instrumented fusion L1-L3.
View Figure 5
Figure 5: (a) Anteroposterior spine radiograph after surgery; and (b) Lateral spine radiograph illustrating the posterolateral instrumented fusion L1-L3.
View Figure 5
Magnetic Resonance Imaging (MRI) offers unique advantages compared to other imaging methods in the assessment of a multitude of spinal disorders [4].
Its ability to obtain images in multiple planes allows a direct visualization of the complex spinal anatomy, providing the surgeon with accurate and complete preoperative information, thus improving surgical planning. This is particularly useful in the evaluation of complex spinal deformities and when minimally invasive surgery techniques are proposed.
Its superior resolution of tissue and spatial contrast make it more specific and sensitive in the evaluation of soft tissues as well as in the infiltrative disorders of the bone marrow, metastasis, infections or reactive changes of the saucer.
The disadvantages of MRI are relatively few. It is considered that its cost is approximately double that of a computed tomography (CT) [5].
If there is a suspicion of unstable spine fractures, an MRI should be performed [4,5].
Spinal support ligaments include the ligament anterior longitudinal, posterior longitudinal ligament, interspinous and supraspinatus ligament. These ligaments are identified in sagittal images as linear areas of low signal strength. The interruption of this hyposignal constitutes direct evidence of ligamentous disruption and can be identified in any pulse sequence In case of ligament injury interspinous we can observe areas of increase signal in T2 sequences in interspinous soft tissues [5].
All authors have no financial support or relationships that may pose a conflict of interest to disclose for this work.