To systematically review the literature available on the use of Denosumab (Dmab) in osteoporosis and the risk of ONJ.
The studies retrieved by the above strategies were included if they met the following pre-established criteria. The patients studied had to be diagnosed of osteoporosis (all ages, both sexes), and they had to be taking Dmab. We measured the likelihood of having osteonecrosis of the jaw. We included in the search for systematic reviews randomised clinical trials (RCT) and cohort studies. We excluded articles on cancer or other disease other than osteoporosis, animal and basic science studies. There was no limitation with regard to the number of patients included in the studies. The bibliographic databases screened were Medline and Embase and the Cochrane. The searches were conducted with language restriction (English, French and Spanish).
We found 10 articles that were studied in detail because by title or abstract they seemed to be related to the study, or because they had no abstract to review. Finally, 2 studies were included (one of them by indirect search) (Table 1). One of the study included was case series and another was systematic review of cases and series of cases and their data retrieved. The quality level of the two articles was low. Related to the studies population, all patients had osteoporosis, mostly were women with mean ages around 50-78 years. All patients were treated with subcutaneous denosumab every 6 months.
Table 1: Main characteristics of the included studies. View Table 1
In these two studies, the incidence of ONJ was very low. Some systemic factors such as previous treatment with BPs or dental extractions are associated with the development of osteonecrosis of the jaws in patients treated with Dmab. Stage 1 of ONJ was the most common and conservative treatment was used with the healing of the lesions.
There are not enough studies that have evaluated the role of Dmab in the development of osteonecrosis (ONJ) of the jaws. Some systemic factors that have been associated with the development of ONJ are described in patients treated with Dmab, such as previous treatment with bisphosphonates or tooth extractions.
Osteoporosis is a disease characterized by decreased bone mass, microarchitectural deterioration of the skeleton and impaired bone strength which results from increased bone resorption relative to formation. Anti-resorptive drugs significantly reduce bone turnover, providing an increase in BMD and a reduction in risk of fracture [1].
Recent advances have identified the Receptor Activator for Nuclear Factor -B Ligand (RANKL) as a critical mediator of bone remodeling. RANKL is essential for the formation, function, and survival of the osteoclasts. It binds to its cognate receptor RANK on the surface of precursors and mature osteoclasts, and stimulates these cells to mature and resorb bone.
Dmab is a novel antiresorptive agent that also inhibits osteclast-mediated bone resorption but works through a different pathway than bisphosphonates. Dmab is a fully human monoclonal antibody (IgG2) that inhibits RANKL with high specificity, mimicking the effects of OPG on RANKL.6 [2].
Following menopause, increased RANKL results in increased bone resorption and bone loss, which can lead to osteoporosis, a condition characterized by compromised bone strength and increased risk of fracture [3]. In postmenopausal women with osteoporosis, denosumab significantly reduced bone turnover markers (BTMs), increased bone mineral density (BMD), and reduced new vertebral (68%), hip (40%), and nonvertebral (20%) fractures compared with placebo [4].
The American Association of Oral and Maxillofacial Surgeons (AAOMS) has recently (2014) updated their definition of medication-related ONJ to (1) Current or previous treatment with antiresorptive or antiangiogenic agents; (2) Exposed bone or bone that can be probed through an intraoral or extraoral fistula (e) in the maxillofacial area that has persisted for more than 8 weeks; and (3) No history of radiation therapy to the jaws or obvious metastatic disease to the jaws [5].
The ONJ is a multifactorial disease, of which occurrence is predisposed by some factors. It includes local factors such as tooth extraction, dent alveolar surgery, periodontal disease, trauma from ill-fitting dentures [6] and systemical factors such as malignant diseases (breast, lung and prostate, multiple myeloma), chemotherapy, chronic steroid therapy, smoking, diabetes and anaemia [6].
The aim of this study was, therefore, to systematically review the literature available on the use of Dmab in osteoporosis and the risk of ONJ. This information was afterwards examined and used by the experts of the Spanish Society of Rheumatology Consensus of osteoporosis to generate clinical practice recommendations for rheumatologists.
As a part of the Spanish Society of Rheumatology Consensus of osteoporosis, a systematic literature review was performed to address the experts' question on the risk of osteonecrosis of the jaw in patients with postmenopausal osteoporosis. A protocol of the review was established and further advice from the complete team of the Consensus was obtained.
The studies were identified by sensitive search strategies in the main bibliographic databases (Table 2). For this purpose, an expert librarian collaborated and checked the search strategies.
Table 2: Search strategies in the different bibliographic databases and hits. View Table 2
The following bibliographic databases were screened as follows: Medline and Embase from the beginning to 8th May 2017, and the Cochrane Central register of Controlled Trials (CENTRAL) up to 8th May 2017. The searches were conducted with a language restriction (English, French and Spanish).
In the end, a hand search was completed by reviewing the references of the included studies, and all the publications or other information provided by the experts related to the systematic review were also examined.
The studies retrieved by the above strategies were included if they met the following pre-established criteria. The patients studied had to be diagnosed of osteoporosis (all ages, both sexes), and they had to be taking Dmab. We measured the likelihood of having osteonecrosis of the jaw.
We included in the search for systematic reviews randomised clinical trials (RCT) and cohort studies. We excluded articles on cancer or other disease other than osteoporosis, animal and basic science studies. There was no limitation with regard to the number of patients included in the studies. Selection of studies and data collection EndNote X7s software was used to manage the records retrieved by searches of the different electronic data bases and manual search methods.
One reviewer (G.C) screened the titles and abstracts of the retrieved articles for selection criteria independently. The reviewer collected the data from the studies included by using ad hoc standard forms. All collection was double by article and independent. The reviewer entered the data from the forms into spreadsheets. Articles that did not fulfil all the inclusion criteria or that had insufficient data were excluded. To grade the quality, we used the levels of scientific evidence and SIGN recommendation grades. Metaanalysis was only planned in case enough homogeneity was present among the included studies.
The result of the search strategies is presented in Table 2 by specific terms, and in total in Figure 1. We found 10 articles that were studied in detail because by title or abstract they seemed to be related to the study, or because they had no abstract to review. Table 3 shows the studies that were excluded after detailed review and the reasons for exclusion. Finally, 2 studies were included (one of them by indirect search) (Table 1). One of the study included was case series and another was systematic review of cases and series of cases and their data retrieved. The quality level of the two articles was 3. Table 1 shows the main characteristics of the included studies.
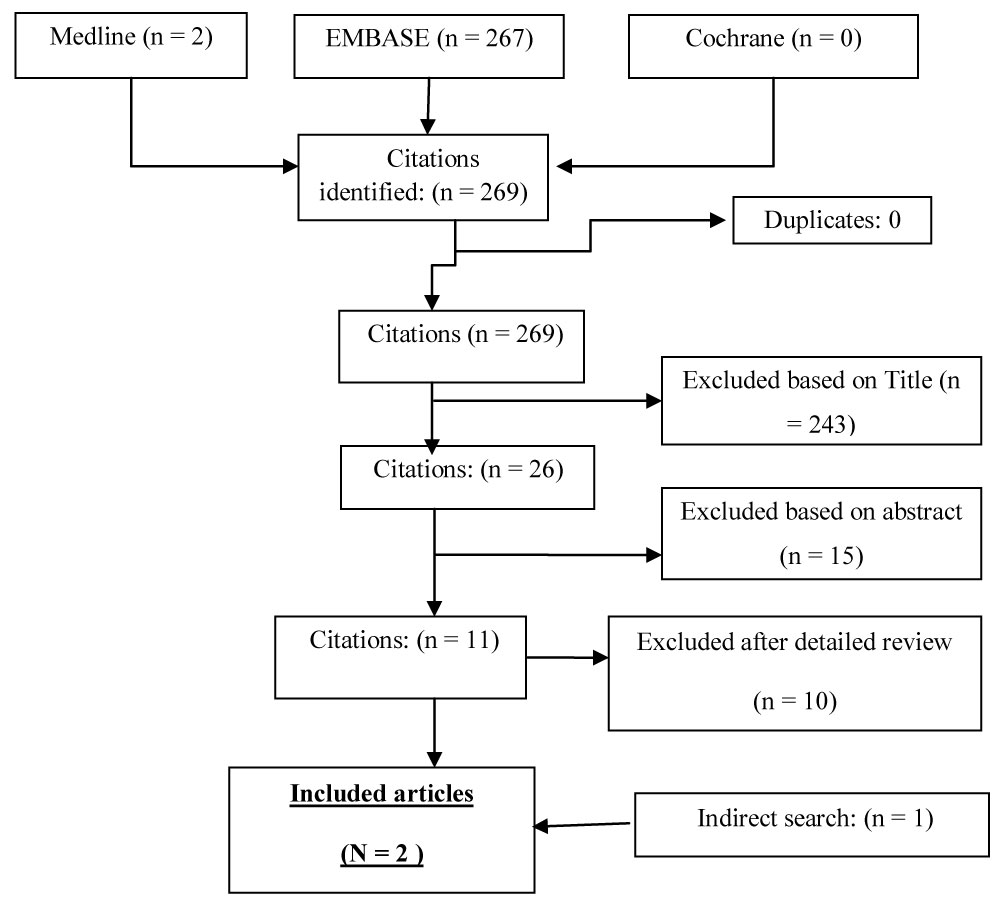 Figure 1: Articles retrieved by the different search strategies and result of selection and appraisal process.
View Figure 1
Figure 1: Articles retrieved by the different search strategies and result of selection and appraisal process.
View Figure 1
Table 3: Excluded studies and reasons for exclusion. View Table 3
Related to the studies population, all patients had osteoporosis, mostly were women with mean ages around 50-78 years. All patients were treated with subcutaneous Dmab every 6 months.
In the study of Bagan, et al. [7] all patients with osteoporosis treated with Dmab at a dose of 60 mg subcutaneously every 6 months were included. Exclusion criteria were treatment with other medications or chemotherapy for associated cancers. In each case, in addition to age and sex, Dmab doses were recorded, and in patients who had been previously treated with bisphosphonates (BPs), the drug used and time in treatment were recorded.
With regard to ONJ, the location of the lesions in the jaw was recorded and the presence of local and systemic risk factors that could contribute to the appearance of the lesions (dental extractions, implants, prosthesis or spontaneous appearance). In each case, orthopantomography was performed, and in three of the eight cases, a computerized tomography was performed. The presence of osteolysis, sclerosis and bone sequestration was recorded. The mean number of doses of Dmab was 3.4 ± 2.2.
Nine patients (90%) had also been treated before with oral BPs, for an average of 44.7 ± 25.11 months. Four had been treated with ibandronate, three with risedronate and three with alendronate. In seven cases (70%), the ONJ was located in the jaw. The most common local risk factor found was tooth extraction (six cases, 60%); Only one case associated with dental implant was found. Three cases (30%) had an intraoral and necrotic fistula and in 9 cases (90%) bone exposure was observed. Regarding the radiographic changes observed, bone sclerosis was present in all cases. No sequestration was found in any case, osteolysis was present in six cases (60%).
Stage 1 of ONJ was the most common, occurring in eight cases (80%), and in all cases except one, conservative treatment was used with the healing of the lesions. One patient did not agree to be treated due to his age and concomitant systemic diseases. The follow-up was lost in two patients.
In the other study [6] the objective was to perform a systematic review that included the clinical cases published in the literature of people who develop ONM after DNM treatment. However, not all selected cases corresponded to people with osteoporosis. To do this, they conducted a review of the evidence using PubMed, Medline and Cochrane from January 2010 to May 2015. Articles should be case reports or series of clinical cases, in patients 18 years of age or older who used Dmab for the prevention of bone metastases and/or treatment of osteoporosis and giant cell tumors or patients who had received some therapy for ONJ.
Based on the established criteria, 22 articles were selected. The parameters analyzed were: Type of disease treated, the characteristics of Dmab treatment, age and sex of the patient, site affected by ONJ, local and systemic risk factors and treatment.
Thirteen full case reports or case series articles were selected for this review. In total, 17 clinical cases were found. Of the 17 cases, only 8 were in patients who had received treatment with Dmab for osteoporosis or osteopenia (47.0%) The majority of cases of ONJ occurred in the posterior mandibular area and only one of them in the posterior maxillary area. Previous treatment with BPs was the most frequent (in 6 of the 8 patients). One patient had received 3 different types of BPs (alendronate and risedronate for 6 years and zoledronate for 1 year). The second most frequent risk factor found was dental extractions (4 of the 8 cases). Of the 8 cases, in 4 of them the received treatment was not exposed. Of the remaining 4, only one of them required surgery and the rest remitted the lesions after conservative treatment.
In the present study we have analyzed the risk of ONJ in patients that use Dmab for the treatment of osteoporosis. For the purpose of the present systematic literature review, we decided to include descriptive studies and case series and qualitative research studies.
We finally included a total of 2 studies. The quality of most of them was low.
ONJ has been observed in patients receiving denosumab at much higher doses than those prescribed for osteoporosis, typically as an antimetastatic agent for cancer [8]; however, it also has been reported in those receiving the normal doses for osteoporosis [5].
Some systemic factors such as previous treatment with BPs or dental extractions are associated with the development of osteonecrosis of the jaws in patients treated with denosumab (level of evidence 3) [6].
There are not enough studies that have evaluated the role of denosumab in the development of osteonecrosis of the jaws (level of evidence 3) [6,7].
The incidence of ONJ in the FREEDOM trial extension was low (0.18 %), with most (six of eight) cases occurring after at least 4 years of exposure [9]. Dmab studies suggested that ONJ may be more likely to develop when Dmab is given to patients with risk factors such as dental extraction, poor oral hygiene, use of removable dental appliances, or chemotherapy [8].
The authors of the review found ONJ cases in seven trials in which Dmab was administered as an antimetastatic agent. These trials enrolled a total of 5072 patients who received 120 mg of Dmab subcutaneously every 4 weeks or every 6 months, and ONJ was reported in 96 of them. Therefore, the incidence of ONJ was low, ranging from 0 to 2% over 13 to 21.4 months of treatment.
Several medical associations have published recommendations to reduce the risk of this complication. In general, the guidelines include in their proposals a correct dental hygiene and revision by a dentist if poor dental health is objectified. If an invasive odontological procedure is planned -exodontia or implant- it is advisable to postpone the start of treatment until the surgical wound is completely healed.
There is some controversy about the attitude to be followed in patients who are already taking Dmab. Most guidelines advise non-oncological patients not to suspend the treatment. In a recent consensus document, in patients who are going to undergo extensive oral surgery and associated risk factors (diabetes, periodontal disease, immunodeficiencies, smoking), clinical judgment may advise temporarily suspending treatment. In this situation, unnecessary prolongation of the suspension should be avoided, especially in patients treated with Dmab. In case of a relevant adverse event such as osteonecrosis of the jaws, and although there is no scientific evidence to show that the withdrawal of the drug will improve the evolution of the process, the same document considers it prudent to suspend it and assess the indication of drugs with different mechanism of action [5].
In conclusion, not enough studies have been found that have evaluated the role of Dmab in the development of osteonecrosis (ONJ) of the jaws. Some systemic factors that have been associated with the development of ONJ are described in patients treated with Dmab, such as previous treatment with BPs or tooth extractions.