Shear wave elastography (SWE) is a relatively new and highly effective method to reveal mechanical features of tissue by demonstrating quantitative elasticity value. The morphological features including margin of the lesion, orientation, shape and border are considered in differentiation of breast lesions on USG. It is a known fact that malignant lesions are usually palpated as a hard mass in the physical examination. A qualitative broad information can obtain about the tissue elasticity by integrating SWE examination into the classical USG evaluation. We reported the finding of SWE examination in breastfeeding patient with breast malignancy in addition to magnetic resonance imaging (MRI) and ultrasonography (USG) findings.
Shear wave elastography, Invasive ductal carcinoma, Breastfeeding
Shear wave elastography (SWE) is a relatively new and highly effective method to reveal mechanical features of tissue by demonstrating quantitative elasticity value [1]. Qualitative and quantitative elasticity values can be helpful in differentiating malignant breast lesions from benign ones [2]. Herein, we reported the finding of SWE examination in breastfeeding patient with breast malignancy in addition to magnetic resonance imaging (MRI) and ultrasonography (USG) findings.
A 27-year-old young female patient admited to our hospital complaining from pain in the right breast. In the young patient with no history of cancer in the family; The patient was breasfeeding and labaratuary findings were normal. On physical examination, a hard mass was palpated in her right breast. A hypoechoic mass lesions was sonographically detected on the right breast in a diameter with 31 × 24 mm (Figure 1). SWE was performed to obtain additional information about mass lesion. Many stiff areas observed within mass lesion on color elasticity mapping. Mean elasticity value was 6.04 m/s 101.4 kPa on consecutive measurement (Figure 2). A core needle biopsy was performed immediately. One of the most important reason of the immediate core needle biopsy was the detection of quite hard mass on SWE. Thus, SWE examination prevented a possible delay in diagnosis in this young, breastfeeding patient. Invasive ductal carcinoma was revealed on histopathological examination. Breast MRI was performed to exclude multicentric carcinoma. In the inner quadrant of the right breast, hypointense on T1 sequences and heterogeneous hyperintense on T2 sequences, irregular mass formations was seen on MRI (Figure 3). Diffusion restriction was detected on diffusion-weighted images and heterogeneous enhancement was observed within lesions. Patient underwent mastectomy.
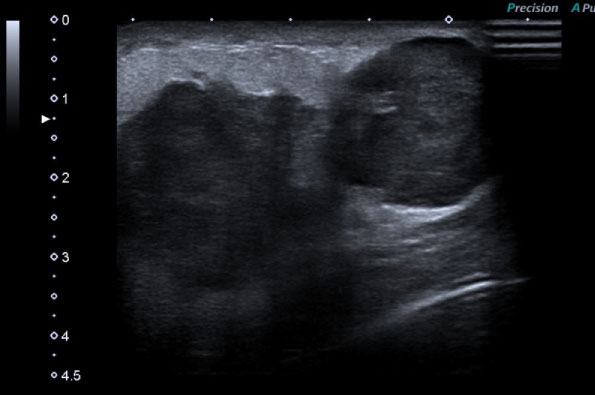 Figure 1: A hypoechoic mass lesions was sonographically detected on the right breast in a diameter with 31 × 24 mm.
View Figure 1
Figure 1: A hypoechoic mass lesions was sonographically detected on the right breast in a diameter with 31 × 24 mm.
View Figure 1
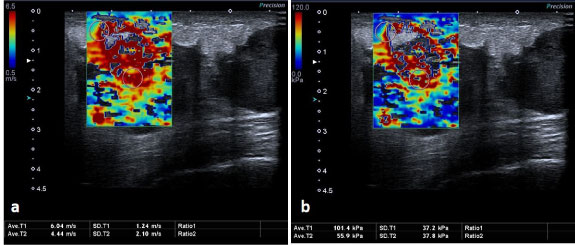 Figure 2: a,b) On SWE images; Any stiff areas observed within mass lesion on color elasticity mapping. Mean elasticity value was 6.04 m/s 101.4 kPa on consecutive measurement.
View Figure 2
Figure 2: a,b) On SWE images; Any stiff areas observed within mass lesion on color elasticity mapping. Mean elasticity value was 6.04 m/s 101.4 kPa on consecutive measurement.
View Figure 2
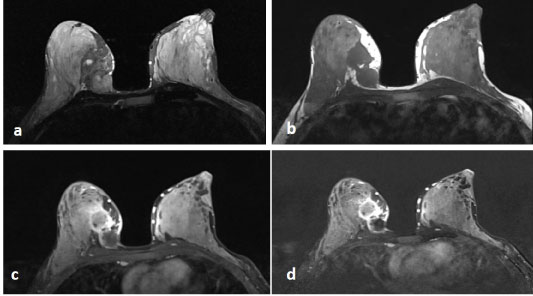 Figure 3: In the inner quadrant of the right breast, hypointense on axial T1 sequence (a) and heterogeneous hyperintense on axial T2 sequence (b), (c) early and late (d) enhanced axial sequences are demonstrated irregular mass formations was seen on MRI.
View Figure 3
Figure 3: In the inner quadrant of the right breast, hypointense on axial T1 sequence (a) and heterogeneous hyperintense on axial T2 sequence (b), (c) early and late (d) enhanced axial sequences are demonstrated irregular mass formations was seen on MRI.
View Figure 3
The morphological features including margin of the lesion, orientation, shape, border and echogenicity are considered in differentiation of breast lesions on USG. It is a known fact that malignant lesions are usually palpated as a hard mass in the physical examination. Unfortunately, USG does not provide information about the stiffness of the lesion. A qualitative broad information can obtain about the tissue elasticity by integrating SWE into the classical USG evaluation. In our patient SWE examination prevented a possible delay in diagnosis in our young who has breastfeeding patient. It is a known fact that malignant mass lesions are harder with the palpation compared to benign lesions. Recently, many researchers reported that elasticity measurements can faciliated to establish correct diagnosis [3-5]. While Olgun, et al. [4] reported that even 37.1 kPa as a mean elasticity cut-off values is a confident marker in differentiating malign lesion from benign [6-8], many researchers suggested that higher mean elasticity values varying between 65 kPa to 80 kPa is more reliable [6,8,9]. In our case report; we measured higher elasticity values in our malign lesion 101.4 kPa on consecutive measurement, which was highy suggestive of malignancy.
In conclusion; integration SWE measurement into USG examination may useful in differing malign lesions from benign ones.