Nocardiosis is a relatively rare disease with an incidence of 3 cases per 1,000,000 each year in the United States. The infection is caused by the Nocardia spp., which are aerobic, gram-positive, branching, weakly acid-fast bacilli found primarily in soil, water and decaying vegetation. Nocardiosis can be localized to a single organ, such as the skin or lung, or disseminated [1]. Immunocompetent patients who are affected typically experience a chronic course involving one organ, most commonly the lung. Patients who are immunocompromised, such as organ transplant recipients or patients on long-term corticosteroids, are much more likely to experience disseminated disease, which normally starts in the lungs and spreads hematogenously [2]. We report the case of a 64-year-old man on long-term immunosuppressant therapy for sarcoidosis who developed disseminated Nocardia farcinica infection.
A 64-year-old African American male with past medical history of sarcoidosis, hypertension, anemia, and chronic kidney disease presented to the emergency department with fevers as high as 103 ℃, leg pain, and back pain that had been worsening over the previous month. Home medications included atorvastatin, testosterone, Symbicort, amlodipine, azathioprine and prednisone for his sarcoidosis, zolpidem, hydrochlorothiazide, Norco, and febuxostat. On admission, his vital signs were stable, and pertinent physical exam included tenderness to palpation in the right thigh and left lower thoracic/upper lumbar paraspinal area with intact gross sensation and strength. Pertinent initial laboratory findings included a hemoglobin of 10.5 (MCV 109), BUN of 52, creatinine of 2.8, CRP of 14.3, and ESR of 86. A urinalysis and urine culture were negative. Blood cultures were sent. Chest X-ray showed scattered bilateral interstitial and airspace opacities. Magnetic resonance imaging (MRI) of the lumbar spine showed a large left paraspinal muscle fluid collection and satellite collections. Interventional radiology was consulted to drain the fluid collection for cultures while the patient was started on IV vancomycin. His home prednisone and azathioprine were held. Initial blood culture was positive for acid fast bacteria and the patient was switched from vancomycin to combination trimethoprim-sulfamethoxazole (TMP-SMX) and linezolid. A head computed tomography (CT) and MRI of the brain showed a left capulostriatal infarct and multiple punctate areas throughout bilateral cerebral hemispheres. A CT of the chest demonstrated multiple nodules in the lower lobes and left upper lobe along with a possible right hilar mass and scattered areas of consolidation (Figure 1). An ultrasound of the right thigh showed a solid and cystic mass, which was drained. A TTE and TEE came back negative for vegetations. Cultures eventually came back positive for Nocardia spp. The patient was clinically stable and therefore switched to oral antibiotics and discharged with outpatient follow-up scheduled.
 Figure 1: CT of the chest on initial presentation. View Figure 1
Figure 1: CT of the chest on initial presentation. View Figure 1
Almost two weeks after discharge, the patient presented to an outside clinic with severe nausea and generalized weakness, which subsequently required re-admission. Upon admission, linezolid was discontinued and trimethoprim-sulfamethoxazole (TMP-SMX) was continued along with minocycline. Within a week of presenting back to the hospital, the patient became septic and experienced chills, emesis and severe pain. Prior abscess culture speciated Nocardia farcinica. With minimal improvement in clinical symptoms, meropenem and amikacin were added to the patient’s antibiotic regimen. To further assess the causal etiology of his clinical deterioration, new imaging was obtained. The MRI of the brain was suggestive of subacute septic emboli (Figure 2). The CT of the chest revealed minimal change. The CT of the abdomen and pelvis showed bilateral pleural effusions with scarring and fibrosis in the lung bases and lymphedema in the soft tissues of each flank and thigh, with serial chest X-rays showing increased lung opacities, low lung volumes and right side pleural effusion. The patient continued to be septic despite multi-drug regimen, prompting repeat blood cultures. Interventional radiology (IR) was consulted for the placement of right thigh and left back drains. The patient’s clinical status along with intractable nausea and vomiting, thought to be caused by trimethoprim-sulfamethoxazole (TMP-SMX) resulted in significant deficit in oral intake, thus requiring total parenteral nutrition. Additionally, the patient developed asymptomatic hyperkalemia, also thought to be due to trimethoprim-sulfamethoxazole (TMP-SMX), which called for replacement with linezolid. Shortly thereafter, the patient’s nausea and vomiting began to improve but he became lethargic. An MRI of the spine showed recurrent paraspinal soft tissue abscesses and MRI of the brain showed worsening septic emboli consisting of increased number of collections and size (Figure 3). A few days later the patient demonstrated improved lethargy and oral intake; however, minocycline was no longer available due to a manufacturer shortage. Trimethoprim-sulfamethoxazole (TMP-SMX) was resumed and meropenem was switched to imipenem. Repeated abscess cultures returned a few days later with Nocardia spp., sensitivities were still pending. The patient continued to remain septic and developed acute on chronic hypoxic respiratory failure requiring BiPAP use at one point. A repeat CT of the chest showed new consolidative opacities, mildly increased perihilar consolidation, small scattered bilateral pulmonary nodules, and worsening bilateral pleural effusions (Figure 4). Given persistent sepsis and clinical deterioration while on multiple antibiotics, fungal studies were obtained. Less than a week later, Nocardia sensitivities returned revealing imipenem-resistance; therefore, imipenem was discontinued and the patient remained on trimethoprim-sulfamethoxazole (TMP-SMX), amikacin and linezolid. The thigh and back drains were removed by IR given decreased output. The patient continued to improve clinically and was slowly increasing his oral intake; however, was still experiencing nausea and vomiting. Repeat fungal studies came back negative. The patient was transitioned to oral amoxicillin-clavulanic acid and moxifloxacin prior to discharge, with antibiotic therapy expected to continue for one year.
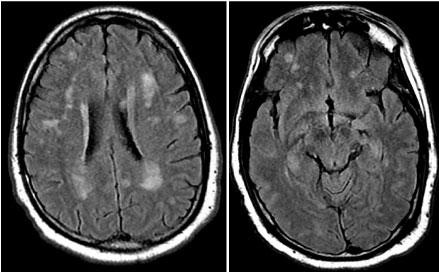 Figure 2: MRI of the brain upon readmission. View Figure 2
Figure 2: MRI of the brain upon readmission. View Figure 2
 Figure 3: Repeat MRI of the brain showing worsening septic emboli. View Figure 3
Figure 3: Repeat MRI of the brain showing worsening septic emboli. View Figure 3
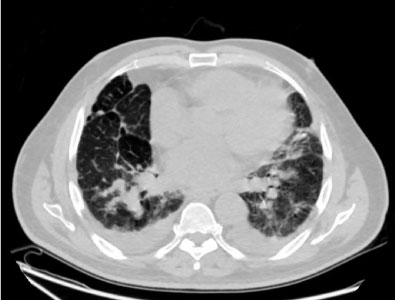 Figure 4: Repeat CT of the chest showing worsening pulmonary disease along with worsening pleural effusion. View Figure 4
Figure 4: Repeat CT of the chest showing worsening pulmonary disease along with worsening pleural effusion. View Figure 4
Nocardiosis is a rare infection caused by a weakly acid-fast, gram-positive bacteria. The infection can be localized or disseminated. Immunocompromised patients, including patients who are on long-term corticosteroids, organ transplant recipients or HIV/AIDS patients, are at a much greater risk of disseminated nocardiosis [2]. Although long-term corticosteroid therapy is a well-established risk factor [3,4], there are a limited number of case reports reporting sarcoidosis and disseminated nocardiosis, such as our patient. Of the reported cases, all patients were on long-term corticosteroid therapy at the time of infection and one case also involved a patient on azathioprine, similar to our patient. The dose of steroids varied between 10 mg per day to 20 mg per day. Two of the reported cases involved Nocardia farcinica; the same species that affected our patient [5-10].
Irrespective of a patient’s immune status, prompt diagnosis and initiation of treatment are important but often delayed because of challenges with diagnosis and its rarity. Extreme variability in clinical manifestations of nocardiosis compounds the challenge. The lungs are the most commonly involved site followed by the central nervous system (CNS) and then skin [11-13]. Given the association between chronic corticosteroid therapy and nocardiosis, the infection should be included in the differential for any such patient presenting with pulmonary, CNS or skin lesions.
Early identification of Nocardia speciation and antibiotic susceptibilities are important components of effective treatment. Sulfonamides, such as trimethoprim-sulfamethoxazole (TMP-SMX), are the most common first-line treatment, with relatively better outcomes documented in the literature. In cases with CNS involvement or dissemination, a multi-drug regimen is often necessary [2]. In this case, our patient was started on trimethoprim-sulfamethoxazole (TMP-SMX) and linezolid when initial tests indicated acid-fast bacteria. After cultures speciated Nocardia farcinica, he was placed on trimethoprim-sulfamethoxazole (TMP-SMX), amikacin and meropenem, which were eventually transitioned to imipenem prior to the discovery of isolate resistance. Prior to discharge he was transitioned to oral amoxicillin-clavulanic acid and moxifloxacin, with antibiotic therapy expected to continue for a year.
Although rare, nocardiosis is an infection that should be kept in mind in patients with sarcoidosis who are on long-term corticosteroids. The infection most commonly involves the lungs and in its most severe form can become disseminated. Timely diagnosis and treatment with appropriate antibiotics are crucial for a desirable clinical outcome.