Temporomandibular joint (TMJ) disorders are under-diagnosed in pediatric patients, and infantile TMJ luxation is a very rare condition. Luxation early in life can cause skletofacial problems, such as retrognathia, if it is left untreated for a long time. It is well known that severe retrognathia is one of the most common causes of sleep-disordered breathing (SDB).
The authors report a case of infantile TMJ luxation with secondary retrognathia associated with SDB, in which intraoral vertico-sagittal ramus osteotomy (IVSRO) was chosen over intraoral vertical ramus osteotomy and sagittal split ramus osteotomy for surgical correction.
IVSRO is an effective osteotomy technique for correcting skeletofacial deformities, especially in cases associated with TMJ disorders.
Temporomandibular joint disorders, Retrognathia, Snoring, Intraoral verticosagital ramus osteotomy, Oscillometry
Temporomandibular joint (TMJ) disorders are under-diagnosed in pediatric patients, and infantile TMJ luxation is a very rare condition [1]. Luxation early in life can cause skeletofacial problems, and it can result in severe retrognathia if it is left untreated for a long time [2].
The correction of retrognathia is always more technically difficult than the correction of prognathic deformities [3,4] because there is a minimal bony material with which to perform the osteotomy, and there may not be an adequate amount of soft tissue to cover the surgically elongated jaw, especially in cases of micrognathia [3]. In 1992, Choung introduced an alternative method for orthognathic surgery, intraoral vertico-sagittal ramus osteotomy (IVSRO). This method includes the beneficial characteristics of both sagittal split ramus osteotomy (SSRO) and intraoral vertical ramus osteotomy (IVRO) [5]; however, few case reports have described the treatment of mandibular advancement with IVSRO in patients with severe class II malocclusion.
It is well known that severe retrognathia is a common craniofacial feature of sleep-disordered breathing (SDB), such as heavy, habitual snoring and obstructive sleep apnea or hypopnea, and this article presents a case in which IVSRO was chosen over IVRO and SSRO to correct mandibular retrognathia with SDB secondary to bilateral infantile TMJ luxation.
A 12-year-old male presented to our outpatient clinic with a complaint of heavy, habitual snoring, and he had a history of nightly apneic episodes. He was also concerned that he had a small mandible. He had no history of trauma or symptoms or signs of inflammation of the TMJ. Clinical and radiographic examinations showed class II malocclusion with TMD as there is clicking and crepitation, and pain in the TMJ and masticatory muscle during mouth opening. Panoramic X-rays and computed tomography (CT) of the TMJ led to a suspicion of bilateral luxation of the TMJ. A decision was made to wait and see until the patient was 18-years-old and his mandible was fully mature. When he was 18-years-old, clinical and radiographic examinations showed mandibular retrognathia with an anterior overjet of around 10 mm, and a retruded mandible (SNB of 65°) and bilateral luxation of the TMJ were apparent on panoramic X-rays and CT of the TMJ (Figure 1 and Figure 2). Before surgery, the authors evaluated the patient's airway caliber using cephalometric radiography and assessed his airway resistance using impulse oscillometry (IOS). Arterial oxygen saturation (SpO2) was monitored continuously with a pulse oximeter during the nighttime (Table 1).
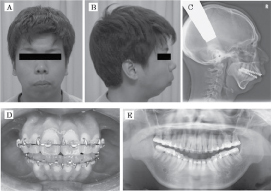 Figure 1: Initial front (A) and lateral views (B) initial lateral cephalometric radiograph (C), initial occlusion (D), and initial panoramic radiograph (E). View Figure 1
Figure 1: Initial front (A) and lateral views (B) initial lateral cephalometric radiograph (C), initial occlusion (D), and initial panoramic radiograph (E). View Figure 1
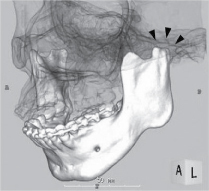 Figure 2: CT radiograph showing TMJ subluxation. View Figure 2
Figure 2: CT radiograph showing TMJ subluxation. View Figure 2
Table 1: Demographic, sleep study, IOS, and pharyngeal airway caliber data before and after surgery. View Table 1
The planned surgical procedure was to advance the mandible by 6 mm on the right side and by 8 mm on the left side combined with median mandibular point advancement of about 7 mm. The authors decided that IVSRO was the most appropriate technique in order to avoid compressive force being applied to the TMJ. IVSRO was performed, followed by skeletal maxillomandibular fixation for 2 weeks. After that, elastic therapy was begun, and training elastics were kept in place for 2 months. The procedure achieved good results; i.e., it abrogated the patient's snoring and SDB without causing neurological complications. A postoperative cephalometric radiograph showed widening of the pharyngeal airway and reductions in airway resistance on IOS and the degree of nocturnal oxygen desaturation at 2 months after surgery (Figure 3 and Table 1). The patient has been followed up for 2 years and the procedure appears to have been a success.
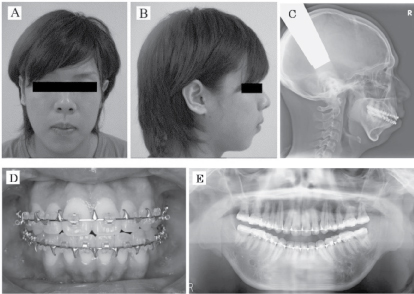 Figure 3: Final front (A) and lateral views (B), final lateral cephalometric radiograph (C), final occlusion (D), and final panoramic radiograph (E). View Figure 3
Figure 3: Final front (A) and lateral views (B), final lateral cephalometric radiograph (C), final occlusion (D), and final panoramic radiograph (E). View Figure 3
The proximity of the TMJ to other anatomical structures makes the diagnosis of TMD challenging, as it is difficult to pinpoint the origins of complaints. Luxation is usually defined as a self-reducing, partial dislocation of a joint due to traumatic overextension. When referring to the TMJ, this definition implies that the condyle passes anteriorly to the articular eminence during jaw opening. TMJ luxation, which is an asymptomatic complex rather than a disease, results from abnormally loose ligaments. In the growing facial skeleton, it is proposed that bilateral infantile luxation either congenital or acquired condition (e.g. significant trauma before 5-years-old which is early in life that most people cannot remember it) [6] retards or arrests condylar growth, which results in shorter vertical dimensions in the proximal mandibular segments and ultimately to mandibular deficiency due to bilateral TMJ degeneration. TMJ degeneration has been found to occur as early as 7 years of age, leading to arrested or regressive proximal mandibular segments, and patients suffering from this condition develop a progressive anterior open bite and skeletal problems, such as retrognathia or mandibular asymmetry [7].
SDB is associated with a variety of conditions that cause upper airway narrowing, and it was hypothesized that upper airway narrowing can occur in patients in whom retrognathia develops after TMJ destruction. As the patient in the present case complained of SDB, the authors decided to evaluate the patency of his pharyngeal airway using cephalometric radiography and also assessed his airway resistance functionally using IOS [8]. IOS employs low-amplitude pressure oscillation superimposed on quiet breathing to measure the impedance of the respiratory system, and it has begun to be used to assess airway obstruction in patients with SDB in recent years. In IOS, the respiratory resistance observed at 5 and 20 Hz (R5 and R20) are used as indices of total and central airway resistance, respectively, and increased upper airway resistance as measured by IOS is associated with increased susceptibility to airway narrowing and collapse. It is well supported theoretically and has the advantage of being convenient, non-invasive, and requiring minimal cooperation from the patient [9]. In this case, IOS was safely performed shortly after surgery, which revealed that the patient's airway resistance was significantly decreased. This change occurred in association with a widening of the pharyngeal airway and the disappearance of snoring.
SSRO and IVRO are the main techniques used to treat mandibular deformities. IVRO has a number of benefits compared with SSRO, e.g., it is associated with a lower incidence of inferior alveolar nerve damage and a shorter operation time, and it produces a favorable relationship between the condyle and the articular disc [10]. The most advantageous characteristic of IVRO is its condylectomy effect, whereby the anterior-inferior repositioning of the condyle results in an increase in the volume of the articular space, an improvement in the articular disc-condyle relationship, and reduced loading on the glenoid fossa. These effects may alleviate TMJ symptoms. Thus, IVRO is an excellent technique for treating TMJ symptoms in patients with mandibular prognathism. However, it is difficult to apply to mandibular advancement, probably due to the small contact area between the surfaces of the proximal and distal segments. In 1992, Choung introduced an alternative method for orthognathic surgery, IVSRO, which includes the beneficial characteristics of both SSRO and IVRO; however, few case reports have described the treatment of mandibular advancement with IVSRO in patients with severe class II malocclusion [5]. Recently, the authors obtained satisfactory results using IVSRO. Fujimura, et al. [11] concluded that IVSRO is potentially as useful as IVRO for the treatment of jaw deformity patients with TMD, and IVSRO can be used selectively in cases in which IVRO is contraindicated, such as those involving mandibular advancement, setback of > 10 mm, or horizontal and/or vertical rotation (counterclockwise rotation) of the distal segment. The authors chose to perform advancement using IVSRO in the present case, as they considered it to be the ideal technique for treating patients with mandibular deficiencies associated with TMD, as it involves an osteotomy that does not require rigid fixation of the condyle. The IVSRO was performed according to the method of Fujimura, et al. [11]. Similar to IVRO, the lateral aspect was exposed from the sigmoid notch to the antegonial notch. Bauer retractors were positioned in the sigmoid and antegonial notches. The temporalis tendon was mostly detached from the coronoid process. The lateral aspect of the subcoronoid process was reduced until the sigmoid notch could be identified (Figure 4A, arrow), when the lateral aspect of the coronoid process was flared out or enlarged. To avoid injury to the inferior alveolar nerve and maxillary artery, the medial aspect of ramus was also exposed carefully from the sigmoid notch region to the lingula and the posterior edge of the ramus similar to the process for SSRO, and a retractor was inserted between the soft tissue and the medial aspect of ramus. A corticotomy line was established from the mid-sigmoid notch or slightly anteriorly to it stretching to the antegonial notch. Full thickness cutting of the sigmoid notch was performed with a fissure bur or oscillating saw along the corticotomy line inferiorly until where the bone marrow was exposed (Figure 4B). The operator confirmed that the tip of the burr or saw cut the medial cortical bone by viewing from the medial aspect of ramus. Wedge-shaped decortication of the lateral aspect of ramus from the sigmoid notch to the antegonial notch was performed using a flat fissure bar (cylindrical in shape) parallel to the original sagittal plane, until where the bone marrow was exposed (Figure 4C and Figure 4D). Vertical osteotomy was performed along the original sagittal plane to the medial posterior border of ramus with an osteotome (a thin straight type blade with an edge width of about 8 mm) (Figure 4E). The cancellous bone was carefully split at the level of the foramen. In patients with TMD, the medial pterygoid muscle and part of the masseteric tuberosity should be detached as much as possible from the proximal segment, but in cases without TMD, stripping of masseteric tuberosity should be kept to a minimum. After osteotomy of the bilateral ramus, the medial pterygoid muscle attachments were separated from the proximal and distal segments. The distal segment could be moved freely, and the inner aspect of the proximal segment overlapped with the decorticated distal segment (Figure 4F). Rigid fragment fixation was not conducted in this case. Instead, maxillomandibular fixation (MMF) was applied with wires before suturing, and the wires were kept in place for 15 days postoperatively. The MMF period was similar to those reported in previously published studies [11-13], but the increased area of contact between the segments of the osteotomy permitted improved osseous healing. An interocclusal splint was used in this case, as at the authors' institution it is considered that interocclusal splints provide more balanced occlusion and so improve the final outcome. Fujimura, et al. [14] described the use of splints in all of their patients while Júnior, et al. [13] reported that at their institution interocclusal splints are only used in cases in which premature contact cannot be prevented before surgery or in cases involving segmental maxillary surgery.
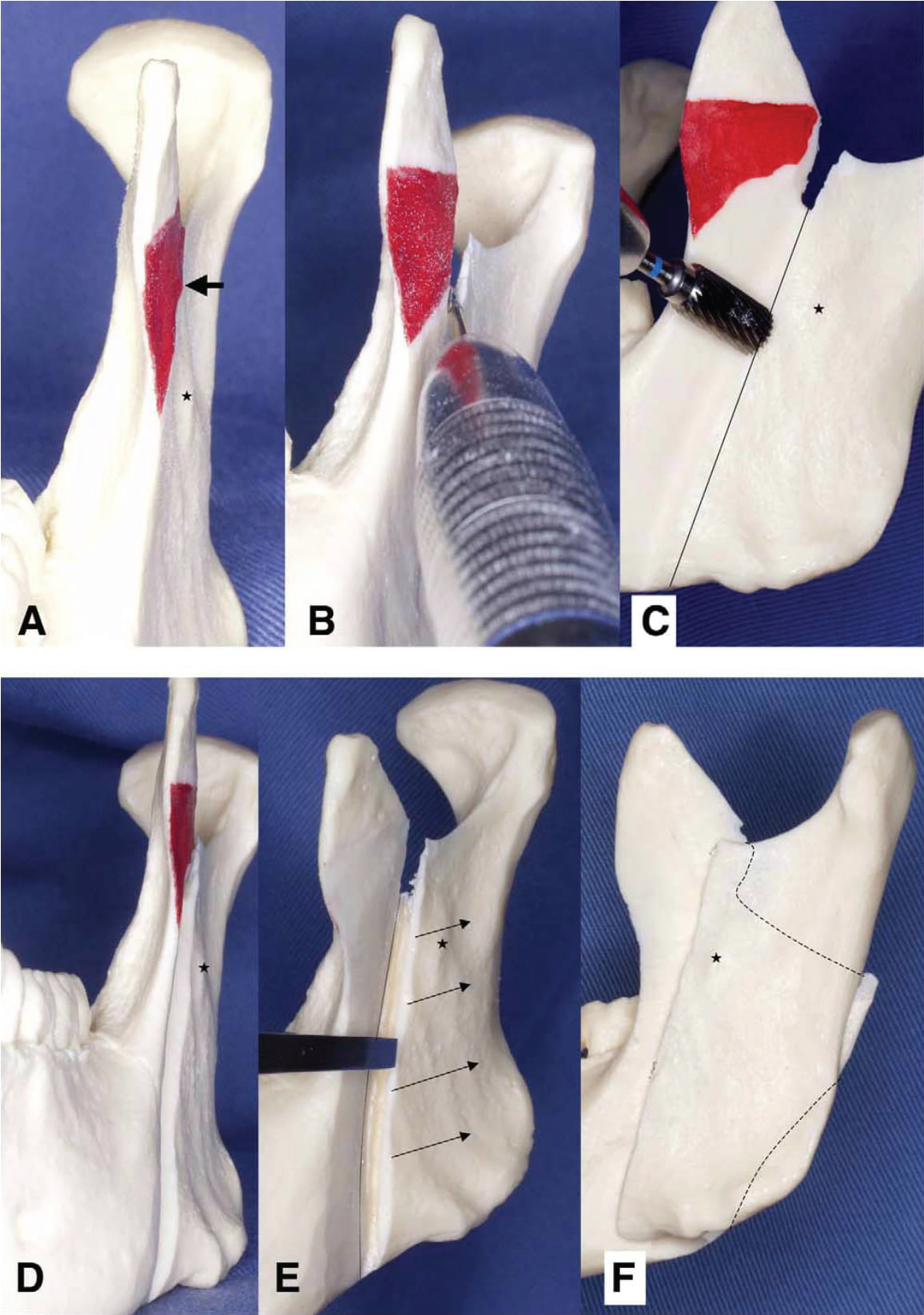 Figure 4: Surgical procedure of intraoral verticosagittal ramus osteotomy using a mandibular model.
Figure 4: Surgical procedure of intraoral verticosagittal ramus osteotomy using a mandibular model.
(A) The lateral aspect of the subcoronoid process was reduced until the sigmoid notch could be identified (arrow); (B) Full-thickness cutting of the sigmoid notch was performed with a fissure bur or oscillating saw along the decortical line inferiorly until where the bone marrow was exposed (about 10 mm); (C, D) Wedge-shaped decortication of the lateral aspect of ramus from the sigmoid notch to the antegonial notch using a flat fissure bar (cylindrical in shape) was performed parallel to the original sagittal plane, until the bone marrow was exposed; (E) Vertical osteotomy was performed with an osteotome to the medial posterior border of ramus; (F) Following osteotomy of the bilateral ramus, the distal segment could be moved freely and was overlapped by the proximal segment. Asterisks indicate antilingual prominence. Fujimura, et al. [11] IVSRO in Skeletal Deformity Patients With TMD. J Oral Maxillofac Surg 2004. View Figure 4
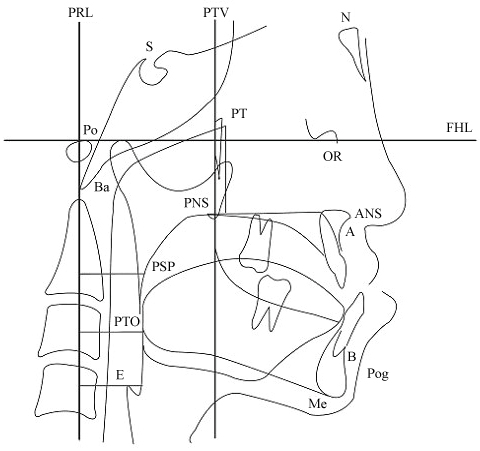 Figure 5: Landmarks and reference lines used in the cephalometry.
Figure 5: Landmarks and reference lines used in the cephalometry.
Measurements of pharyngeal morphology: 1. PRL-PSP distance; 2. PRL-PTO distance; and 3. PRL-E (the horizontal distance between PRL and the frontal wall of the pharyngeal airway passing E). Cephalometric landmarks: N: Nasion; S: Sella; OR: Orbitale; Po: Porion; ANS: Anterior nasal spine; PNS: Posterior nasal spine; Pog: Pogonion; Ba: Basion; Me: Menton; A: Point A (the deepest anterior point in the concavity of the anterior maxilla); B: Point B (the deepest anterior point in the concavity of the anterior mandible); PSP: The most posterior point of the soft palate; PTO: The point crossing the inferior mandibular border in the posterior area of the tongue; E: The most superior point of the epiglottis; FHL: Frankfort horizontal line (the line between the porion and orbitale); PTV: The line perpendicular to the Frankfort horizontal line passing through the pterygoid; and PRL: The line perpendicular to the Frankfort horizontal line passing through porion. View Figure 5
Hashami, et al. [12] reported that the overall complications rate of IVSRO is 11%, with injuries to the inferior alveolar nerve (IAN) occurring in 3.8% of cases. Hashami, et al. encountered similar complications to those reported by Júnior, et al. [13], including bad splits and bleeding; however, they did not report any injuries to the IAN. There were no complications in the present case.
IOS is a useful, non-invasive, and simple tool that can be used to sensitively estimate airway resistance before and after orthognathic surgery. Furthermore, IVSRO exhibits a low morbidity rate and is a versatile and efficient osteotomy technique with a low complications rate. This osteotomy technique should be considered when treating skletofacial deformities, including mandibular advancement and setback, especially in cases involving TMD.
The authors declare that there are no conflicts of interest regarding the publication of this article. The authors alone are responsible for the content and writing of the paper. In addition, the authors have no financial interests related to the subject matter or materials discussed in this manuscript.
This study was not supported by funding from any organization.