Rehabilitation of angle class III deformity concomitant with oligodontia with great functional, esthetic and social impairment for the patient needs a combined orthodontic-surgical treatment. To achieve secure, quick and stable dental and facial rehabilitation, backward planning with cone-beam CT navigation best supports the multidisciplinary approach. Here we show longtime stability of more than 5 years after thoroughly planning, bimaxillary osteotomy with an implant guided transpalatal distractor (Surgi-Tec All-in-One), conceptional extractions and alveolar augmentation in a male patient with ICD10 (K00.0; K07.1). The diagnosis included craniomandibular malfunction, dysgnathia class III, maxillary retrognathia with horizontal and transverse narrowing of the maxilla, mandibular prognathia with lingual tipping of the mandibular front teeth, multiple missing of permanent teeth and hypodontia of deciduous teeth with cones and platelet deficiency and thrombocytopenia.
The treatment included orthodontics with multi-brackets in the mandible, maxillofacial surgery with Le-Fort-Osteotomy and reconstruction and augmentation of the maxilla with a bone graft of the iliac crest with vertical subtotal separation, Obwegeser/Dal Pont-osteotomy, modified according to Hunsuck-Epker in the mandible, implantation and prosthetics.
The result was good osseointegration > 80 on the Ostell ISQ-scale and the successful healing of the augmentation even for the enossal implants. Facial proportions and the profile expression showed harmonized. The dental situation was satisfying in function as well as in the esthetic aspect. At the follow-up dates after 6, 12, 18, 24, 36 and 60 months the results remained stable. The patient was highly satisfied. Discussion of methods is performed additionally.
Angle class III deformity concomitant with oligodontia means great functional, esthetic and social impairment for the patient. Not only chewing but the complete facial expression and speech can be involved, with a big negative impact on the patient's quality of life [1-33]. For this, especially in severe cases of concomitant class III malocclusion and oligodontia a combined orthodontic-surgical treatment is indicated and has shown best success in a lot of cases [4-8]. The facts of missing teeth, insufficient stability and atrophy of the alveolar bone and the aim to harmonize the facial structures with esthetic reconstruction, need comprehensive thorough planning. Interdisciplinary cooperation between orthodontics, oral and maxillofacial surgery and prosthetics have been proved to lead not only to best but also to time saving success [9-11].
For corrections of transverse maxillary deficiencies, the transpalatal distraction is used successfully for years. The nowadays common technique of palatal widening with a final space between the central incisors was first described by Derichsweilerin the year 1954 [12]. During the following 30 years a lot of experiments with different and modified devices have been published for example by Steinhäuser [13] and Glassmann, et al. [14] so far using a dental fixation only. However, in adult patients, palatal distraction of the maxilla needs fixation in the palate and not only along the teeth to avoid cortical decay and root resorptions because of teeth movements. The first bone-borne device with a titanium implant in the palatal bone developed by Surgi-Tec was published by Mommarts [15] and since then has been proved well [16-18].
A combination of bimaxillary osteotomie with palatal distraction, necessary extractions and alveolar augmentation can be the best procedure, as was shown formerly and also in the presented case [19-21]. Therefore, the implant guided transpalatal distractor (IGPD) is an improved instrument for jaw stabilization and transversal elongation in adult patients with severe class III malocclusions [20-23]. The gentle distraction usually in combination with a Le Fort-osteotomy leads to supporting osteogenesis and therefore longtime stability of the additional procedures like implant insertion [17,19,24-27].
To achieve secure, quick and stable dental and facial rehabilitation in such complicated anatomic situations, backward planning with 3D navigation best supports the multidisciplinary approach. Cone-beam CT (CBCT) with flat-panel detectors and devices for dose reduction has been proved first in oncology and angiography, but nowadays is used widely in maxillofacial practice [28]. Additional planning software like NobelGuide® (Sweden) with Procera [29-33] or SIMPLANT® (module craniofacial, Materialize, Belgium) [27,34,35] facilitate planning and lead to precise positioning of the implants especially in the esthetic zone in implant supported reconstruction [27,32,36-40].
The procedure is minimal invasive with the possibility to insert dental and facial implants in one time. More than this, for the patient, the CT-guided planning and surgery means reduction of time of surgery as well as reduction of trauma and postoperative complications, which was confirmed by several studies, especially the randomized studies of [41-46].
The aim of our all-in-one concept was to reduce the necessary orthodontic as well as the surgical efforts but always on the background of the best possible dental and prosthetic rehabilitation. With the presented case, we show longtime stability of more than 5 years after thoroughly planning, bimaxillary osteotomy with an implant guided transpalatal distractor (Surgi-Tec All-in-One), conceptional extractions and alveolar augmentation in a patient with class III malocclusion and oligodontia.
In November 2007, a male patient with ICD10 (K00.0; K07.1) asked for treatment. The diagnosis included craniomandibular malfunction, dysgnathia class III, maxillary retrognathia with horizontal and transverse narrowing of the maxilla, mandibular prognathia with lingual tipping of the mandibular front teeth (Figure 1). Additionally, we diagnosed multiple missing of permanent teeth and hypodontia of deciduous teeth with cones (Figure 2, Figure 3 and Figure 4). Systemically, the patient suffered from platelet deficiency and thrombocytopenia.
 Figure 1: Extraoral view of a 23-old-male patient with oligodontia and class III anomaly before treatment.
View Figure 1
Figure 1: Extraoral view of a 23-old-male patient with oligodontia and class III anomaly before treatment.
View Figure 1
 Figure 2: Intraoral view pf the patient: Maxillary retrognathia, multiple missing teeth and hypodontia of deciduous teeth before treatment.
View Figure 2
Figure 2: Intraoral view pf the patient: Maxillary retrognathia, multiple missing teeth and hypodontia of deciduous teeth before treatment.
View Figure 2
 Figure 3: Orthopantomography before treatment.
View Figure 3
Figure 3: Orthopantomography before treatment.
View Figure 3
 Figure 4: Cephalometric X-ray (lateral view) with facial analysis before treatment.
View Figure 4
Figure 4: Cephalometric X-ray (lateral view) with facial analysis before treatment.
View Figure 4
We chose a combined treatment consisting of orthodontics with multi-brackets in the mandible, maxillofacial surgery with Le-Fort-Osteotomy and interpositioning of a bone graft of the iliac crest in the maxilla, and at last Obwegeser/Dal Pont-osteotomy, modified according to Hunsuck-Epker in the mandible. Implants and prosthetics should be performed afterwards.
The whole procedure included Le-Fort I-Osteotomy, reconstruction and augmentation of the maxilla as interpositioning with vertical subtotal separation, osteotomy to shift the lower facial part with separation in the ascending part and in the horizontal mandible part, and finally a secondary palatal bony transplant of the iliac crest.
After CBCT analysis of the dental and skeletal anomalies and analysis of lateral cephalograms concerning skeletal and soft tissue profile, the patient got presurgical orthodontic treatment. Because of the low dento-alveolar stability, the first surgical intervention concerned the transpalatal distraction. Surgery took place in our clinic for esthetic dental medicine and facial surgery, Dortmund, Germany. After removal of a 1 cm × 0.3 mm piece of gingival transpalatal distraction device was inserted on implants regio palatal 12, 22, 16, 26 (Figure 5 (IGPD)). We used Surgi-Tec TPD All-in-One 2.5 mm, which has been proved to fit well for transverse palatal distraction. Anesthesia was done by Ultracain DS forte. The distractor was fixed with osteosynthesis screws. First activation was performed for 2 mm, second one for 1 mm and the third one for 10 mm. An iliac cortico-spongy chip was prepared and inserted in the palate extension.
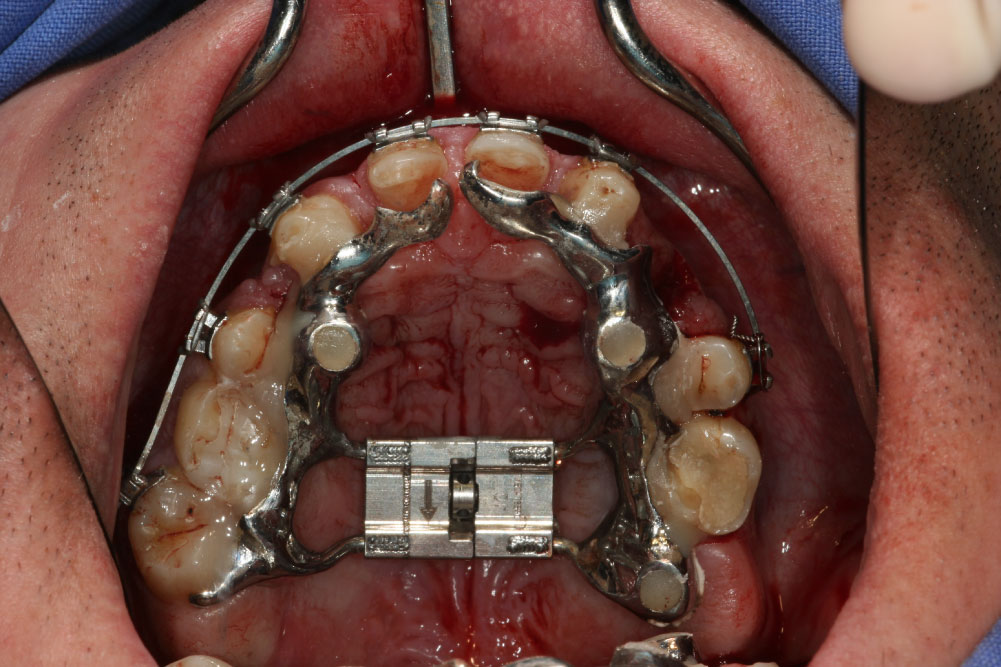 Figure 5: Custom made implant guided palatal distractor before activation.
View Figure 5
Figure 5: Custom made implant guided palatal distractor before activation.
View Figure 5
After 6 months of consolidation and ossification, the second surgical intervention was planned and performed as corrective osteotomy, beginning with the mandible. In course of the osteotomy according to Obwegeser/Dal Pont,the mandible was set back to the maxilla by splint for 8 mm, and fixed with one plate with cortical screws. After this, the maxilla was set forward by Le-Fort-I-Osteotomy for 12 mm and fixed, too. The first palatal widening 6 months ago turned out to be insufficient, so we decided to split the maxilla again along the sutura palatina mediana with activation for 8 mm. A second bone graft from the iliac crest was now used for alveolar augmentation in region 13-21 for a discontinuous palatal widening (Figure 6).
 Figure 6: Maxillary osteotomy (LeFort I) and discontinuous palatal distraction; sagittal interpositioning of iliac crest graft.
View Figure 6
Figure 6: Maxillary osteotomy (LeFort I) and discontinuous palatal distraction; sagittal interpositioning of iliac crest graft.
View Figure 6
In preparation for the planned implantations, gaps were needed in the maxilla as well as in the mandible. For this, we lateralized, medialized and distalized the corresponding teeth, so called orthodontic volume optimizing [47], (Figure 7a and Figure 7b). In the meantime, the cones of teeth 31/41 and 11/21 could be extracted during the time of 12 months. The plates for osteosynthesis could be removed and the alveolar ridge of maxilla and mandible was augmented with the iliac bone graft in regio 11-13, 23/24, 31/41, and 35 (Figure 8 and Figure 9). After that, we inserted implants in the maxilla in regio 16, 14, 12, 22, 11, 21, 24, and 26 and in the mandible in regio 36, 34, 31/41, 44, 46 (SI Cace, SIConepiece for teeth 14 + 34). Concerning the teeth 31/41, a bone split was set (Figure 10). The other teeth were pre-grinded as preparation for the later prosthetics of crowns and bridges. A model was prepared in the laboratory.
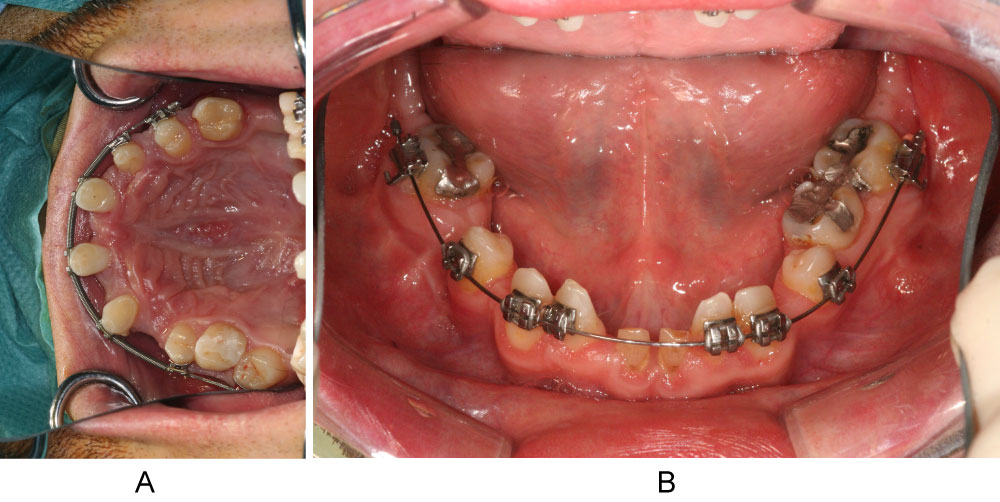 Figure 7: a,b) "Orthodontic volume optimizing" by lateralization, medialization and distalization of corresponding teeth.
View Figure 7
Figure 7: a,b) "Orthodontic volume optimizing" by lateralization, medialization and distalization of corresponding teeth.
View Figure 7
 Figure 8: Secondary alveolar ridge augmentation with onlay-grafts from iliac crest.
View Figure 8
Figure 8: Secondary alveolar ridge augmentation with onlay-grafts from iliac crest.
View Figure 8
 Figure 9: Cephalometric X-ray (lateral view) after bimaxillary osteotomy and bone augmentation.
View Figure 9
Figure 9: Cephalometric X-ray (lateral view) after bimaxillary osteotomy and bone augmentation.
View Figure 9
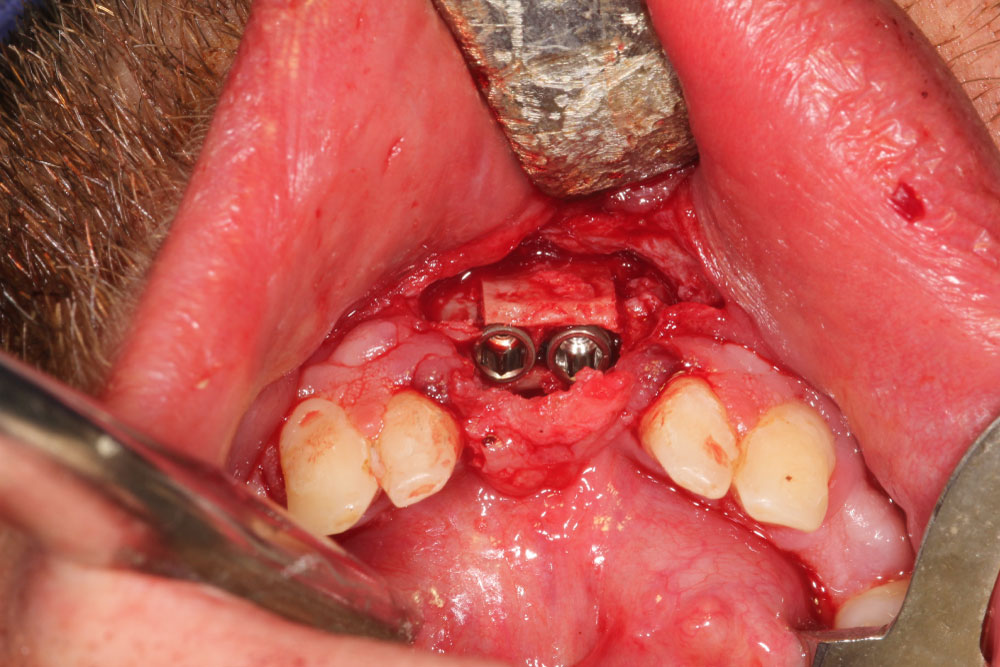 Figure 10: Bone split region 31, 41 and dental implantation 31, 41.
View Figure 10
Figure 10: Bone split region 31, 41 and dental implantation 31, 41.
View Figure 10
After 6 months of healing, the implants could be revealed and individual gingiva formers were incorporated to shape the soft tissue (Figure 11).After additional three months, the final prosthetic device of high esthetic standard could be incorporated: Circonia for the maxilla and SiO2 ceramics for the mandible (Figure 12, Figure 13, Figure 14 and Figure 15).
 Figure 11: Clinical situation after selected tooth extraction and implantation in region 16, 14, 12, 22, 11, 21, 24, 26.
View Figure 11
Figure 11: Clinical situation after selected tooth extraction and implantation in region 16, 14, 12, 22, 11, 21, 24, 26.
View Figure 11
 Figure 12: Extraoral smile/view with long-term provisional bridges for vertical bite stabilization.
View Figure 12
Figure 12: Extraoral smile/view with long-term provisional bridges for vertical bite stabilization.
View Figure 12
 Figure 13: Intraoral maxillary situation after cemented single crown restorations on natural teeth and implants.
View Figure 13
Figure 13: Intraoral maxillary situation after cemented single crown restorations on natural teeth and implants.
View Figure 13
 Figure 14: Intraoral mandibular dental restoration with single crowns on natural teeth and implants.
View Figure 14
Figure 14: Intraoral mandibular dental restoration with single crowns on natural teeth and implants.
View Figure 14
 Figure 15: Orthopantomography at the end of treatment. Implant 14 not charged.
View Figure 15
Figure 15: Orthopantomography at the end of treatment. Implant 14 not charged.
View Figure 15
Osseointegration was measured by OstellISQ, which determines the vibration frequency of the implant by Resonance Frequency Analysis (RFA) and a stability scale. The stability quotient scale counts between 1 and 100, with ISQ 1 corresponding approximately to 1,000 Hz and ISQ 100 corresponding approximately to 10,000 Hz in a close to linear way. By comparison analyses of resonance frequency changes, the implant stability can be determined. The software enables to set correlations between bone-to-implant contact (BIC) and implant stability [48,49]. Additionally, we evaluated the maxillofacial proportions and the dental function and finally patient's satisfaction after 6, 12 18, 24, 36 and 60 months.
We measured good osseointegration > 80 on the Ostell ISQ-scale after this comprehensive corrective osteotomy and the successful healing of the augmentation even for the enossal implants. Facial proportions and the profile expression showed harmonized. The dental situation was satisfying in function as well as in the esthetic aspect (Figures 3). The dentolabial analysis showed good visibility of the teeth in neutral position with cutting edges of 2 mm. Interinzisal lines and middle facial lines assorted well, occlusion and commissure line corresponded. The mandibular-maxillary relation was fixed as central occlusion with maximum intercuspidation Figure 3.
At the follow-up dates after 6, 12, 18, 24, 36 and 60 months the results remained stable. The patient was highly satisfied.
Maxillary retrognathia with horizontal and transverse narrowing of the maxilla, is one of the indications for distraction osteogenesis, besides other types of hypoplasia. Distraction by a transversal palatal device with the aim of osteogenesis in the new formed alveolar gap offers a wide range of movements and in general good post-operative stability. Though it is common among maxillofacial surgeons, methods vary.
Alveolar distraction osteogenesis not only can correct maxillofacial deficiencies but also creates stability for later dental implantation [50,51]. Mandibular osteotomy according to Obwegeser/Dal Pont lately has been proved to be safe and reliable in a study of [52] Al-Nawas, et al. with 400 patients. Corrective osteotomy for long is common in orthopedic surgery but rarely has been published for correction of severe maxillofacial deficiencies. Corrective maxillofacial osteotomy notably after alveolar distraction osteogenesis demands thorough planning and exact application because of risks of complications that each step of surgery includes [53] Ettl, et al. Moran, et al. [54]. However, the good esthetic and functional results including implant stability of our presented case therefore show that this comprehensive procedure can lead to satisfying results as well in functioning as in the esthetic aspect.
In the past 10 years, the bone-borne distractor has been established in clinical practice. Though the tooth-borne device is still used, in comparison studies results achieved with a bone-borne distractor compared to a tooth-borne devices how a tendency towards greater space gain, lesser complications with especially fewer root resorptions, and easier handling by the patient [55-60]. Our longtime results with the bone-borne Surgi-Tec All-in-One device confirm the expert knowledge especially in highly complicated cases of maxillofacial deficiencies.
In most cases of usage of a palatal distractor, patients suffer from cleft lip and palate. Other indications are obstructive sleep apnoea or Crouzon syndrome. The majority of publications report treatment of children and adolescents, most of them using an external rigid distractor. There are few cases published concerning multiple maxillofacial deficiencies in adults indicating transpalatal distraction, corrective osteotomy of maxilla and mandible and dental implantation. And among those, there are rare cases using an internal distractor and gathering follow-up data over several years [20,61-65] found higher stability after distraction osteogenesis than after conventional orthognatic surgery. Jakobsone, et al. [65] reported about good stability three years post bimaxillary surgery of class III patients with a slight tendency of mandibular relapse. The results of the study of Hirjak, et al. [66] with 15 adult class III - patients are in line with our results: After 60 months the authors confirmed good stability and satisfaction after distraction osteogenesis.
The measurement of the implant stability quotient (ISQ) in our presented case led to good results of osseointegration even in the augmented areas. The technique of resonance frequency analysis (RFA) with use of the ISQ has been approved. Some studies found significant correlations between bone volume and ISQ, so that this method seems to be suitable for osseointegration evaluation [66-70]. It is a minimal invasive device with rapid delivery of results and especially suitable for patients with multiple maxillofacial problems and procedures.
Usually, cone-beam CT (CBCT) is used for follow-up evaluation and yields exact results especially in sophisticated procedures like corrective osteotomy [57,58,71-74]. But moreover, CBCT offers the maxillofacial surgeon a wider range of facilitations and prediction of the best possible results, with the final benefit of higher patient satisfaction and stability of results.
CT data give real geometric transformations showing exact information about bone quality and structure. The impression of bone architecture and height of the alveolar ridge, vascularization, real bone volume and jaw geometries, is of exceptional use for the maxillofacial surgeon and facilitates planning especially of sophisticated restauration and rehabilitation. The three dimensional information assure to set even temporary implants for example for the IGPD exactly and to use just the given volume space. By this means an immediate prosthetic loading is possible, which provides a time saving procedure and for the patient therefore leads to reduction of pain and complications [32,33,75,76].
An important approach is the use of CBCT for operation planning and for navigation before implantation with help of a drilling template. The tool SimplantPro (Materialise) enables to send the data to the main computer or to work with the CBCT-data in the laboratory. Last but not least, cone-beam CT offers to simulate each step of the planned procedure. That comprises implant length and diameter, number of dental implants, type of facial implants, augmentation and method. The simulation before real surgery takes off patient's fears and ensures the surgeon to choose the best fitting method and device. Especially for profile optimizing surgery planning with good prediction can be done.
Comprehensive surgical procedures to change facial structures in line with numerous prosthetic rehabilitations, demand a close multidisciplinary cooperation to achieve the desired functional and esthetic improvements. More than this, exact and detailed planning of each necessary step is essential, especially in cases of changes of the facial structures. CBCT planning and navigation software facilitate and shorten the procedures with the final benefit for the patient of lower fear and pain and less complications. With the option to plan and to simulate all surgical and implantological steps, even complicated anatomic preconditions can be integrated and managed.
At the end, exact planning and visualization shorten time of surgery and complete therapy and is necessary in complex dental and facial cases. Here we could show that bimaxillary osteotomy together with palatal distraction in an all-in-one concept on the background of CBCT planning and navigation lead to good longtime results.