Facial aesthetics has a meaningful relationship with the capacity of people to form interpersonal relationships, which can lead to cases of harassment when there are severe facial disharmonies. For a long time, orthognathic surgery has been indicated in patients whose growth has ended in order to achieve more stable and predictable results over time. However, there are cases where psychosocial stress due to dentofacial deformities makes necessary to intervene patients at a younger age. This review article aims to describe the surgical management and stability of growing patients through orthognathic surgery attained from the reported English literature during the last 50 years. From all the information gathered, a surgical protocol has been proposed at the end of this article, based on the expected results and the surgical technique carried out, in order to obtain the most stable and predictable results possible. Despite the lack of existing evidence regarding this subject and the quality of these studies, orthognathic surgery in growing patients is a surgical procedure that should be performed in cases where patients could develop more severe problems in the future, mainly in the psychosocial aspect.
Orthognathic surgery, Growth, Development, Dentofacial deformities
The management of growing patients with severe dentofacial anomalies often presents a challenge for both orthodontists and surgeons, largely due to the lack of published articles regarding the times of various surgical procedures, their effects on the continuity of dentofacial development and its stability over time, which is why orthognathic surgery is usually indicated after the end of its growth.
However, there are situations in which postponing surgical intervention may lead to several problems, whether functional or aesthetic, the latter being one of the main indications to anticipate the surgical procedure for psychosocial reasons, both in the short and long term, where it has been seen that facial appearance is a important factor in the determination of interpersonal relationships.
Following this, it is essential to possess a detailed knowledge of normal craniofacial growth, where the vertical, sagittal and transversal maxillary development differs both in their peak of development and the finalization of it. Likewise, the different surgical techniques used in orthognathic surgery allow the surgeon, in certain occasions, a management of the maxillofacial growth axes.
Due to this, it becomes necessary to carry out and individualized evaluation of each of these patients to determine an adequate diagnosis and phase of maxillofacial growth in which it is found. This information will allow us to define a surgical treatment plan in the short and long term, establishing a sequence of systematized surgical procedures, responding to the problems of each patient in particular.
A structured sensitive literature search was performed in multiple web-based search engines and bibliographic databases that catalogue published research: PubMed/MEDLINE, EBSCO Dentistry & Oral Science Source, Scopus and The Cochrane Library (until June 2018). The MeSH terms used were "Osteotomy, Le Fort", "Orthognathic Surgery", "Osteotomy, Sagittal Split Ramus", "Adolescent", "Child", "Syndrome", "Cleft Palate" and "Adult". The used non-MeSH terms were: "Growth", "Development", "Early" and "Cleft", with boolean operators "AND", "OR" & "NOT" (Table 1). There was no publication date filter, however language filters were applied to the search (english/spanish). Additionally, a manual search for references, to explore filtered findings, was conducted. A total of 18 articles, published between 1979 and 2017 were included in this review (Figure 1). Articles that included growing patients with diagnosis of dentofacial anomalies of non-syndromic origin treated by orthognathic surgery were included, while those that included cleft patients or an adult population, without distinction in the sample, were discarded. The collected data was then organized and validated using the Oxford Centre for Evidence-based Medicine (CEBM)-Levels of Evidence criteria and its corresponding recommendation grades. The CONSORT statement [1] was used for reporting randomized clinical trials, the STROBE statement [2] for reporting observational studies, and the CARE statement [3] for case reports.
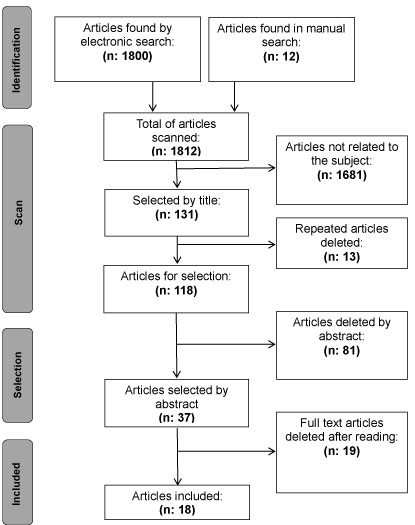 Figure 1: Articles selection flow chart.
View Figure 1
Figure 1: Articles selection flow chart.
View Figure 1
Table 1: Search strategy. View Table 1
Our systematized structure literature search identified 18 articles, categorized as follows: 1 clinical trial, 11 observational studies, 4 cases reports and 2 narrative reviews. These articles were classified according to 1) Treated dentofacial deformity; 2) Surgical technique and 3) Patients mean age at the moment of the surgery (Table 2). Eleven articles did not make a distinction between male and female patients, which have different growth peaks. Regarding the age of the patients at the moment of surgery, Mojdehi, et al. [4] has the lowest average age (12.8 years), meanwhile Wolford, et al. [5] has the highest (17.5 years). The amount of maxillary anomalies is 16 (47%), where the most prevalent is the vertical maxillary hyperplasia (50%) in the maxilla and the mandibular hypoplasia (39%) in the mandible, followed closely by the mandibular hyperplasia (33%), from the 18 mandibular anomalies. For the treatment of maxillary deformities, the most used technique was the Le Fort I maxillary osteotomy (67%), followed by the anterior maxillary osteotomy (27%) and the horseshoe maxillary osteotomy (1%). On the other hand, the most commonly used mandibular techniques were the sagittal split ramus osteotomy (36%), the vertical ramus osteotomy (16%) and the genioplasty (16%). The complementary use of the high condylectomy technique was described in 3 articles.
Table 2: Articles selection results. View Table 2
The current evidence contains a large number of articles that mention the surgical techniques used in orthognathic surgery; however, the greater number of these procedures are carried out in adult patients who have already completed their growth, which is why there is not enough studies regarding surgical protocols in patients who haven't completed their development and who, for many reasons, should be treated. Among the reasons that can lead to a premature intervention in this kind of patients, it can be found the excessive dentofacial anomalies, functional problems, and the psychosocial stress, being the last one the main reason for surgery [6-9]. In these cases, self-esteem, physical affection and the ability to establish interpersonal relationships can be affected, with serious complications in the long term, where a relationship between being a victim of bullying during childhood and suicide attempts along life has been observed, with an odds ratio of 3.75 [10]. It has also been established that the social and psychosocial influence of dental and facial appearance is an important factor in the perception of people regarding the kindness, social status, popularity and intelligence of an individual, with teeth being the main mocking reason in bullying [11].
According to Wolford, et al. [12], when treating these kind of anomalies, regardless of the surgical technique performed, the vertical growth will remain unaffected, contrary to the development in the sagittal axis. Regarding the stability after maxillary replacement in patients with residual growth, the maxillary reposition is a stable procedure during growth in patients between 10 and 16 years of age, seen at a 12-78 months post-surgical follow-up, and even early intervention may favor the disproportionate growth characteristic of vertical excess [13]. The reduction of the vertical height produces a mandibular self-rotation and decrease of the lower facial third [13], indicative of adaptive compensations due to the mandibular surgical replacement and self-rotation, without changes in the vertical growth pattern both maxillary and mandibular [14].
Finally, a relationship between postoperative stability and the type of fixation used was found, where in a study of 48 patients with an average age of 14.63 years (DE = 1.37 years), it was concluded that the segmented osteotomy has little or null effect on maxillary vertical growth, and that rigid fixation provides superior stability in the sagittal axis in the long term, when compared with wire fixation [14].
Only 2 articles evaluate the maxillary excess in the sagittal axis [12,13], where both stated that the continuity of growth in this axis is dependent on the surgical technique performed, where this is related to the integrity of the septal cartilage. This could mean that the Le Fort I maxillary osteotomy would completely inhibit sagittal development, while the horseshoe maxillary osteotomy (dentoalveolar osteotomy) would allow continuity in growth. Despite this, none of the authors supports this theory with post-operative growth studies, therefore it is correct to indicate that evidence is needed to support this hypothesis.
Is mainly characterized by a deficit in the growth in the sagittal axis of the maxilla, being necessary in many cases a new surgical intervention once the development is finished. Despite this, there are situations where it is necessary to carry out orthognathic surgery due to functional alterations, such as the psychosocial stress that patients present due to dentoskeletal anomalies [7,9]. In a series of cases [7] where 6 patients with severe facial anomalies were analyzed, 5 were skeletal class III and presented severe functional and psychosocial problems, which is why they were operated at approximately 15 years, with a new class III in the long term due to continuous mandibular development. Despite this, at the time of finishing the growth, only 1 patient was re-intervened, mainly due to the satisfaction of the rest with the results achieved and the greater stability of the new skeletal class III.
In cases where there is an accelerated growth pattern at the mandibular level, it is recommended to perform a sagittal split ramus osteotomy (SSRO) with a complementary high condylectomy, in order to stop the growth. It can also be performed a single bilateral high condylectomy when there are no alterations in the mandible at that point [5,7,12,15]. Studies comparing the long-term stability of a group of patients where orthognathic surgery (Le Fort I maxillary osteotomy + SSRO) was complemented with a high condylectomy in relation to those which only orthognathic surgery was performed, showed that patients belonging to the first group obtained stable results in the long term, even in cases where the age of patients does not exceed 14 years; while those of the second group presented higher recurrence [5-7].
When analyzing the long-term results of pediatric patients after bilateral SSRO, it has been seen good skeletal balance and an harmonious posterior dentofacial development [16,17]. When comparing the stability of these patients with adults, in those patients who had already finished their growth, achieved more stable results in the long term, however, from the psychosocial point of view, changes were similar [18]. In cases where there is a pattern of insufficient mandibular growth, it has been described the adolescent internal condylar resorption (AICR) as a cause [19,20]. When comparing the mandibular growth pattern after the removal of the bilaminar tissues surrounding the condyles and bimaxillary orthognathic surgery with healthy patients, it was possible to determine that the subsequent development was normalized [19]. The removal of the bilaminar tissues is performed because there is an increase in receptors that may predispose an exaggerated response in this tissue [19]. Galiano, et al. [20] in a retrospective study conducted in 24 patients with an average age of 16.5 years, analyzed the results of AICR by means of disc replacement and orthognathic surgery. It was seen a significant reduction in temporomandibular and facial pain, along with fewer headaches. Improvements in the chewing function and a good skeletal and occlusal stability were maintained in the long term [20].
From all this data gathered, a surgical protocol has been proposed for the treatment of different dentoskeletal anomalies and their various combinations when accompanied by other alterations
One of the main limitations of the present review is the quality of the selected articles. Despite having carried out a sensitive search in multiple databases and search engines, the information collected dates from many years back, with unstandardized variables and shortcomings in the report of information, such as the age of each patient at the time of surgery, type of surgical technique performed and the orthodontic treatment duration. On the other hand, the level of evidence in these articles consist mainly of observational studies, partly due to the difficulty of carrying out randomized clinical trials in this kind of patients due to the ethical considerations that this implies.
Although it is advisable to wait for patients to finish their growth to perform surgery, there are cases where it is not possible due to psychosocial factors that are positively altered after surgical interventions. Regarding the available evidence, although this is scarce and the available articles date back many years, with small samples and a little impact, these tend to yield similar results in terms of long-term stability, with multiple reports of cases with acceptable results regarding the improvement in the psychosocial aspect and the increase in the quality of life of these patients. Due to the differences in the type and magnitude of the dentoskeletal anomaly of each patient, it is necessary to carry out individual evaluations where the altered growth patterns are defined and the influence of these alterations in the psychosocial profile of each individual. Because of the circumstances in which these interventions are carried out (psychosocial stress), it is important to manage the expectations of both parents and children, and to warn about the possibility of a second surgical intervention after the cessation of growth.