Loeys-Dietz Syndrome (LDS) is a rare autosomal dominant connective tissue disorder. Patients with this disorder have mutations in several genes which encode for Transforming Growth Factor-Beta Receptor. This genetic mutation causes patients to have low bone mineral density, usually resulting in osteoporotic-like fractures. Stress fractures are rarely reported in patients with LDS. We report a case of stress fracture in a patient with LDS, discuss the management of this patient and provide a brief overview of LDS.
Loeys-Dietz Syndrome (LDS) is an autosomal dominant genetic connective tissue disorder. It was first observed and described by Dr. Bart Loeys and Dr. Hal Dietz at the Johns Hopkins University School of Medicine in 2005 [1]. LDS consists of 5 types, and TGFBR1 and TGFBR2, SMAD3, TGFB2 and TGFB3 are the genes known to harbour mutations in individuals with LDS. Genetic testing for these mutations is available if there is a high index of suspicion of the diagnosis [2,3]. We present a care report which emphasizes on the fracture risk in Loeys-Dietz syndrome.
The patient in the presentation of this case report is a 12-year-old girl who was diagnosed with LDS type II (TGFBR2 mutation) at 5-years-old. This is complicated by a background of dilated aortic sinus s/p patent ductus arteriosus coil closure; on losartan 37.5 mg, C1-C2 cervical spine subluxation, and recurrent right patella dislocation, for which she underwent soft tissue patella tendon reconstruction.
This patient presented to the Emergency Department of a tertiary care paediatric hospital after being unable to stand after a fall. She experienced a sudden weakness in her left leg while trying to carry a backpack. Her left leg eventually gave way, resulting in her falling and landing on her buttocks. She had complained of pain and swelling in the left thigh from time to time prior to this incident but was still able to ambulate with no significant difficulties. There was no history of preceding trauma, high energy activity or high impact sports. On physical examination, she was found to have an isolated fracture of the left femur, but no other concomitant injuries. There were no open wounds, neurological or vascular impairment.
Initial radiographs (Figure 1) revealed a displaced fracture of the left femur shaft with a background of bone remodeling. This was likely due to an underlying stress fracture as seen from callous formed along the length of the mid-shaft of the femur. She underwent surgical fixation of the fracture: closed reduction using a traction table and internal fixation via insertion of titanium elastic nailing system (TENS) was done under image-intensifier guidance (Figure 2). She recovered uneventfully post-operatively. The patient underwent rehabilitation with partial weight bearing and subsequently moved on to full weight bearing. The TENS implants were removed after 8 months. At 12-month follow-up, the patient remained well and had no complains of limb pain or new fractures.
 Figure 1: Displaced fracture of the left femur shaft with a background of bone remodeling.
View Figure 1
Figure 1: Displaced fracture of the left femur shaft with a background of bone remodeling.
View Figure 1
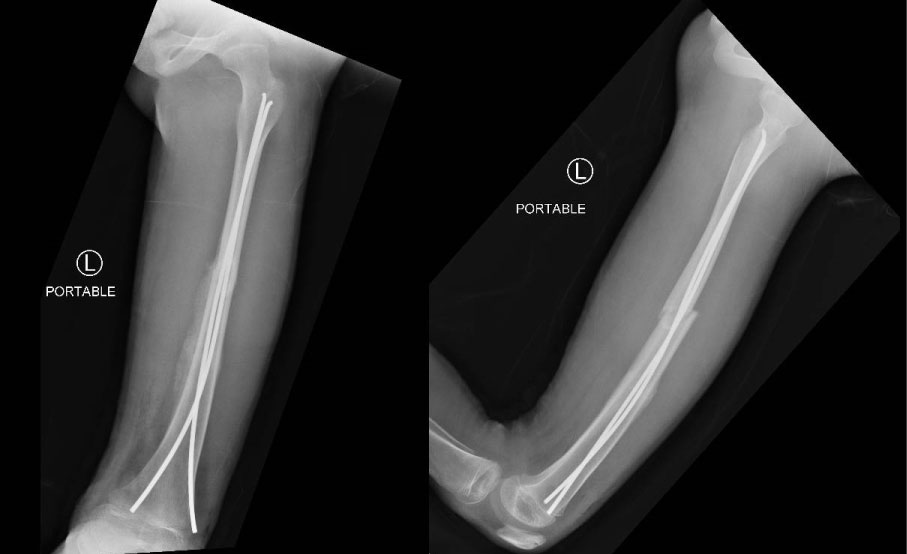 Figure 2: Surgical fixation of the fracture.
View Figure 2
Figure 2: Surgical fixation of the fracture.
View Figure 2
The incidence of LDS is very low in the Asian population [4]. Most reports of LDS were from the European and American population. Previous studies were done in Korea [4] which identified 13 patients from a period of June 2000 to December 2010, and in Hunan province of China [5]. Locally, Ting, et al. [6] reported that from 2007 to 2013, five patients with LDS have been diagnosed and managed in KK Women's and Children's Hospital.
It is well described that patients with LDS present with osteoporosis and multiple fractures at a young age. The incidence of fractures reported in the general population is 2.3-2.42 fractures per 100 person-years [2]. Compared with the general population, the incidence of fractures in patients with LDS was significantly greater at 3.86 fractures per 100 person-years. There was a 50% risk of fractures by the age of 14 years. Fractures were most common in the upper extremity [7], amounting to 60.8%, with a comparatively higher prevalence of forearm and wrist fractures. A study also noted low bone mineral density and a history of fractures in two patients with LDS and TGFBR2 mutations [2]. It can be postulated that low bone mineral density increases the risk of fractures in patients with LDS. The most commonly described fracture pathology and the fracture pattern is osteoporosis-related low energy fragility fractures. This differs from our patient, who had a stress fracture with no significant repetitive trauma to the bone.
Considering the biochemical predictors for low bone mineral density, we note that there are large amounts of TGF-b in bone and cartilage that modulate the activity of osteoblasts and osteoclasts [1,4]. TGF-b1 has a role in coupling bone resorption and formation [8]. It has been observed that bone turnover is elevated, and bone mass is low in LDS patients, suggesting increased TGF-beta signaling; this same observation was seen in mice carrying a similar mutation [9]. Thus, the bone turnover and bone mass results are compatible with the hypothesis that the TGFBR2 mutations in these patients were associated with increased TGF-beta signaling. This suggests that weak bone mass in combination with increased physical activity is a recipe for stress fractures. Given the patients skeletal immaturity, and the potential of the periosteum to heal, her stress fracture did not surface till a later age [10].
With earlier detection and improvement in treatment of vascular complications of LDS, it is expected that life expectancy of patients with LDS would increase as well. Life expectancy in LDS patients was once estimated to be 26 years of age. Nowadays, most patients can lead a long, full life, comparable to that of non-LDS individuals. Hence, apart from instituting appropriate vascular imaging surveillance, this case also highlights the importance of paying close attention to fractures and bone density in patients with LDS. Osteopenia or osteoporosis may become increasingly important issues as the patient ages, which can result in low-impact fractures as seen in this patient [11].
It is important that physicians include screening of stress fractures in their routine history and examination and counsel their patients about their predisposition to low bone mineral density and higher fracture risk. First-line measures to optimize bone health in children fall into three main categories: Nutrition, physical activity, and treatment of the underlying condition and associated comorbidities. In terms of nutrition, vitamin D and calcium are some of the most well-described nutritional factors for bone health [10]. Calcium is a key nutrient for adequate skeletal mineralization with recommended intakes best achieved through a healthy diet. Even though high impact activity has been shown to have an anabolic effect on the growing skeleton and to increase bone mass in children, patients with high risk for fragility fractures will still have to make some lifestyle modifications. This should be a multi-disciplinary effort, in consultation with the physiotherapist and occupational therapist.
To treat osteoporosis in children, bisphosphonates are known to be the most extensively published agents. Bisphosphonate therapy is typically reserved for children with a history of low-trauma fractures, with a limited potential for spontaneous recovery due to permanent or persistent osteoporosis risk factors. Low-energy long bone fractures, such as in this patient, and symptomatic vertebral fractures are the most frequent indications for treatment.
Currently, it is unclear whether there is any effective treatment that will alter the course of osteoporosis in the subset of patients with LDS who develop skeletal fragility. Since there is insufficient data to recommend drug therapy for the primary prevention of osteoporotic fractures in children at present, careful monitoring of at-risk children is indicated. This is important in identifying early signs of bone fragility, particularly in those with limited potential for spontaneous recovery.
The successful treatment of our patient supports the use of TENS nailing in children with stress fractures associated with low bone mass. The role of prophylactic surgical management and the exact surgical principles should be further assessed with long term follow up and vigilant monitoring.
LDS is a connective tissue disorder that presents with increased risk of stress fractures as well as skeletal fragility fractures. We emphasize the importance of treating osteoporosis and osteopenia in these patients. The key facets of treatment are nutrition, activity modification and management of low bone mass. Stress fractures on a background of osteoporosis in skeletally immature patients, can be treated effectively with TENS nailing.