Several studies have linked elevated cardiac troponin to increased overall risk in patients with acute coronary syndrome but the prognostic significance of elevated troponin in non-cardiac conditions remains scanty.
The primary aim of this study was to investigate the prognostic significance of elevated high sensitivity troponin T (TnT-HS) in non-cardiac disorders outside the remit of an acute coronary syndrome (ACS). Secondarily we aimed to investigate the impact of cardiovascular comorbidities and other clinical presentations in the release of cardiac biomarkers in non-cardiac disorders.
This was a retrospective electronic patient record pilot review where all patients with elevated TnT-HS without acute coronary syndrome, recent angioplasty or heart failure within a three month period were enrolled into the study and subsequently followed prospectively for a six month period. From January 1, 2016 to June 30, 2016, a total of 2535 patients were screened of which 306 patients had elevated TnT-HS and 162 patients met the study inclusion criteria.
Data were encrypted and collected in Google database format, exported into excel spreadsheet, analyzed and computed using SPSS (version 24) to identify clinical associations with increased values of TnT-HS.
Most troponin TnT-HS samples (77.1%) were obtained from emergency room (ER) attendance and 63.4% of patients were male. The mean age was 72 years and no correlation were found between age and troponin levels (rs = -0.18, p = 0.816) by Spearman Rank-order correlation. Although expectedly patients with diagnosis of acute coronary syndrome displayed TnT-HS values significantly higher than those of other groups, positivity to TnT-HS (> 40 ng/l) was also observed in patients with other clinical conditions. In multivariate analysis, baseline chronic kidney disease (CKD), acute infectious diseases mainly urinary tract infection and cerebrovascular events (CVA) were independently associated with TnT-HS positivity at admission. Observations from the cohort as a whole; TnT-HS positivity exhibited high sensitivity and negative predictive value, counterbalanced by low specificity and limited positive predictive value. Major adverse cardiac and cerebral events (MACCE) were significant within 6 months including; Death (13.7%), MI (3.9%), Stroke (ischemic 4.6%, hemorrhagic 2.3%, TIA 0.8%) - p value < 0.02.
TnT-HS positivity should be cautiously interpreted in patients exhibiting non acute cardiac conditions associated CKD, infections, and CVAs. This troponin elevation in non-cardiac conditions still carries a significant adverse prognosis.
After adjusting for age and renal insufficiency, we can suggest a new cut off level of TnT-HS > 30 ng/l to have increased risk of MACCE within 180 days in non-cardiac conditions.
Troponin T high sensitivity, Non-cardiac disease, Significance, Outcomes
Troponins are proteins that facilitate contraction of cardiac muscle by binding with actin and tropomyosin. Each troponin (Tn) complex is composed of three subunits - TnC, TnT and TnI. TnC binds calcium and regulates activation during contraction. TnT binds the complex to tropomyosin while TnI inhibits binding in the absence of activation [1-5].
Troponins are expressed in cardiac and skeletal muscles (fast and slow). TnC is found as a single isoform in all three sources. TnT and TnI on the other hand, exist as different isoforms in each type of muscle cell. This has led to the development of specific assays for the cardiac isoforms of Troponin T, I, and Troponin T high sensitivity (CTnT, CTnI, and TnT-HS) to indicate myocardial injury [2-5].
Cardiac troponin I CTnI is only produced in myocytes, while CTnT is found in small amounts in skeletal muscles. The, most specific assays for myocardial injury measure for CTnI [5,6].
Cardiac troponins were introduced in the year 2000 by the American and European guidelines to diagnose acute coronary syndromes caused by thromboembolic disease [6]. Their use has expanded to indicate myocardial injury caused by obstructive and nonobstructive coronary artery disease and they were found to carry prognostic significance [6-19].
Elevation of cardiac troponins has been noted to occur in heart failure, renal failure, pulmonary embolism, respiratory failure, stroke, anemia, and other medical disorders.
The pathophysiology is thought to be related to myocardial injury caused by noxious stimuli, stretch and hypoxia [7-28].
This has led to the classification of type 1 versus type 2 myocardial infarction (MI) [29,30]. Type 1 myocardial infarction denotes myocardial injury caused by hypoperfusion to myocytes because of atherosclerotic/thromboembolic disease. It includes the spectrum of acute coronary syndromes: Unstable angina and myocardial infarction with or without ST changes. Patients present with characteristic chest pain and elevated cardiac troponins and will require urgent reperfusion therapy to salvage the myocardium (2013 ACCF/AHA guidelines for STEMI and the 2014 AHA/ACC guidelines for NSTEMI).
Type 2 myocardial infarction is thought to be caused by supply-demand mismatch to the myocytes because of systemic hypoperfusion or noxious stimuli. Therapy is directed at treating the underlying cause. It has been reported that patients with type 2 MI and elevated cTnI had increased risk of death within 6 months compared to those without MI [29-30].
In this study, our primary aim was to investigate further the prognostic significance of elevated TnT-HS in non-cardiac disorders. The secondary aim of this study was to investigate the effect of cardiovascular comorbidities in raising cardiac biomarkers in non-cardiac disorders.
This is a retrospective electronic pilot cohort review over 6 months conducted in International Medical Center (IMC)- Jeddah from January 2016 to June 2016.
1. To evaluate the prognostic significance of elevated TnT-HS in different non-cardiac medical disorders indicated by the development of MACCE including myocardial infarction (MI), transient ischemic attack, stroke, or death.
2. To study cardiovascular co-morbidities effect on elevation of TnT-HS in different non-cardiac medical disorders.
A MACCE was defined as the development of MI, Stroke/TIA or death within the six month follow-up period. The 2013 ACCF/AHA guidelines for STEMI and the 2014 AHA/ACC guidelines for NSTEMI are used to define MI. Stroke and TIA are defined by the American Heart Association (AHA) guidelines published in 2013.
A master database was produced containing patients with different medical disorders who had elevated TnT-HS.
2535 patients who presented to IMC were investigated for elevated TnT-HS in the period between January 1st to June 30th 2016 were pooled into a common database. From these patients, 162 patients met the study inclusion criteria and 31 were lost to follow-up.
1. Elevation of cardiac troponin (CTn) above 0.050 ug/L TnT-HS > 30 ng/l
2. Patients admitted with non-cardiac medical diagnoses.
1. Acute coronary syndrome or MI during the index admission.
2. Coronary intervention within the past one month.
3. Patients with a myocardial infarction within the past one month.
A web-based questionnaire was developed and a team of data collectors gathered the following data:
1. Demographic data (age, gender, weight, height, BMI)
2. Location where sample was collected
3. CK, CKMB, CTn, TnT-HS Levels, LDH (in case of serial tests, the highest value will be considered as the index value).
4. D Dimmer, BNP
5. Complete blood counts
6. Creatinine, Glomerular Filtration Rate, Blood Urea Nitrogen, Sodium, Potassium
7. ALT
8. Calcium, Magnesium, Albumin
9. TSH, HBA1c
10. CRP
11. Echocardiographic Findings (baseline at the initial episode and over the six-month follow-up period).
12. ECG findings
13. Final Diagnosis
14. Presence of CVS co-morbidities (Diabetes, Hypertension, Dyslipidemia, Smoking, Obesity).
15. Diagnosis of MACCE after the sample was drawn over the six-month follow-up period.
Estimation of serum Troponin T (TnT) was done using highly sensitive electrochemiluminescence immunoassay based on sandwhich assay principle. The measuring range of assay is 3-10000 ng/L. The patient testing was performed after calibration and control were satisfied as per manufacturer standard recommendations for TnT.
All data were collected using a web-based questionnaire, exported into an Excel® spreadsheet and computed using SPSS version 24. Qualitative Data:
1. Frequencies and percentages are used to find out the incidence of elevated CB-TnT-HS in different non-cardiac medical disorders.
2. Chi Square was used to assess significance of categorical variables, p value < 0.05 was considered significant.
3. All decimal places were rounded to 2 significant figures.
1. Means and standard deviations of elevated CB in different non-cardiac medical themes were produced.
2. We tested the variable troponin by using Shapiro-Wilk test for normal distribution. We used two non-parametric tests: Kruskal-Wallis and Man-Whitney test to compare mean troponins between different themes and between patients who developed and did not develop major CVS events respectively.
3. We examined a new cut-off value (threshold) of biomarker elevation that may be a surrogate level by constructing area-under the curve graphs to facilitate prognostic significance in non-cardiac medical disorders.
4. Chi square and multi-nominal logistic regressions were used to study CVS co-morbidities effect on elevation of CB TnT-HS in different non-cardiac medical disorders.
Approval for the study was obtained from the hospital Research and Ethics Committee. Consent for the study was deemed unnecessary because it was a retrospective electronic records review with no patient identification or interaction. A customized encrypted coding scheme was incorporated to ensure patient confidentiality.
In the interval between January to July 2016, 162 patients met the inclusion criteria of the study, from this group 31 were lost to follow-up. Most troponin TnT-HS samples (77.1%) were obtained from the ER and 63.4% of patients were male (p value > 0.05) (Table 1).
Table 1: Presenting the location where Troponin samples were obtained and Gender. View Table 1
The mean age of the sample was 72 years. No correlation was found between age and troponin levels by Pearson.
Medical disorders were grouped into 5 different themes; infectious, renal, neurological (CNS), respiratory and others. The most prevalent theme was infectious (39.7%) and the most prevalent diagnosis was urinary tract infection (Table 2). Patients with gastroenterology, rheumatology, haematology and where no specific diagnosis was reached were classified as -Other given their small proportion of the sample. The third most prevalent theme was renal, followed by CNS and respiratory (Figure 1). There was no significant difference in echo and ECG findings between different themes by chi square (p value > 0.05) (Table 3).
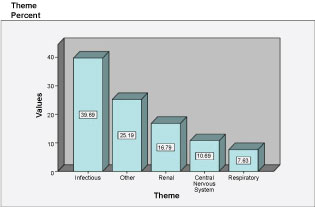 Figure 1: Summarizing the prevalence of different themes.
View Figure 1
Figure 1: Summarizing the prevalence of different themes.
View Figure 1
Table 2: Summarizing the different themes and diagnoses. Themes were compared using chi-square, significance was chosen at 0.05. View Table 2
Table 3: Summarizing the difference between themes using chi-square. P value < 0.05 was considered significant. View Table 3
Of the patients who actually developed a major CVS event, 30.3% initially had an infectious etiology and 27% a CNS etiology (Figure 2). We used chi-square to compare the risk of developing a major CVS event between different themes. The only theme that was significant was the neurological (p < 0.05) (Table 4).
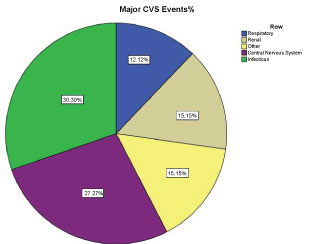 Figure 2: Summarizing the percentages of different themes in patients who developed Major CVS events.
View Figure 2
Figure 2: Summarizing the percentages of different themes in patients who developed Major CVS events.
View Figure 2
Table 4: Comparing different themes with developing Major CVS event. Chi-square was used, p value < 0.05 was considered significant. View Table 4
The most common symptom observed in patients who developed major CVS events was shortness of breath and neurological symptoms such as decrease level of consciousness (LOC) (30.30% each) followed by infectious symptoms such as fever (27%) and cough (21%). Chest pain was the least observed symptom (6%) (Figure 3 and Table 5). There was no significant difference between symptoms and developing major CVS events (p > 0.05).
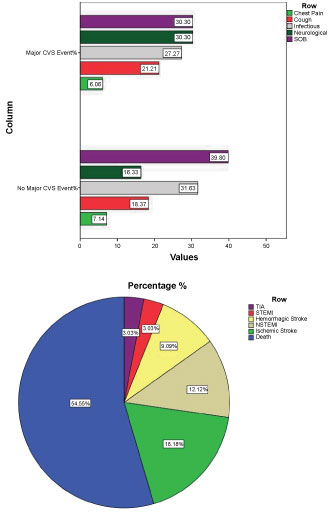 Figure 3: a) Summarizing the initial chief complaints in patients who developed and did not develop Major CVS events; b) Summarizes the different types of Major CVS events.
View Figure 3
Figure 3: a) Summarizing the initial chief complaints in patients who developed and did not develop Major CVS events; b) Summarizes the different types of Major CVS events.
View Figure 3
Table 5: Summarizing the initial chief complaints in patients who developed and did not develop Major CVS events. View Table 5
Table 6 illustrates the different major CVS event and their time-course. Most major CVS events were deaths (13.7%) followed by Ischemic stroke (4.6%) (Figure 3).
Table 6: Summarizing the different Major CVS events and their time course. View Table 6
The mean troponin of the data sample was 0.27 (27 ng/l) ± (SD) 0.54 (54 ng/l). We tested the variable troponin by using Shapiro-Wilk test and found that it was not normally distributed (p value < 0.05). We used two non-parametric tests: Kruskal-Wallis and Man-Whitney Test to compare mean troponins between different themes and between patients who developed and did not develop major CVS events respectively. The highest means of troponin were observed in patients with CNS diagnoses 0.45 (45 ng/l) ± SD 1.02 (102 ng/l) followed by Respiratory (0.42 (42 ng/l) ± SD 0.97 (97 ng/l), however the difference between themes was not significant (p > 0.05) (Figure 4). Patients who developed CVS events had a higher troponin mean 0.30 (30 ng/l) ± SD 0.55 (55 ng/l) compared to patients who did not (0.26 (26 ng/l) ± SD 0.54 (54 ng/l), however the difference was not statistically significant as assessed (p > 0.05) (Figure 5).
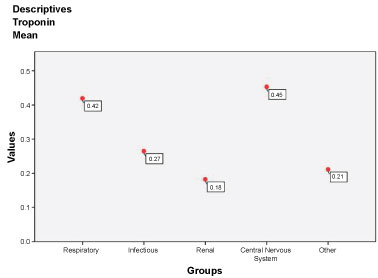 Figure 4: Comparing means of troponins encountered in different themes.
View Figure 4
Figure 4: Comparing means of troponins encountered in different themes.
View Figure 4
 Figure 5: Comparing means of troponins between patients who developed and did not develop major CVS events.
View Figure 5
Figure 5: Comparing means of troponins between patients who developed and did not develop major CVS events.
View Figure 5
The most prevalent comorbidities observed in the data sample are presented in Figure 6. In the Major CVS patient group, hypertension (HTN) was most prevalent followed by diabetes (DM) and chronic kidney disease (CKD). We used chi-square to compare the difference in comorbidities between the group of patients who developed Major CVS events and those who did not; only CKD was observed to be significantly different (p value < 0.05). However, when we performed nominal logistic regression on the data sample, the difference between comorbidities in both groups including CKD was not significant (p > 0.05) (Table 7).
 Figure 6: Illustrating the comorbidities in the studied population.
View Figure 6
Figure 6: Illustrating the comorbidities in the studied population.
View Figure 6
Table 7: Summarizing the different lab results in the studied population. View Table 7
Elevated cardiac troponins occur at times of myocardial injury [6-28]. The etiology was initially thought to be due to ischemia secondary to the ACS paradigm involving obstruction of the coronary arteries [9-31]. Cardiac troponin elevation can occur in other diseases and does not necessarily indicate the presence of a thrombotic acute coronary syndrome as recent research has shed light on many other medical causes of troponin rise besides the ACS [29-41]. Troponin elevation was also reported in healthy young adults and children [33].
Among the 131 patients included in this study, the most common etiology associated with elevated Cardiac troponin was the infectious group, with UTI being the most common diagnosis. Sepsis is the leading cause of death in the non-cardiologic ICU. Poorly distributed nutritive blood flow and altered convective and diffusive oxygen transport during sepsis can lead to organ dysfunction and multiple organ failure. One of the causes of myocardial dysfunction is thought to be myocardial ischemia in sepsis; however, conventional biochemical parameters to detect myocardial ischemia lack sensitivity and specificity. Serum cardiac troponin T (S-TnT) was reported to have higher sensitivity and specificity in diagnosing minor myocardial injury [36-43].
This may be due to increased myocardial demand due to hypoxia, fever and hypotension which accompany sepsis conditions [42]. Spies and colleagues studied the elevation of cardiac troponins on 26 ICU patients with underlying sepsis and concluded 23 that elevated troponins carried a prognostic significance and were associated with higher mortality [43].
The second common medical etiology in our study was due to renal disease including end-stage renal disease on hemodialysis and acute on chronic kidney disease. Cardiovascular disease is a major cause of morbidity and mortality among patients with chronic kidney disease and those on hemodialysis accounting for approximately 50% of deaths [42-44]. Measuring troponins among this group of patients is often misleading as they tend to have higher troponin levels than other sub-groups due to reduced renal clearance [45]. In patients with renal disease, elevated troponins have a low sensitivity to diagnose acute coronary syndrome (high false positive), and thus should be used with caution when assessing prognosis [46].
Respiratory disorders causing elevated troponins included respiratory failure, obstructive airway disease and pulmonary embolism. The hypoxia associated with respiratory disorders causes� myocardial injury leading to type 2 MI [29,30]. In recent studies, elevation of troponin I in patients with chronic obstructive pulmonary disease was an independent predictor of the need for non-invasive mechanical ventilation [47-49]. In patients with pulmonary embolism, elevated troponins indicate a sub-massive or massive clot and are used as a risk determinant thrombolysis or embolectomy [50-56]. In one study [51] cardiac troponin levels were increased in 24 of 147 patients (16%) with documented acute pulmonary embolism and in 20 of 594 patients (3%) without pulmonary embolism (p < 0.001). In the same study patients with acute pulmonary embolisms, 8 of 24 (33%) with increased cardiac troponin I levels and 9 of 123 (7%) with normal cardiac troponin I levels died during hospitalization (p < 0.001).
Neurological diseases were important causes of troponin elevation in our study, and the only theme in which elevation of TNT-HS was associated with development of a major CVS event (p < 0.05). Studies have shown that aneurismal subarachnoid hemorrhage survivors and in whom the aneurysm has been occluded, had an overall increased long-term mortality rate and an increased incidence of cardiovascular events compared with age-and sex matched groups [56-61].
There is evidence that troponin may be released from the injured myocardium in response to noxious agents and hypoxia incited by different medical disorders and may reflect overall severity of illness, once coronary artery disease has been excluded [54-64]. In our study, 33 patients developed major cardiovascular events, 18 deaths, 5 ischemic strokes, 4 NSTEMI, 1 TIA, 3 hemorrhagic strokes, 1 STEMI. This MACCE denotes that elevated troponin in non-cardiac conditions confers a significant implication at 6 months clinical outcomes and is not to be ignored. Our findings are in agreement with the result of a recent cross-sectional study of high-sensitivity cardiac troponins T which concluded that Significant illnesses apart from the acute coronary syndrome are important causes of a rise in cTn to above the 99th percentile, and appear to reflect the total body burden of disease. Even when the high hs-cTn concentration is not due to the acute coronary syndrome, there is a significant association with all-cause mortality [57].
After adjusting for age and renal insufficiency, we can suggest a new cut off level of TnT-HS > 30 ng/l to have increased risk of MACCE within 180 days in non-cardiac conditions (Figure 5). So, in brief, cardiac troponins are released into the circulation when cardiac myocytes are damaged by acute ischemia or any other mechanism. Cardiac troponins are important for the diagnosis, risk assessment, prognosis, and determination of antithrombotic and revascularization strategies. However, troponin elevation indicates the presence, not the mechanism, of myocardial injury.
The major limitation of our study was its retrospective nature, meaning that some data could have been missed due to missing documentation. Additionally, our small cohort size, which may not be representative of the whole population and relatively short follow-up duration. Some subjects with raised troponin, we suspect had at least some form of stable pre-existing asymptomatic background coronary artery disease.
Our data suggest that in a mixed population, many persons will have increased troponin concentrations, without overt cardiac disease being present or manifest. While troponin is cardiac-specific, it is not ACS-specific, and any significant illness may cause a rise in troponin due to severe stress caused by the acute non-cardiac clinical event may result in a minor leakage of myocardial markers. This troponin elevation in non-cardiac conditions still carries a significant outcome on prognosis. Elevated cardiac troponin levels can be present among several non-cardiac situations including; infection, sepsis, kidney, pulmonary, neurological, and critically ill patients without evidence of myocardial ischemia. The stroke and mortality rates of troponin-positive patients are significantly higher compared with troponin-negative patients. Even minor elevations are specific for myocardial injury. We can suggest a new cut off level of TnT-HS > 30 ng/l to have increased risk of MACCE within 180 days in non-cardiac conditions. However, every elevated troponin level in the non-cardiac patient should not be rigorously scrutinized or treated as a myocardial infarction.
We recommend further prospective, preferably multicenter large population studies to clarify the implications various medical disorders have on cardiac biomarkers, cardiovascular events and mortality.
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.