Acute Myocardial Infarction (AMI) during the early postpartum period is a rare event and carries a high mortality rate. We report an unusual case of Type A aortic dissection involving the left coronary ostium and presenting as anterolateral ST segment elevation myocardial infarction. Our patient was diagnosed to have aortic dissection at the time of left heart catheterization, and suffered a cardiac arrest prior to undergoing surgical intervention.
A 39-year-old Caucasian woman presented to the outside hospital with complaints of one hour of excruciating retrosternal chest pain, dyspnea and diaphoresis. Ten days prior to the presentation, patient underwent an uncomplicated vaginal delivery. Her pregnancy was complicated by moderate gestational hypertension. Electrocardiography (ECG) showed ST segment elevations in leads aVL, aVR, V2 and V6 with reciprocal changes in II, III and aVF (Figure 1).
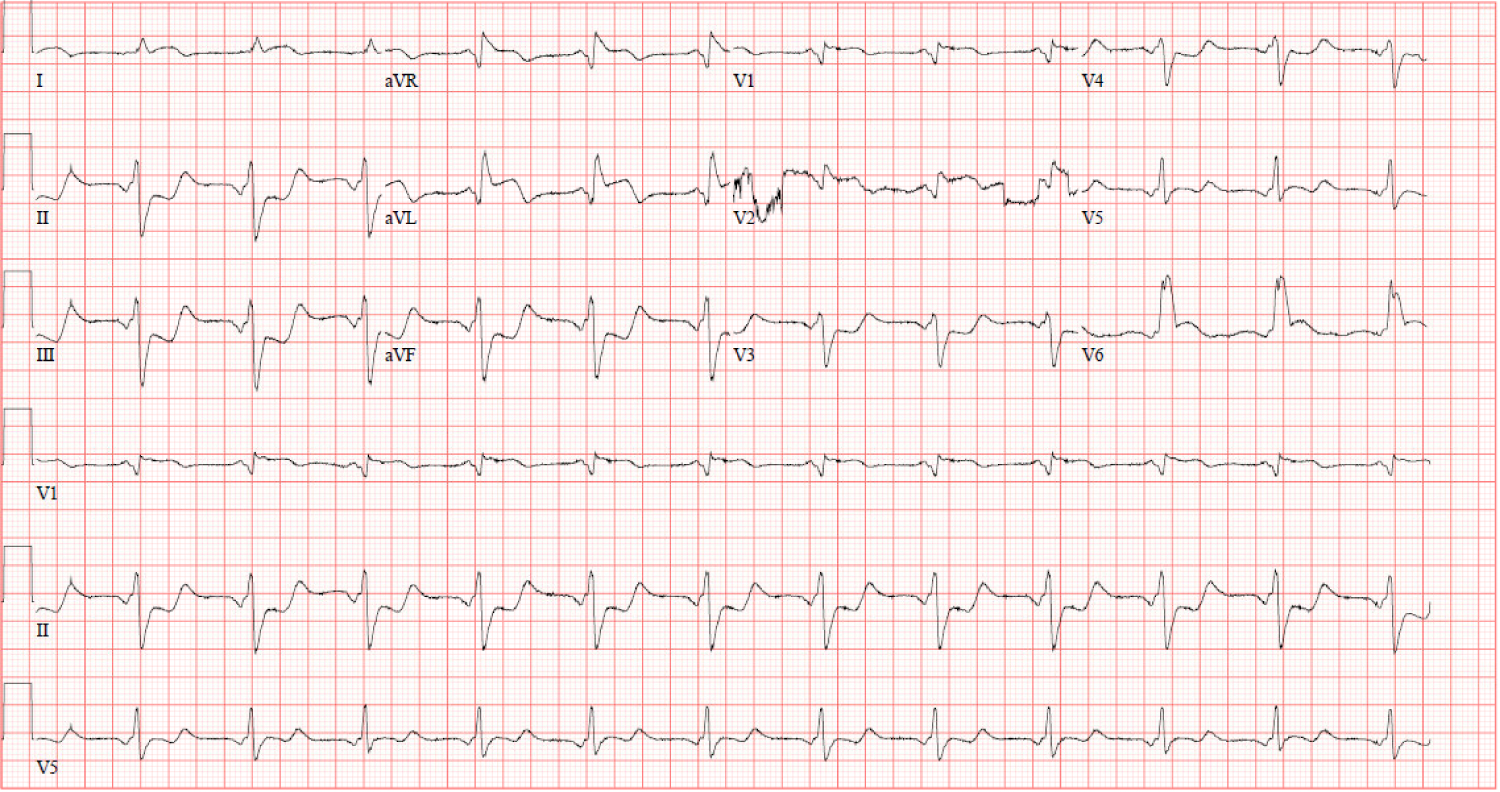 Figure 1: Presenting 12-lead EKG revealing ST elevations in leads aVL, aVR, V2 and V6 with ST depressions in II, III and aVF.
View Figure 1
Figure 1: Presenting 12-lead EKG revealing ST elevations in leads aVL, aVR, V2 and V6 with ST depressions in II, III and aVF.
View Figure 1
Laboratory data was significant for troponin 0.158 ng/mL, Brain natriuretic peptide (BNP) 70 pg/mL and D-Dimer 2.08 mg/L. She received aspirin, clopidogrel and heparin prior to transfer to our facility for left heart catheterization.
When she arrived at our ER, she continued to report chest pain and dyspnea. She was hemodynamically unstable with blood pressure 53/23 mmHg, heart rate 74 beats/minute, respiratory rate 20/minute and an oxygen saturation of 95% on 100% oxygen via non-rebreather mask. She was immediately placed on dopamine drip and moved to the catheterization lab. In the lab she was found to be increasingly hypoxemic and had an episode of vomiting, requiring intubation. Transthoracic echocardiogram showed mild - moderate left ventricular dysfunction with no pericardial effusion. The right femoral artery and vein were accessed percutaneously. A 6 - French JR4 catheter over a J wire was advanced into the ascending aorta, however due to difficulty encountered in passing the catheter through aortic valve, there was a suspicion for aortic dissection and injection through Judkins catheter confirmed the presumed diagnosis (Figure 2).
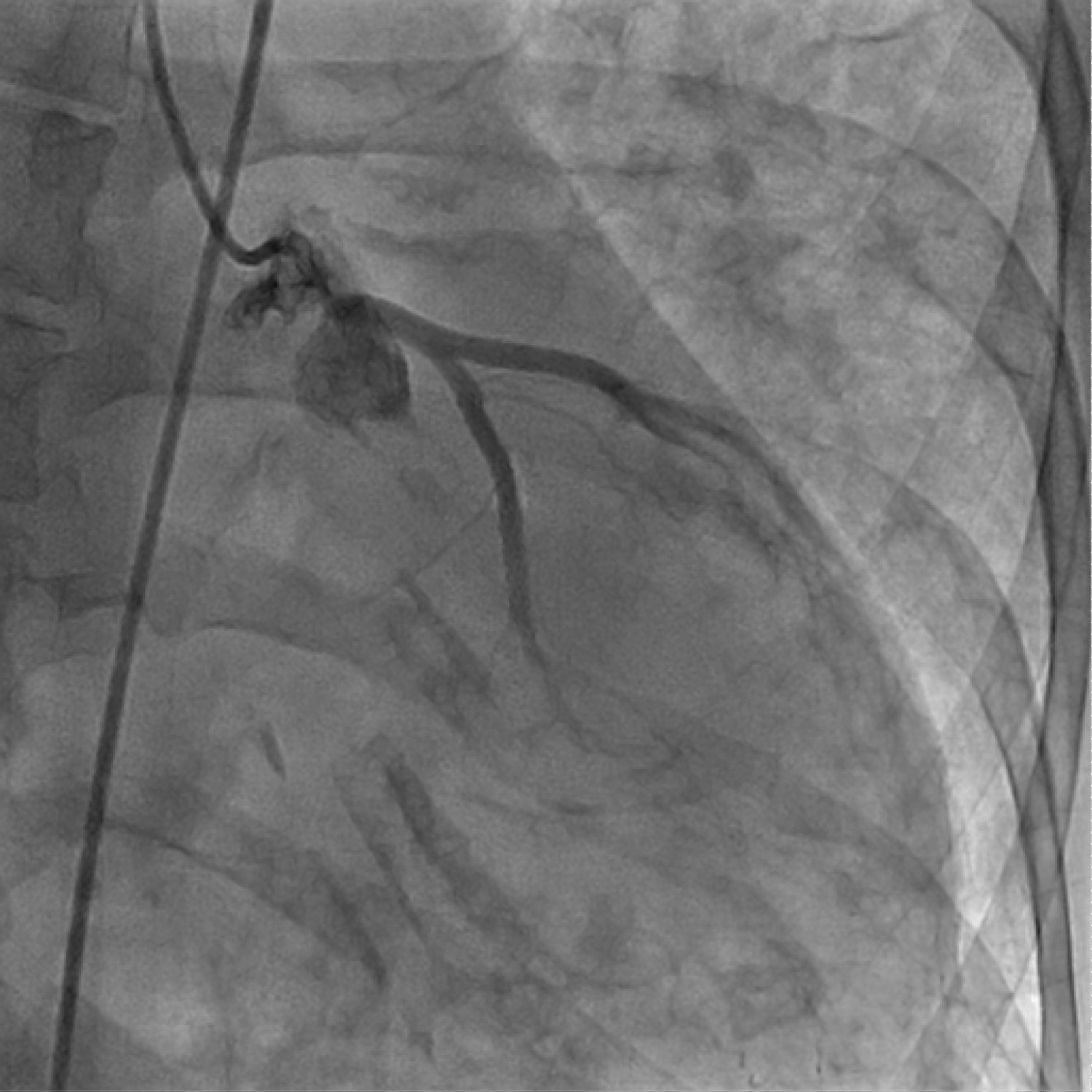 Figure 2: Coronary angiography depicting false and true lumen.
View Figure 2
Figure 2: Coronary angiography depicting false and true lumen.
View Figure 2
Thoracic aortogram with a pig tail catheter outlined the presence of flap (Figure 3). There was also compression and narrowing of left main artery, with 90% occlusion and sluggish flow through the left sided circulation.
 Figure 3: Thoracic aortogram outlining the dissection flap.
View Figure 3
Figure 3: Thoracic aortogram outlining the dissection flap.
View Figure 3
Due to hypotension, severe left main stenosis and very poor blood flow in the left sided circulation, stenting was performed with the help of a 4 x 12 mm bare metal stent alleviating the high grade stenosis (Figure 4).
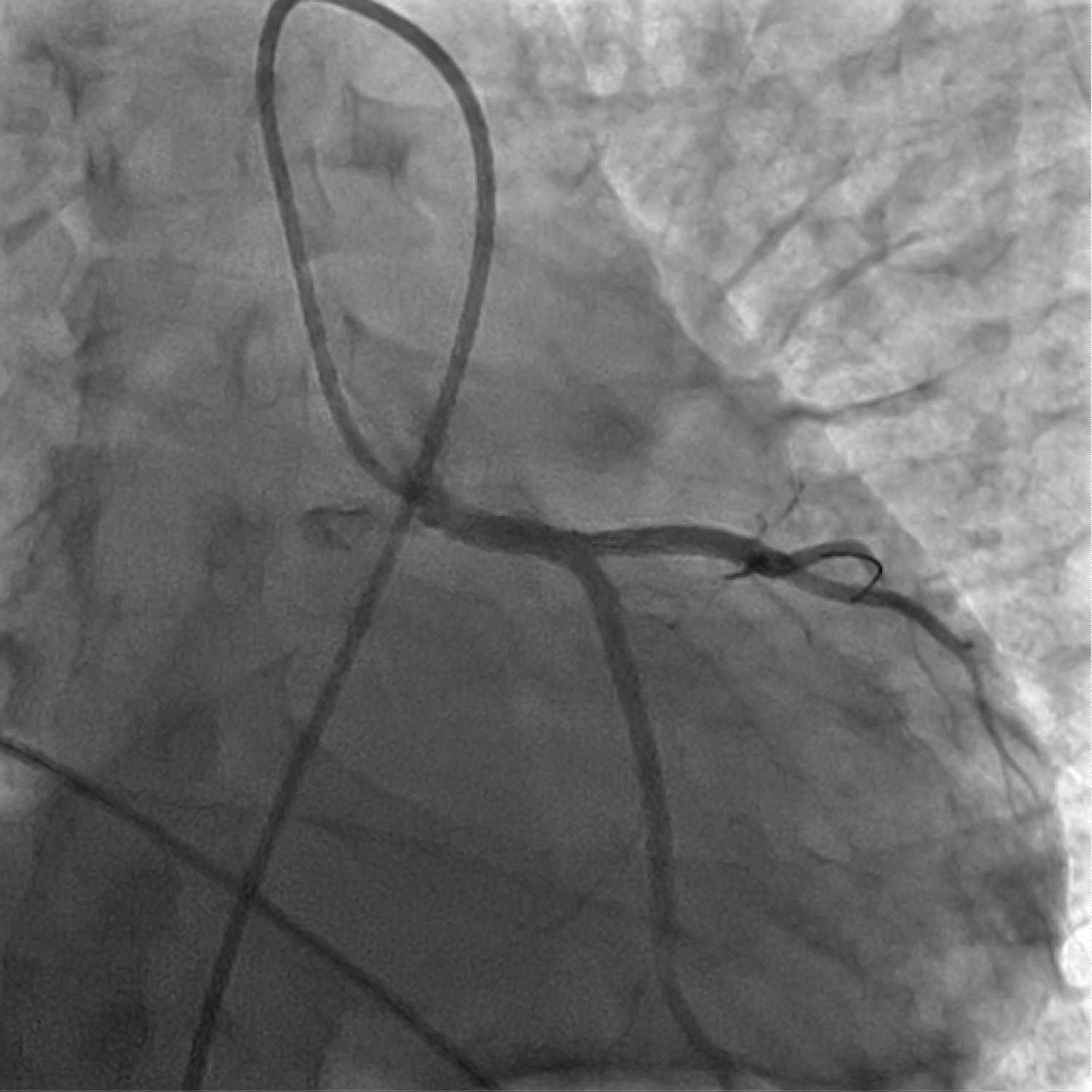 Figure 4: Angiography after stent implantation in left main coronary artery.
View Figure 4
Figure 4: Angiography after stent implantation in left main coronary artery.
View Figure 4
Her blood pressure stabilized following the procedure, however she was found to be in persistent wide complex tachycardia with a heart rate in 140-150's bpm. Her rate and rhythm remained unchanged despite amiodarone and synchronized cardioversion. Surgical intervention for aortic repair was attempted. She was then immediately moved into a helicopter for transferring her to a higher level facility for aortic repair. Unfortunately, she went into cardiac arrest with pulseless electrical activity and passed away.
Aortic dissection can occur in pregnancy or during the postpartum period without any pre-existing disease due to hormonal changes. The incidence of non-syndromic aortic dissection in this group of population is 14/1,000,000, with a fatality ratio of 4.4/1,000,000 [1]. The third trimester of pregnancy or immediate postpartum period is the most common interval of occurrence. The differential diagnoses of severe chest pain in postpartum period include acute myocardial infarction, pulmonary embolism, and aortic dissection. Complications of aortic dissection are aortic rupture, aortic regurgitation, acute myocardial infarction, tamponade and end-organ ischemia. When there is an involvement of coronaries, aortic dissection often involves right coronary artery (RCA) and present as inferior wall STEMI [2,3]. The frequent occurrence of dissection from the right anterior aspect of ascending aorta above the right sinus of Valsalva, explains the high incidence of RCA involvement [4]. Involvement of the left main coronary ostium is rare [5,6] and occurred in our patient.
The Stanford classification divides aortic dissection into type A and type B [7]. Type A dissection (TAAD) involves the ascending aorta, and eventually progressing to the distal aorta. Type B dissection originates at the level of descending aorta.
Neri, et al. classified the coronary ostial involvement by dissection as follows [8]:
Type A: Ostial dissection, with a disruption of the inner layer limited to the area of the coronary ostium. About 20% of patients with type A dissection have ECG evidence of acute ischemia or Myocardial infarction. Among these patients, 1-2% have involvement of coronary artery ostium secondary to proximal dissection flap.
Type B: Retrograde extension of the aortic dissection from the ostium into the coronary arterial wall creating false lumen.
Type C lesion: Complete detachment of aortic root from affected ostium of coronary artery, with intussusception of inner cylinder into the involved coronary artery.
Acute chest pain, mediastinal widening and/or aortic widening, pulse and/or blood pressure differentials can be used to predict aortic dissection [9]. Upper extremity pulse discrepancies may occur in 30% of aortic dissection, and comparatively lesser in distal disease [10]. On the other hand, CXR may be abnormal in 80% of the patients, with an abnormal aortic contour in 45% of patients and mediastinal widening in 60% of cases. These three variables could identify 96% of acute aortic dissection cases [9]. In other instances, modalities including D-Dimer and computed tomography (CT) could be important to establish the diagnosis. D-Dimer may be a useful tool in differentiating aortic dissection from myocardial infarction within the first 6 hours with a sensitivity of 96.6% at cutoff value of 500 ng/ml [11]. A 2-dimensional Trans thoracic echocardiography (TTE) is also helpful as an initial screening test, specifically in patients with type A dissection with a sensitivity ranging from 78%-100% in those cases [12]. A TTE was performed in our patient who only showed left ventricular dysfunction with no other abnormalities. The sensitivity of transesophageal echocardiogram, Computed Tomography and Magnetic resonance imaging exceed 90% in the diagnosis of aortic dissection [10]. However, imaging studies for STEMI patients may not be done initially due to a possibility of increasing the "door to balloon" time in the emergency setting. Due to hemodynamic instability and concerning EKG changes, our patient was immediately taken to the catheterization lab in order to save the "door to balloon time" as mentioned above. During a cardiac catheterization procedure, an intravascular ultrasound (IVUS) examination could reveal the presence of TAAD in STEMI patients [9]. Surgery is the definitive treatment, however successful stabilization of the left main artery lesion while awaiting surgery has been reported [5]. In case of our patient, we performed stenting as a bridge to definitive surgery due to hemodynamic instability and severe stenosis of left sided coronary circulation, while the patient was being transferred to a higher level facility for aortic repair.
• Recognize aortic dissection as one of the causes of severe chest pain in pregnancy and postpartum.
• Although rare, consider aortic dissection as a potential cause of ST segment elevation myocardial infarction in pregnancy and postpartum.
• Early diagnosis and surgical management are keys to survival.
None.
None.