Kounis Syndrome is an anaphylactic acute coronary syndrome which may be caused by several causative agents including food, drugs, environmental and other causes [1]. The various triggers result in mast cell activation with subsequent release of inflammatory mediators such as histamine and cytokines which then interact with T cells and macrophages in cardiac tissues. This results in coronary vasospasm and/or coronary plaque erosion or rupture [2]. The presentation is similar to that of an acute coronary event with chest pain and corresponding changes in EKG and troponin [3]. This was first reported in 1950 with a coronary event being attributed to an allergic reaction to Penicillin [4]. In 1991, Kounis described this relationship in more detail as “allergic angina” and this syndrome has been subsequently named after him [5]. Kounis syndrome although not rare, has remained underrecognized in clinical practice and underreported in clinical literature. We present a case of Kounis Syndrome secondary to intravenous (IV) radiologic contrast administration in a patient who had previously tolerated IV contrast studies.
A 76-year-old male with past medical history significant for prostate cancer (in remission), diabetes, hyperlipidemia and tobacco dependence but no identified coronary artery disease presented to emergency room complaining of Left abdominal and flank pain which started at rest. His initial work-up only revealed significant hematuria and his pain resolved IV Tylenol administration. The cause of hematuria was investigated with a CT abdomen/pelvis with contrast. 130 mL of Iohexol 350 mg iodine/ml (Omnipaque 300) was administered via IV. Within 15 minutes of IV contrast administration, the patient complained of chest tightness and pain radiating to both jaws. He became tachycardiac and hypotensive. An EKG was immediately done which revealed widespread ST depressions in anterolateral leads along with ST elevation in aVR (Figure 1). His Troponin had increased from normal to 0.282 ng/ml. A STAT echo done at bedside which revealed no regional wall motion abnormalities. The Patient was given diphenhydramine and dexamethasone for possible contrast reaction and his hypotension subsequently improved. A follow up EKG was done 30 minutes later which revealed normal sinus rhythm without any ST changes (Figure 2). Patient's troponin continued to increase till it peaked at 5.055 and then gradually resolved. No treatment for an acute coronary event was administered. Patient underwent nuclear vasodilator stress test (Figure 3) which did not reveal any evidence of ischemia. The patient was then treated for his complaint of hematuria which was diagnosed as nephrolithiasis and he made a complete recovery. As the patient's symptoms started immediately after receiving contrast and resolved within 30 minutes of administration of intravenous steroids and Benadryl, his clinical course was consistent with an allergic coronary vasospasm (Kounis syndrome). The inciting factor was determined to be iohexol contrast dye. However, the patient had previously tolerated the contrast on multiple occasions as recently as 4 years ago in a similar radiologic study. Upon discharge contrast (Omnipaque) was added to allergy list and he was given follow-up with urology for nephrolithiasis.
 Figure 1: EKG revealed widespread ST depressions in anterolateral leads along with ST elevation in aVR.
View Figure 1
Figure 1: EKG revealed widespread ST depressions in anterolateral leads along with ST elevation in aVR.
View Figure 1
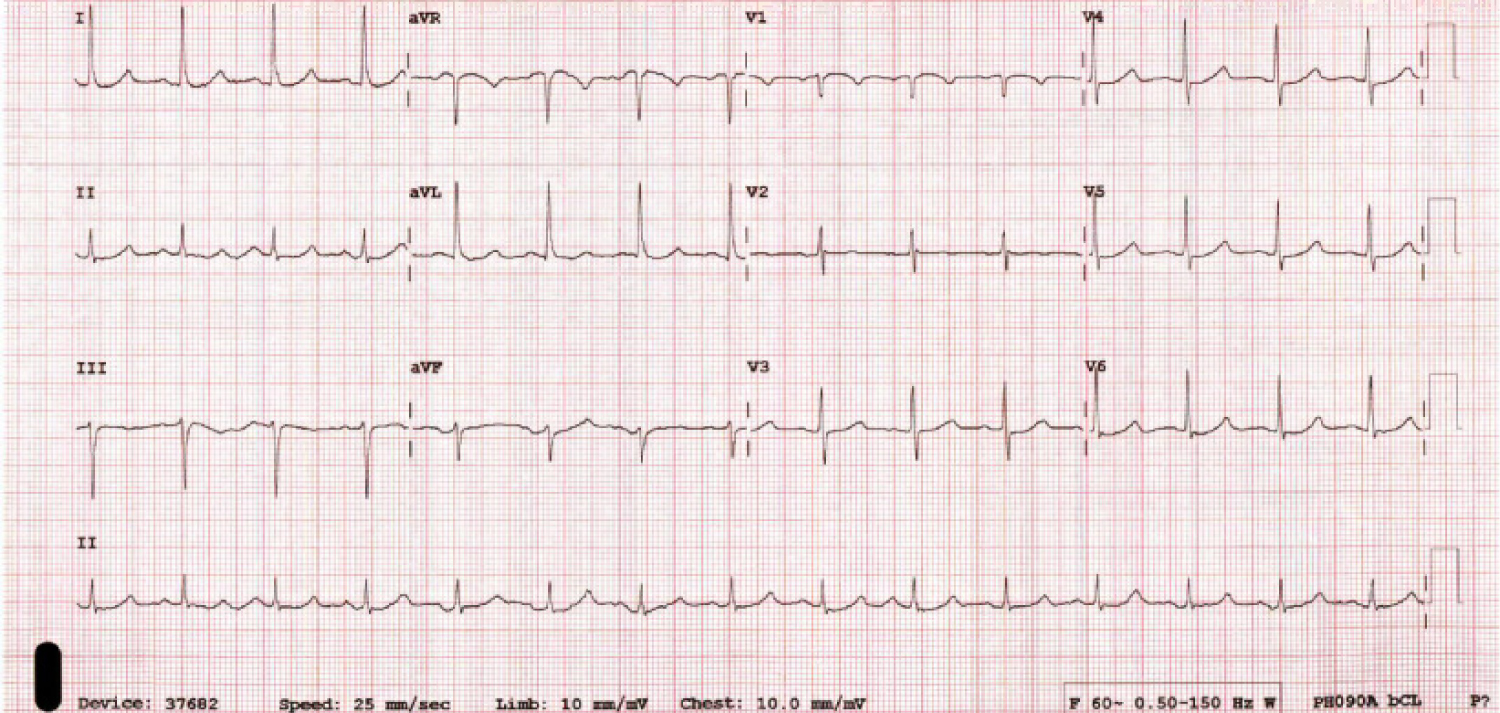 Figure 2: Follow up EKG revealed normal sinus rhythm without any ST changes.
View Figure 2
Figure 2: Follow up EKG revealed normal sinus rhythm without any ST changes.
View Figure 2
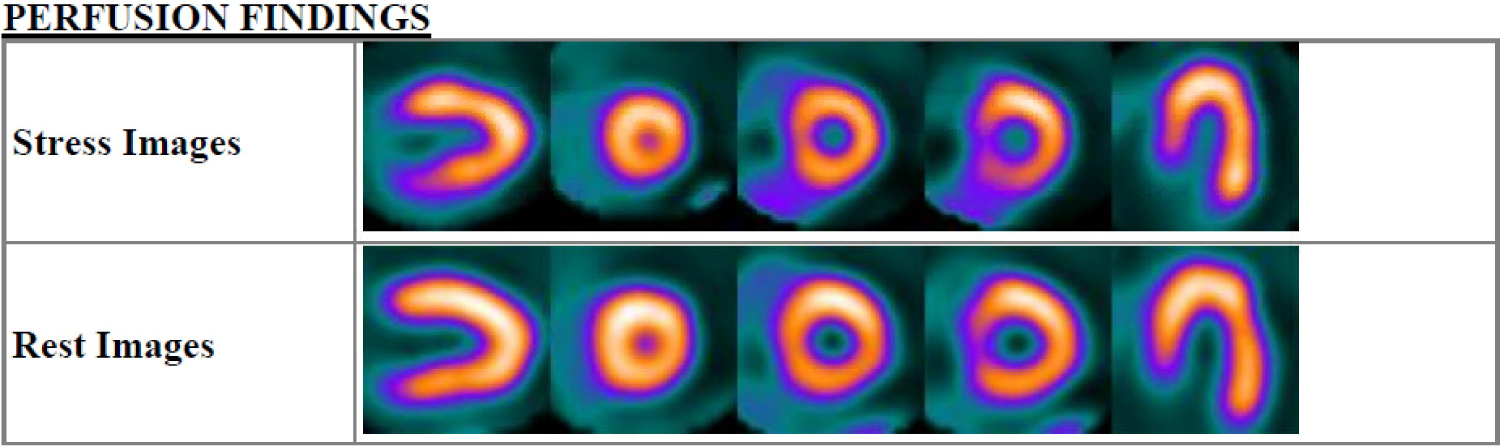 Figure 3: Nuclear vasodilator stress test did not reveal any evidence of ischemia.
View Figure 3
Figure 3: Nuclear vasodilator stress test did not reveal any evidence of ischemia.
View Figure 3
Kounis Syndrome is classified into three separate types. Type I includes patients with no coronary artery disease (CAD) who develop coronary vasospasm which may or may not progress to an acute myocardial infarction with raised cardiac enzymes. Type II includes patients with preexisting coronary atheromatous disease who develop an allergic reaction leading to either a coronary spasm without raised cardiac enzymes or a coronary spasm leading to atheroma erosion or rupture. Type III includes patients who develop stent thrombosis after an allergic reaction [2].
Our patient developed Type I Kounis syndrome after exposure to Iohexol contrast. Iodine based Contrast Media (RCM) has been known to cause anaphylactic adverse effects and has at times led to death secondary to anaphylaxis [6]. The role of RCM has also been established as a cause of Kounis Syndrome [3]. He had previously been given the same contrast in different volumes and concentrations on three separate occasions with no adverse effects. This is likely a new anaphylactic reaction caused by repeat exposure to RCM although there was a gap of 4 years between repeat exposures. Although developing an anaphylactic reaction due to repeat exposure to RCM is fairly common [3], it is worth noting that the association of Kounis syndrome and repeat exposure to RCM has not been determined. Prior case studies have not highlighted if the anaphylactic occurred after an initial exposure or repeat.
Further study can also be done regarding Kounis Syndrome severity upon repeat exposure in comparison to an initial exposure as anaphylactic reactions are often less severe on initial exposure rather than repeat.
Kounis Syndrome remains an underreported and underrecognized cardiac condition. Further studies into potential causes and better recognition of the syndrome may be helpful in management of this syndrome.