Despite considerable improvement in the cardiac replacement therapy including durable left ventricular assist device and heart transplantation, some patients are not good candidates for such intensive therapies given their comorbidities. We had a 58-year-old patient with advanced heart failure who was assigned to INTERMACS profile 2 with progressive end-organ dysfunction refractory to inotropes. Following the detailed discussion, he decided not to receive cardiac replacement therapy dominantly given his comorbidity of schizophrenia. A palliative care team consisting of multidisciplinary medical providers started to commit and prescribed 2.5 mg of morphine together with low-dose anti-heart failure medications, which improved not only his heart failure symptom but also his congestive heart failure itself. Aggressive commitments of the palliative care team with optimal medical therapy, which are tailored depending on each advance care planning, should improve not only patients' quality of life but also advanced heart failure itself.
Heart failure, Ventricular assist device, Morphine, Dyspnea
Survival in patients with advanced heart failure has increased given the increasing number of cardiac replacement therapy including durable left ventricular assist device (LVAD) and heart transplantation in addition to the improvement in pharmacological therapy [1]. However, given the shortage of donor heart, high morbidities following cardiac replacement therapy, its high medical cost, and its extensive invasiveness, many heart failure patients cannot be good candidates of such intensive therapies [2]. Nevertheless, an alternative approach for such cohorts, including palliative care, has not yet been established thus far [3].
We had a patient with advanced heart failure and schizophrenia, who eventually decided to decline to receive cardiac replacement therapy. His heart failure was successfully managed using morphine-incorporated medical therapy following the intervention of palliative care team.
A 58-year-old male patient with a history of schizophrenia for 30 years was admitted to our institute presenting dyspnea at rest, appetite loss, and peripheral edema. Blood pressure was 119/83 mmHg, heart rate was 108 bpm, saturation was 98% on 3 L/min of nasal cannula support. Serum sodium was 131 mEq/L, serum total bilirubin was 0.9 mg/dL, serum creatinine was 1.1 mg/dL, and plasma B-type natriuretic peptide (BNP) was 3167 pg/mL.
Chest X-ray showed cardiomegaly and bilateral pulmonary congestion. Transthoracic echocardiography showed 71 mm of left ventricular end-diastolic diameter and 6% of left ventricular ejection fraction with diffuse severe hypokinesis. He was hospitalized with a clinical diagnosis of congestive heart failure.
Following the initiation of intravenous administration of dobutamine and oral diuretics, his dyspnea and peripheral edema relatively improved (Figure 1). However, 0.625 mg/day of enalapril and 1.25 mg/day of carvedilol rather worsened his pulmonary congestion and hypotension, accompanied by increases in serum total bilirubin and creatinine up to 1.8 mg/dL and 1.7 mg/dL, respectively. He was assigned to the INTERMACS profile 2 with worsening end-organ function refractory to inotropes therapy [1].
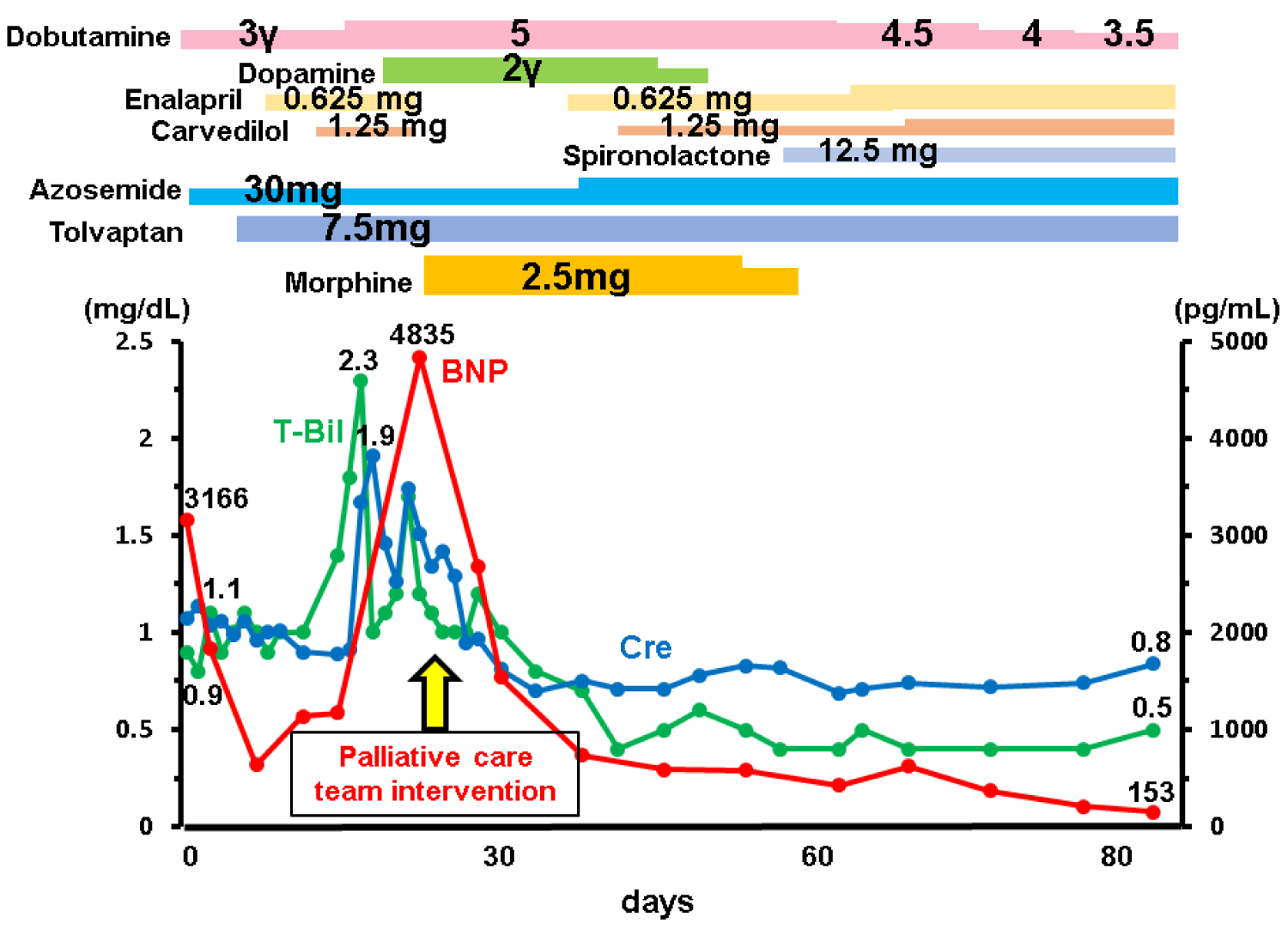 Figure 1: Time course following the hospitalization.
Figure 1: Time course following the hospitalization.
BNP: B-type Natriuretic Peptide; T-Bil: Total Bilirubin; Cre: Creatinine
View Figure 1
Following the detailed explanation of his current clinical condition and repeated discussion with him and his caregivers, they decided to decline any further invasive procedures and treatment, including endo-myocardial biopsy to diagnose etiology, mechanical circulatory supports, and heart transplantation, but rather to receive palliative care.
From day 20, the palliative care team, consisting of multidisciplinary experts (medical doctors, expert nurses, pharmacists, physical therapists, psychotherapists, nutritionists, and medical social workers), participated in the daily care and 2.5 mg/day of intravenous administration of morphine was initiated to ameliorate his persistent dyspnea due to pulmonary congestion following the careful explanation of its adverse effects. His dyspnea improved immediately as well as amelioration of congestive heart failure following the initiation of morphine therapy, which further allowed us to initiate low-dose anti-heart failure medications including enalapril, carvedilol, and spironolactone, followed by a considerable decrease in plasma BNP (from 4835 pg/mL to below 1000 pg/mL) as well as recovery of end-organ dysfunction. Liaison psychiatrists committed to stabilize his mental health and anxiety for his disease. Cardiac rehabilitation was performed to improve his activity of daily life. Social workers soaked external institutions appropriate for his unique medical features.
The dose of morphine was reduced gradually given the improvement of his symptom. On day 82, he was transferred to another institute to continue palliative care with dobutamine infusion.
Patients with advanced heart failure often face major decision makings, such as continuous inotropes infusion via central venous catheter, intra-cardiac defibrillator, and cardiac replacement therapy [4]. Of note, these major interventions should be presented with a balanced description of alternative approaches.
Decision making for cardiac replacement therapy is sometimes challenging, given that it requires complex assessments of the refractoriness of heart failure, relatively preserved end-organ function, the ability of self-management, social support with appropriate caregivers [5]. Given that destination therapy is not approved in Japan [6], candidates of durable left ventricular assist device should also satisfy the indication of heart transplantation beforehand.
Following detailed discussion with multidisciplinary health care providers [7], he and his family eventually decided to decline such an intensive surgical therapy but instead preferred palliative care, predominantly due to his severity of schizophrenia. Such discussion should be repeated if necessary and the decision can be changed. The patient at first declined central venous catheter but later accepted for long-term palliative care with inotropes [8]. Unfortunately, the palliative care team started to commit after the decision, because rapid progression of his heart failure did not allow their early intervention. In principle, the palliative care team had better intervene at earlier stage before hemodynamic deterioration, although it is sometimes challenging in the real-world practice.
Psychological support is another important approach for those with advanced heart failure, given that many heart failure patients are at high risk of depression or any other psychological disorders [9]. Although large-scale randomized control trials could not demonstrate a significant advantage of medical interventions in improving depression and cardiovascular status [10,11], pharmacologic therapy using selective serotonin reuptake inhibitors and tricyclic antidepressants are attempted, if applicable, with careful attention for their side effects including QT prolongation, hypotension, and hyponatremia. The patient was supported by the psychological support team during hospitalization to manage his schizophrenia and heart failure-related anxiety.
Symptom management is a key to palliative care for those with advanced heart failure, and morphine has a dominant role in the literature of cardiac palliative care [12]. Following the detailed discussion with the palliative care team, we initiated morphine at a low dose of 2.5 mg/day. Interestingly, morphine therapy improved not only his dyspnea but also heart failure congestion with improvement in BNP levels. The detailed mechanism remains uncertain, but morphine therapy resulted in a decreased cardiac demand due to sympathetic nerve suppression, an afterload reduction due to peripheral artery dilatation, and a preload reduction due to venous dilatation, all of which ameliorated congestive heart failure and gave us a chance to initiate anti-heart failure agents [13]. Adverse effects of morphine including hypotension and bradycardia were not observed, probably due to concomitantly administered inotropes. In ten heart failure outpatients, Johnson and colleagues also observed that four-day morphine therapy significantly decreased plasma BNP levels compared to the placebo [14]. Further studies to investigate optimal morphine-incorporated medical therapy for those with advanced heart failure are warranted.
TI receives grant support from JSPS KAKENHI: JP20K17143.