Sepsis is global health priority and the leading cause of death in critical care. The SEPSIS 3 criteria introduced in 2016 is the latest tool in diagnosing sepsis. It uses SOFA and qSOFA scores in place of the SIRS criteria for better ability to predict mortality in patients with suspected infections. The performance of these scores in critical care units outside high-income countries remains largely unknown.
We compared the performance of SOFA and qSOFA in predicting the in-hospital mortality of an adult critical care unit in Kenya. We conducted a retrospective review of all patients admitted to the critical care units with suspected infection between 1 January 2017 and 31 December 2017. A standardized electronic data collection tool was be used to collect demographic, clinical and outcome data on the participants. Area under the receiver operating characteristic curves (AUROC) with 95% confidence intervals was used to compare SOFA and qSOFA.
We enrolled 450 patients with a mean age of 56 years [SD ± 19.10] and 57.60% were male. Majority of the patients, 352 (78.20%), presented through the emergency department. Pneumonia was the commonest source of infection 293 (65.10%). There were 92 deaths (mortality rate of 20.44%). The majority of patients, 371 (82.44%) manifested a SOFA score of ≥ 2 and 190 (42.22%) had a qSOFA score of ≥ 2. SOFA score was superior in predicting in hospital mortality compared to qSOFA with an AUROC = 0.799 [0.752-0.846] vs. 0.694 [0.691-0.748, P < 0.001].
A SOFA score of two or more is better than qSOFA score in predicting in-hospital mortality among adult critical care patients with suspected infection. This finding suggests that SOFA is an appropriate tool in the initial diagnosis sepsis in critical care setting in a developing country.
SOFA, qSOFA, Sepsis, Low income countries, Critical care infections
AKUHN: Aga Khan University Hospital Nairobi; APACHE II: Acute Physiology and Chronic Health Evaluation II; AUROC: Area Under Receiver Operator Characteristic Curve; GCS: Glasgow Coma Score; ICU: Intensive Care Unit; IQR: Interquartile Range; LMICs: Low to Middle Income Countries; qSOFA: Quick Sepsis-related Organ Failure Assessment; SIRS: Systemic Inflammatory Response Syndrome; SOFA: Sepsis-related Organ Failure Assessment; SPSS: Statistical Package for Social Sciences; SSC: Surviving Sepsis Campaign
SOFA: Sequential Organ Function Assessment; qSOFA: quick Sequential Organ Function Assessment; AUROC: Area Under Radio Operator Curve; SD: Standard Deviation
Sepsis is a life-threatening condition with organ dysfunction caused by a dysregulated host response to an infection [1]. In 2016, there were an estimated 30 million cases of sepsis and 6 million deaths attributed to sepsis globally [2]. The incidence of sepsis has increased by 8.7% from 1979 to 2000. Sepsis is now the leading cause of critical care mortality [2]. Furthermore, Sepsis survivors have a higher risk for long-term physical, cognitive and psychosocial morbidity [3]. Sepsis is also a costly condition with US$ 20 billion spending annually in the USA alone [4]. In view of these, the World Health Organization (WHO) declared sepsis a global health priority in 2017 [5].
Despite this health impact, defining sepsis has remained difficult, hindered by a variable clinical presentation and absence of a reliable diagnostic test [1]. In March 2016, the third international consensus definition for sepsis and septic shock (SEPSIS 3) was published [1]. SEPSIS 3 defined sepsis as life-threatening organ dysfunction caused by a dysregulated host response to infection. Organ dysfunction is an increase in the sequential (sepsis-related) organ failure assessment (SOFA) score of two points or more. Septic shock is a subset of sepsis with profound circulatory, cellular and metabolic abnormalities associated with a greater risk of mortality (> 40%) than sepsis alone. Septic shock is defined clinically by vasopressor requirement to maintain a Mean Arterial Pressure (MAP) of > 65 mmHg and a serum lactate > 2 millimole per liter (mmol/l) in the absence of hypovolemia [1].
The SEPSIS 3 definition task force also developed a new simple measure for rapidly identifying patients with sepsis termed quick SOFA (qSOFA) incorporating systolic blood pressure < 100 mmHg, altered mental status and a respiratory rate of 22 breaths per min or greater. A score of two or more points in patients with presumed infection defines sepsis. The qSOFA does not require laboratory tests and therefore offers a simple bedside assessment for sepsis, potentially useful in low resource settings.
This new definition (SEPSIS 3) is the most up-to-date view of sepsis, incorporating the advances in the understanding of sepsis pathobiology, especially in distinguishing sepsis from uncomplicated infection. This task force definition also promises to offer easily measurable clinical criteria that captures the essence of sepsis and allows for a more accurate appreciation of the scale of the sepsis problem globally [1].
However, there was no involvement of Low-income countries in the making of the SEPSIS 3 definition. The taskforce of the SEPSIS 3 acknowledged this as a limitation and encouraged further research in these regions, especially in the performance of the new SOFA and qSOFA scores in patients with suspected infections in Low income countries [1].
To the best of our knowledge, there are no studies assessing the performance of the new SOFA and qSOFA scores in low income to middle-income countries in Africa. Generally, there is paucity of data on sepsis from developing countries particularly from sub-Saharan Africa where there is a larger population at risk of sepsis in sub-Saharan Africa due to the high burden of HIV and other infectious diseases predisposing to sepsis at a younger age compared to the high-income countries [6]. The infecting pathogens are also different [6]. Sub-Saharan Africa also has limited critical care capacity in these environments to manage sepsis, affecting outcomes of sepsis patients. These factors make the low-income countries distinctly different and a priority region in sepsis research [7].
The primary aim of is to compare the performance of the SOFA score and qSOFA score in predicting in-hospital mortality among patients with suspected infection in a low-income country setting.
We conducted this study at the Aga Khan University Hospital, Nairobi (AKUH, N) a 258-bed capacity, private, nonprofit, premier teaching hospital offering tertiary level and secondary level healthcare services to the people of East Africa. AKUH, N established in 1958 received the Joint Commission of International Accreditation (JCIA) accreditation in 2013. AKUHN has over 35 beds for critical care, one of the largest critical care capacities in Nairobi city.
We used a retrospective cross-sectional study design.
The study population were all adult patients admitted to the critical care units in the period 1st January 2017 to 31st December 2017. We included all patients aged ≥ 18 and suspected infection at admission; defined as those patients who have bodily fluids sampled for cultures with or without receiving antimicrobials within the first 24 hours of admission to the critical care units. We excluded participants with incomplete data; defined as cases without outcome data (alive or dead at hospital discharge) or lacked necessary data to complete the SOFA and qSOFA score for the first 24 hours of admission to critical care.
The critical admission records were manually screened then checked against the electronic health record using the inclusion criteria. Subsequently, a list of the all cases of suspected sepsis with the patients' identification numbers generated. Primary Outcome was all cause in-hospital mortality as confirmed from the hospital medical records and death register. Secondary outcome was achieving a critical care length of stay of at least three days. Similar to the original SEPSIS 3 study and subsequent studies in other regions of the world that have looked at performance of the SOFA and qSOFA. The SOFA score includes laboratory variables (Partial pressure of oxygen, platelet count, creatinine and bilirubin levels) and clinical variables (Glasgow coma scale and hypotension).
We developed a data abstraction tool to extract variables of interest. Variables of interest included: Demographical information (age and sex), critical care length of stay, and hospital length of stay, status at discharge (alive or deceased) from critical care and hospital, clinical and laboratory variables for the calculation of the SOFA and qSOFA scores. The scores for the first 24 hours of critical care admission were calculated and the highest score in that first 24 hours taken. Trained research assistants abstracted the data electronically using EPI INFO® software version 7.2.2.6. The principal investigator counter checked all the collected data at the end of every week of data collection to make sure accuracy in data collection and compliance with the study protocol.
After data collection and coding, the data moved from to a password-secured Stata database for analysis. For statistical analysis, descriptive quantitative variables were reported using means (± Standard Deviation) or medians (interquartile range (IQR)) according to their distribution. Chi-square test compared categorical variables and Wilcoxon's rank sum test compared continuous variables. Area under the receiver operating characteristic curve (AUROC) with 95% confidence interval was be used to determine discriminatory power of each score. The Hanley and McNeil method compared the differences in the AUROCs of the scores overall and in the subgroup of sepsis patients. All statistical tests were two sided and P value < 0.05 was considered significant.
There were 1790 admissions to the critical care units of AKUHN in the period 1 January 2017 to 31 December 2017. There were 844 patients meeting criteria for suspected infections at admission, of these 394 patients were excluded for various reasons as shown in Figure 1. A total of 450 patients finally formed the study cohort.
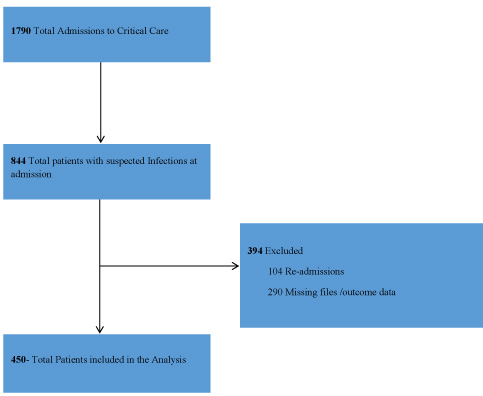 Figure 1: Flow diagram showing the selection of study cohort. View Figure 1
Figure 1: Flow diagram showing the selection of study cohort. View Figure 1
The demographic and clinical profiles of the patients are provided in Table 1 below. The age of the patients ranged between 18 and 98 years with a mean age of 56 years [SD ± 19.10]. The majority were male 259 (57.6%). Non-survivors were older (59 vs. 52 years, P = 0.002).
Table 1: Baseline characteristics of participants. View Table 1
Majority of the patients, 352 (78.2%) came to the critical care units through the emergency department. The mortality rate was higher among patients referred from other sources compared to the emergency department (33.67% 16.76%, P < 0.001).
The most common comorbidity was diabetes mellitus, 123 (27.3%), followed by malignancy, 74 (16.5%). In the study cohort, 40 (8.9%) were HIV positive. Patients with liver disease and malignancy had a higher mortality, 7.3% vs. 15.2%, P = 0.05 and 11.7% vs. 34.8%, P < 0.001 respectively.
The commonest sites of infection were respiratory system, 293 (65.1%), followed by urinary tract 102 (22.7%) and bloodstream infection 98 (21.8%). The patients with a respiratory source of infection had a higher mortality (67.6% vs. 55.4%, P < 0.029). Patients with bloodstream infections also had a higher mortality (19.3% vs. 31.5%, P < 0.011). The same is reflected in culture yield, with a higher mortality among those with culture positive results (16.4% vs. 38%, P < 0.001). Overall, 92 (20.9%) patients had a positive culture.
The most common organisms isolated from blood were Escherichia coli (29.5%), Klebsiella pneumonae (2.13%) and Staphylococcus aureus (9.8%). Among the isolated Escherichia coli, 41.4% were extended spectrum β-lactamases producing (ESBL). Majority 55.2% were sensitive to most commonly used antibiotics including penicillins and cephalosporins.
Of the 450 patients recruited, 371 patients (82.4%) had a SOFA score of two or more and 190 (42.2%) patients had qSOFA score of two or more Table 2. The distribution of each score and relationship with in-hospital mortality and critical care stay of three or more days are presented in Figure 2 and Figure 3 below.
 Figure 2: Mortality at SOFA score on critical care admission among patients with infection. View Figure 2
Figure 2: Mortality at SOFA score on critical care admission among patients with infection. View Figure 2
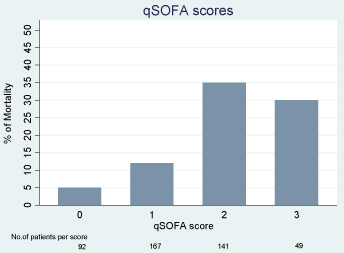 Figure 3: Mortality by qSOFA score at critical care admission among patients with infection. View Figure 3
Figure 3: Mortality by qSOFA score at critical care admission among patients with infection. View Figure 3
Table 2: Baseline characteristics of participants. View Table 2
In hospital mortality was 24.53% and 34.21% for patients with SOFA and qSOFA scores of two or more respectively (P < 0.001). Non-survivors had a longer critical care length of stay compared with survivors (median length of stay of 3 days vs. 5 days, P < 0.008) Table 3.
Table 3: Baseline characteristics of participants. View Table 3
Prediction of in-hospital mortality was significantly higher using SOFA (AUROC, 0.799 [95% CI, 0.752 to 0.846]) than qSOFA (AUROC, 0.694 [95% CI, 0.641 to 0.748]); all p < 0.001 (Figure 4). When considered in conjunction with baseline prediction of mortality, SOFA (AUROC, 0.822 [95% CI, 0.744-0.869]) outperformed qSOFA (AUROC, 0.751 [95% CI, 0.695-80.7]) for prediction of in hospital mortality.
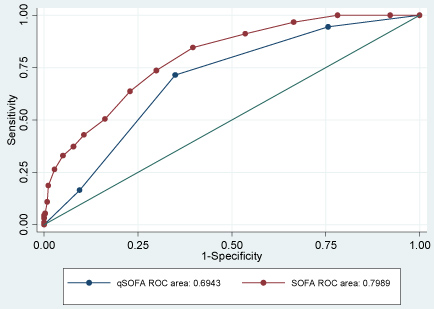 Figure 4: Crude AUROC-critical care mortality. View Figure 4
Figure 4: Crude AUROC-critical care mortality. View Figure 4
The superior performance of SOFA was not maintained in the secondary outcome of a critical care length of stay of three or more days, SOFA (AUROC, 0.658 [95% CI, 0.605-0.712]) vs. qSOFA (AUROC, 0.669 [95% CI, 0.621-0.717]).
In this study comparing the performance of SOFA score with qSOFA score in predicting in hospital mortality among critical care patients in a low-income country, SOFA score was superior to qSOFA score. There was no difference in the predicting prolonged critical care stay between the SOFA and qSOFA scores.
Recent study by Seymour, et al. [6] in Pittsburg, USA in 2016 showed SOFA was superior in discriminating for in hospital mortality among critical care patients, with an AUROC of 0.74 (95% CI 0.73-0.76) compared to qSOFA with a AUROC of 0.66 (95% CI, 064-0.68). In another high income setting of Australia and New Zealand, Raith, et al. [8] also showed a SOFA to be superior to qSOFA in predicting for in hospital mortality among critical care patients with an AUROC 0.753 (95% CI, 0.750-0.757) compared to AUROC of 0.607 (95% CI, 0.603-0.611) for qSOFA. This study the SOFA was superior to qSOFA with a slightly higher AUROC of 0.799 (95% CI, 0.75-0.846) for SOFA and AUROC of 0.694 for qSOFA (95% CI, 0.641-0.748). In a middle income setting of Thailand in 2018, Khwannimit, et al. [9], showed similar higher AUROCs with SOFA (AUROC 0.839) superior to qSOFA (AUROC 0.814). In these studies, by Seymour, et al. [10], Raith, et al. [8] and Khwannimit, et al. [9], SOFA also showed superiority in predicting prolonged critical care stay. In this study, there was no difference in predicting for prolonged critical care stay between SOFA and qSOFA, attributed to the fewer patients with qSOFA score more than two in this study.
This study cohort had more males than females in keeping with similar studies by Seymour, et al. [10], Raith, et al. [8] and Khwannimit, et al. [9]. This may be explained by the gender difference in sepsis with males having a higher predisposition [11]. Patients in our study were younger with a mean age of 54 years compared to 62 years in both Raith, et al. [8] and Khwannimit, et al. [9]. This reflects the underlying demographic differences in the settings with older populations in both USA and Thailand compared to Kenya [12]. In severity of illness, this study cohort had a comparable proportion of patients with SOFA score of two or more compared to the Raith, et al. [8] in Australia and New Zealand (82.44% Vs. 90.1%) [8]. The same for qSOFA score of two or more (42.22% Vs. 54.4%) [8]. Overall mortality was higher in this study cohort with mortality rate of 20.44% compared to 18.7% in the Raith, et al. [8]. The higher mortality in patients with relatively less severe illness and younger age attributed to differences in co morbidities with higher number of malignant disease in this study cohort. The overall mortality rate among this cohort of with suspected sepsis is less than the overall critical care mortality in a public critical care unit at Moi teaching and referral hospital, Eldoret, Kenya, with a 53% overall critical mortality and 80% mortality among sepsis patients [13]. The patient to critical care health care professionals and better access to advanced diagnostics and critical care therapies at AKUH, N critical care units likely explains the difference in mortality rate. The average length of critical care stay was four days in our cohort similar to other studies to Raith, et al. [8], Khwannimit, et al. [9] and Seymour, et al. [10]. The overall hospital length of stay was longer in the Khwannimit, et al. [9] cohort with an average length of hospital stay of 16 days compared to this study cohort's 8 days, likely due to differences in patient characteristics with an older patient pollution in the Khwannimit, et al. [9]. There may also be differences in care and discharge protocols in the settings.
In comorbidities, there were significant differences between this cohort and studies higher income countries. In Raith, et al. [8] cohort only 0.1% had HIV/AIDS compared to 8.9% in our cohort. This reflects the differences in prevalence of HIV in Kenya at 4.8% in 2017 [14] compared to Australia and New Zealand at 0.1% in 2017 [15]. There were also more patients with diabetes (27.3% vs. 3.5%) and malignancies (16.5% vs. 3.2%) in this cohort compared to the Raith, et al. [8] cohort. This may reflect differences in the overall diagnosis and management of these conditions. There is earlier diagnosis and better treatment options in the higher income countries compared to low income countries [16]. This earlier and better treatment reduces the number of cancer patients requiring critical care admission [17].
The commonest source of infection was the respiratory system followed by urinary tract source in keeping with Seymour, et al. [10], Raith, et al. [8] and Khwannimit, et al. [9]. There is a low MRSA prevalence in this study at 9% compared to higher income countries, like USA with a prevalence of 41% [18]. The MRSA prevalence of < 10% is similar to a study at AKUH, N in 2014, that showed a prevalence of 4.8% [19] and other African countries like in Madagascar with 4.4% [20]. The commonest organism was E.coli followed by K. pneumonia similar to both Raith, et al. [8] and Khwannimit, et al. [9] cohorts. We had a high proportion of prevalence of ESBL producing bacteria among our gram-negative isolates (44.1%) compared to 2.6% in most parts of Europe [21]. Therefore, there are distinct differences in pathogen antibiotic resistance patterns in this study cohort compared to high-income countries. It is unclear how this affects the patient outcomes. Further study would be required.
This study has confirmed that a SOFA score of two or more points within the first twenty-four hours in critical care had a good predictive for in hospital mortality. The study also demonstrated SOFA was superior to qSOFA in predicting in hospital mortality in this cohort of critical care patients with suspected infection at the point of admission in a low-income country. This suggests that SOFA would be an appropriate data based starting point in diagnosing sepsis in a developing country population as suggested in the consensus statement of SEPSIS 3 definition [1].
The main limitations of this study are it is from a single well-resourced center study and the retrospective nature with missing data and excluding patients who develop sepsis latter in to their stay in the critical care units or patients with sepsis outside the critical care setting. This limits generalizability. We also did not explore the uniformity of sepsis management. Improper management of sepsis may affect the outcome. We recommend further research on sepsis management and outcomes, looking prospectively at compliance with surviving sepsis bundles or other guideline-based sepsis management and related outcomes.
The present study demonstrated that among adult patients with suspected infection at admission to critical care, a SOFA score of two or more was better than qSOFA score of two or more in predicting in-hospital mortality. This finding suggests that SOFA is an appropriate tool in the initial diagnosis sepsis in critical care setting in a developing country. This is in keeping with Sepsis 3 consensus recommendation.
We obtained ethical approval from Institutional Research and Ethics Committee of AKUH, N, reference number 2018/REC-60, see below. This study had a waiver of informed consent granted because we were reviewing medical records of discharged patients. In addition, patient data were de-identified.
The authors for the study: "Comparison of the sequential organ failure assessment (SOFA) and quick SOFA scores in predicting in-hospital mortality among adult critical care patients with suspected infection" listed on the title page and below have all reviewed and approved the submitted version of this article for publication. This article has not been published or submitted for publishing in any other journal. The content contained in this submission does not require any special permission from other journals or authors.
All data generated or analysed during this study are available from the corresponding author on reasonable request.
The authors declare that they have no competing interests.
The Aga Khan University provided a research grant of US dollar 1000 to assist in the data collection by paying for data collection clerks.
MS, RS and WS coordinated the data collection, analysed and interpreted data for the comparison of SOFA and qSOFA in predicting critical care mortality. All authors read and approved the final manuscript.
We thank Dr. Abdulaziz Mansour for proofreading and editing of this paper. Special thanks to the medical records department at Aga Khan University Hospital, especially Mr. James Kaburia and Ms. Helda Amariata. Finally, we are grateful to our data collection clerks Julia Njoroge, Adelaide Nam, Priya Dhanda and Aditi Vakil.