With aging, occurs a decrease in the number of melanocytes active enzymatically around 12.0% to 24.0% every ten years. As a treatment, stem cell therapy with adult stem cells has been the focus of many studies. Among adult stem cells, adipose-derived stem cells (ADSC) ubiquinone, known as coenzyme Q10 (CoQ10), is a lipid-soluble antioxidant. It is shown to reduce lipid peroxidation of low-density lipoprotein regenerates endogenous vitamin E and protects cells against oxidative stress induced by UV radiation.
To explore through the literature review the use of cellular therapy with stromal vascular fraction and coenzyme Q10 to meet the dermatological aesthetics.
Use of Mesh terms: Adipose-derived stem cell. Estromal Vascular Fraction. Aesthetics. Dermatology. In the main databases such as Pubmed, Medline, Bireme, EBSCO, Scielo, etc. The total of 63 papers that were submitted to the eligibility analysis was cross-checked and after that 23 studies were selected, following the rules of systematic review-PRISMA.
The production and secretion of growth factors have been identified as an essential function of ADSC, and many skin rejuvenation effects have been demonstrated [1,2]. Thus, ADSC has been shown to stimulate collagen synthesis and dermal migration of fibroblasts during the wound healing process. In addition, the secreted factors of the ADSC protect the dermal fibroblasts against oxidative stress. CoQ10 is also known as ubidecarenone or ubiquinone. This liposome penetrates deep into the epidermis and releases noble actives directly into the sites of action. Powerful antioxidant reduces the organic aging process.
The use of stromal vascular fraction is an important option for dermatological aesthetics, according to the observation of the results obtained in this study. This procedure should be improved and has been widely discussed, mainly because it can be performed as an autologous material and associated with the use of coenzyme Q10.
Adipose derivated stem cell, Estromal vascular fraction, Aesthetics, Dermatology
With aging, occurs a decrease in the absorption of some substances, such as hydrophilic substances [3]. Thus, there is a decrease in the number of melanocytes active enzymatically around 12.0% to 24.0% every ten years [4]. The loss of thickness of the dermis accentuates with age. There is a decrease in collagen and elastic fibers. Wrinkles are the results of this decrease [4].
As a treatment, stem cell therapy with adult stem cells has been the focus of many studies, due to the absence of ethical problems that embryonic stem cells present, as well as a carcinogenic potential [3,4]. Among adult stem cells, adipose-derived stem cells (ADSC) have essentially the same properties as stem cells derived from bone marrow [4,5].
In addition, they have advantages in greater accessibility and relative abundance compared to other types of adult stem cells [6]. Experiments using ADSC have been explored more frequently in recent years. In dermatology, there are several studies on the effective application of stem cells, such as antioxidant action and effects on rejuvenation [1].
Among the latest publications, the effects of ADSC on wound healing, as well as sun damage [2], stand out. The stromal vascular fraction (SVF) of adipose tissue is a rich source of pre-adipocytes, mesenchymal stem cells, endothelial progenitor cells, T and B cells, monocytes, macrophages, and fibroblasts. Because it contains a large population of stem cells derived from adipose tissue, it has the ability to differentiate into several lineages [7,8]. The aging of the skin involves a number of different degenerative processes, as well as a significant decrease in the collagen produced by fibroblasts. Several cytokines and growth factors are also involved, stimulating the synthesis of collagen by fibroblasts for skin rejuvenation [9].
Regenerative medicine that uses stem cells and own body growth factors is an alternative therapeutic strategy for repairing damaged tissues. However, there are still few reports on the antiaging effects of SVF derived from adipose tissue [10-14].
In addition, ubiquinone, known as coenzyme Q10 (CoQ10), is a lipid-soluble antioxidant [15-17]. It is shown to reduce lipid peroxidation of low-density lipoprotein regenerates endogenous vitamin E and protects cells against oxidative stress induced by UV radiation. It was tested that ubiquinol cream reduces the depth of wrinkles [18,19].
In this sense, CoQ10 is an essential lipid molecule for aerobic organisms. It participates in the production of ATP by oxidative phosphorylation, transferring electrons from respiratory complexes I and II to complex III in the internal mitochondrial membrane. In addition, CoQ10 participates in many other vital functions within the cell [20,21]. However, CoQ10 supplementation is widely recommended in high doses (30.0 mg/kg in children and at least 600.0 mg daily in adults) for all patients with mitochondrial diseases, since it is a supplement that has no side effects and brings many benefits to the patient metabolism. Because it is lipophilic, CoQ10 is transported in the circulation by lipoprotein particles [22,23].
Therefore, the present study aims to explore through the literature the use of cellular therapy with SVF and coenzyme Q10 to meet the dermatological aesthetics.
Selection criteria: Cases series, Prospectives, Retrospectives, Randomized, double-blind, placebo-controlled trials in humans with a publication time of the last ten years were selected and analyzed.
Study selection and risk of bias in each study: Two independent reviewers performed research and study selection. The data extraction was performed by reviewer 1 and fully reviewed by reviewer 2. A third investigator decided some conflicting points and made the final decision to choose the articles. Only studies reported in Portuguese and English were evaluated. The Cochrane instrument was adopted to assess the quality of included studies [24].
Search strategy and information sources: In general, as an example, the search strategy in MEDLINE/Pubmed, Web of Science, Science Direct Journals (Elsevier), Scopus (Elsevier), One File (Gale) followed the following steps:- search for mesh terms (Adipose derivated stem cell. Estromal Vascular Fraction. Aesthetics. Dermatology), - use of the booleans "and" between mesh terms and "or" among historical findings.
Summary of literary findings: The literature summarizes the qualitative and quantitative data such as type of study, complications, success rate using the stromal vascular fraction and coenzyme Q10 for aesthetic treatments (Figure 1).
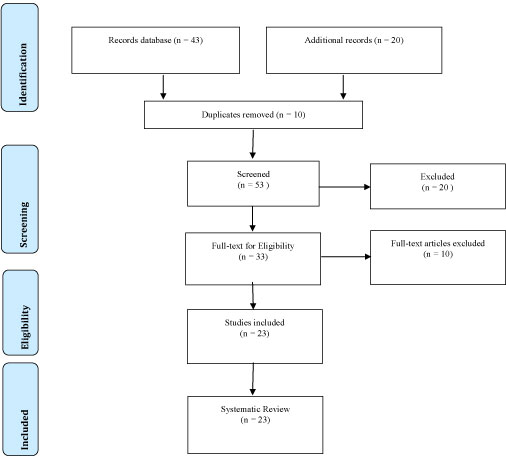 Figure 1: Flow Chart. View Figure 1
Figure 1: Flow Chart. View Figure 1
Risk of bias: Considering the Cochrane tool for risk of bias, the overall evaluation resulted in 12 studies with high risk of bias and 5 studies with uncertain risk. Also, absence of the source of financing of pharmaceutical companies responsible for the marketing of medicines. Only three articles did not present the source of funding, while 13 did not disclose this information in the conflict of interest statement.
With the evolution of aging, the skin undergoes changes such as irregular pigmentation, thinning and loss of elasticity [3,4]. The factors that trigger skin aging may be intrinsic or chronological, composing a natural process, related to genetic factors, shortening of telomeres and action of free radicals; and extrinsic, constituting photoaging [5].
In that sense, regenerative medicine that uses body stem cells and growth factors is an alternative therapeutic strategy for repairing damaged tissues and is becoming a predominant cell-based therapy [6]. Stem cells derived from adipose tissue (ADSC) secrete growth factors such as vascular endothelial growth factor (VEGF), a growth factor similar to insulin (IGF), hepatocyte growth factor (HGF) [1].
In this context, the production and secretion of growth factors have been identified as an essential function of ADSC, and many skin rejuvenation effects have been demonstrated [1,2]. Thus, ADSC has been shown to stimulate collagen synthesis and dermal migration of fibroblasts during the wound healing process. In addition, secreted ADSC factors protect dermal fibroblasts against oxidative stress induced by UVB radiation and chemicals [2,7].
Evidence reinforce the critical role of growth factors derived from ADSC in wound healing, the antioxidant effect and improves the texture and appearance of skin wrinkles, showing that can be good candidates for the treatment of photoaging [8]. EVF of adipose tissue is a rich source of pre-adipocytes, mesenchymal stem cells, and endothelial progenitor cells, which have great differentiation capacity in several lineages. For this reason, it has been extensively studied in aesthetic procedures, correction of scars and treatment of this and deep grooves in photoaging [9].
One study evaluated the effect of EVF on the treatment of deep grooves and found that there was clinical improvement perceived by the patients and by the observer physician, evidenced by the increase in the percentage of collagen fibers [10]. Regarding the thickness of the dermis, in most patients, there was no significant increase in relation to the control. One explanation for this may be related to a technical error at the time of biopsy, perhaps held in areas containing the entire thickness of the dermis and subcutaneous tissue and areas without the presence of all layers of the dermis, thus justifying the maintenance of thickness or even its decrease after the procedure [10].
Therefore, the application of EVF may present good clinical results, with histological confirmation, but it needs further studies to standardize the obtaining of the material, as well as for the development of the application techniques [11-14].
Fredrick Crane, in 1957, discovered Coenzyme Q10 (CoQ10) in the mitochondria of the ox's heart, and in 1958 its physicochemical properties were revealed [15]. This compound is a quinone, similar to a vitamin, is liposoluble and a crystalline powder in its pure form [16]. CoQ10 is also known as ubidecarenone or ubiquinone. This liposome penetrates the epidermis is released noble directly at the sites of action. Antioxidant power reduces the process of organic processing [17]. Can be used in hair products, cream milk, gels, sunscreens, and post-sun lotions. They may be associated with Tinol, nutripeptides [18].
The pH stability is between 4.8 and 8.0. Used in concentrations of 0.50 to 10.00%. Liposomes are tiny vehicles characterized by phospholipids dispersed in aqueous media, which carry an aqueous volume inside them, which can be used for active air transport [18,19]. The phospholipids are organized and may consist of one or multiple layers. We have a great affinity with the skin and we have the moisturizing and restorative effect on the protective lipid barrier of the epidermis. The liposomes are sensitive to the surfactant that is why they are carried in gas. They are used in concentrations of 2.0 to 5.0% [20].
CoQ10 is part of the electron transport chain and is found in large concentrations in the mitochondria, especially in the muscles, brain, and heart [20,21]. However, because they are organs more vulnerable to the action of oxygen free radicals, Q10 exerts an important protective antioxidant action. However, due to aging, genetics, and consumption of statins, the amount of CoQ10 is decreased [22].
Its synthesis can occur through the cycle of mevalonate, responsible for the production of cholesterol, or it can be obtained by feeding, but the amount obtained by these means may not be sufficient [23]. Clinical studies have shown that the use of coenzyme Q10 (from 30 mg dia-1 to 3000 mg dia-1) is essential to inhibit the progression and reduction of the above-mentioned diseases [22]. The dose of CoQ10 that can be obtained with food intake, about 2-5 mg dia-1, is not sufficient to meet the needs of the organism [22], because only 10.0% is absorbed slowly from the treatment intestinal due to high molecular mass and low solubility in water [22].
The cytotoxicity of natural killer cells in the population of healthy elderly women is dependent on the plasma concentration of CoQ10 [15-17]. It is also capable of altering the immune response by decreasing the proinflammatory cytokines IL-6 and TNF-α, which are involved in the progression of myocardial infarction [18]. In addition, CoQ10 reduces the number of lipid peroxides found in atherosclerotic lesions [19]. Thus, CoQ10 protects the lipids present in cell membranes as well as plasma lipoproteins [19].
The use of stromal vascular fraction is an important option for dermatological aesthetics, according to the observation of the results obtained in this study. This procedure should be improved and it has been widely discussed, mainly due to the possibility of being performed as an autologous material and associated with the use of coenzyme Q10.