Fox-Fordyce disease (FFD) is an uncommon chronic inflammatory skin disease of the apocrine sweat glands that could be considered as a rare adverse event of laser hair removal. It is postulated that laser therapy could induce damage to the follicular infundibulum, resulting in epidermal detachment and altered keratinocytes maturation which led to keratin plugging. Here, we present a case of a post-pubertal woman who developed axillary itchy lesions with clinical and histological features compatible with FFD, after a series of axillary laser hair removal treatments. The management of the condition is unsatisfying: We suggested our patient stopping epilation sessions and applying topical corticosteroids, with good response on symptoms but no significant effect on the lesions.
Fox-Fordyce disease, Miliaria, Laser hair removal, Diode laser
Fox-Fordyce disease (FFD) is an uncommon chronic inflammatory skin disease of the apocrine sweat glands mostly affecting post-pubertal women. The exact etiology of the disease remains unknown and different causes have been suggested, such as hyperhidrosis and hormonal factors [1,2]. In recent years few cases of FFD following laser hair removal have been reported, proposing it as a novel cause of FFD [3]. We report the case of a 17-year-old woman who developed itchy papules of the axillae following laser hair removal, with clinical and histological features compatible with FFD.
A 17-year-old woman was referred to our clinic for the evaluation of bilateral axillary mild itchy lesions since eight months. Four weeks before the onset of her symptoms, she had done the second session of 810 nm Diode Laser (Mediostar Next, Esthelogues.r.l., Calenzano, Firenze, Italy) for axillary hair removal. She denied any similar eruption in the past neither adverse reactions after the first laser session. Dermatological examination showed multiple dome-shaped, few millimetres size, skin-coloured, discrete follicular papules within the axillary vault bilaterally; some hair shafts of a few millimetres were observed between papules, and other cut shafts were centred on papules (Figure 1). Physical examination was otherwise normal. A biopsy specimen performed from the axillary papules revealed dilatation of the apocrine secretory unit, with prominent dilatation of the follicular infundibulum, follicular hyperkeratosis and keratin plug; there was periductal and perifollicular infiltration of inflammatory cells and a mild perifollicular fibrosis (Figure 2). Few foam cells were identified.
 Figure 1: Multiple skin-coloured follicular papules on the axilla vault. View Figure 1
Figure 1: Multiple skin-coloured follicular papules on the axilla vault. View Figure 1
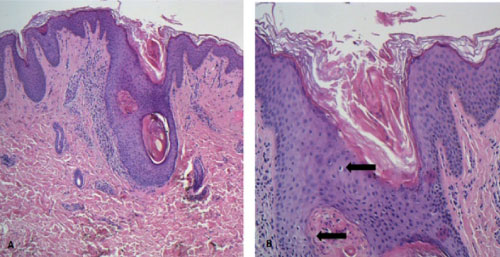 Figure 2: A) Histopathological examination revealing dilatation of the apocrine secretory unit, with prominent dilatation of the follicular infundibulum, follicular hyperkeratosis and keratin plug (haematoxylin and eosin; H&E); B) Dyskeratosis of the follicular infundibulum. View Figure 2
Figure 2: A) Histopathological examination revealing dilatation of the apocrine secretory unit, with prominent dilatation of the follicular infundibulum, follicular hyperkeratosis and keratin plug (haematoxylin and eosin; H&E); B) Dyskeratosis of the follicular infundibulum. View Figure 2
Clinical pathologic correlation was consistent with FFD and the close temporal relation with the laser treatment led us to consider it as FFD- laser induced.
She was prescribed topical 0.1% methylprednisolone aceponate cream twice daily for 2 weeks then once daily for 2 weeks with good response on symptoms but no significant effect on the lesions.
Fox-Fordyce disease (FFD) is an uncommon chronic inflammatory skin disease of the apocrine sweat glands, mostly affecting post-pubertal women. The etiology of disease is unknown but marked female predominance, rarity prior to puberty and, by contrast, remission after menopause suggest a role for hormones [1]. It is characterized by numerous pruritic skin-coloured, dome-shaped, follicular papules localized on gland-bearing areas (axillae, areola, umbilicus and ano-genital area). Histopathological features include dilation of the follicular infundibulum with plugging, dyskeratosis of the infundibular epithelium and follicular hyperkeratosis; there is an associated periductal lymphohistiocytic infiltrate with typical foam cells and mild perifollicular fibrosis [4].
The exact pathogenesis of the disease is still controversial, but it seems to be secondary to obstruction of the apocrine duct due to keratinocytes dysmaturation that leads to hyperkeratosis and keratin plugging; blockage of the apocrine duct will lead to sweat retention, dilatation of the apocrine glands and, in time, rupture of the apocrine system and secondary inflammation [5]. Furthermore, the inciting event that triggers the chain of events remains elusive.
Recent reports indicated laser hair removal as a possible novel cause of FFD [5]. Non-ablative laser hair removal devices target the melanin pigment in hair shaft cells, heat it up and destroy the basal stem cells in the follicle with a permanent hair reduction [6]. It is postulated that laser therapy could induce damage to the follicular infundibulum, resulting in epidermal detachment and altered keratinocytes maturation which led to keratin plugging. The damage seems to be heat related rather than wavelength specific [3], as shown by different types of laser (Diode, Alexandrite, IPL) utilized in the cases of laser induced FFD reported in the literature.
The risk of development FFD after laser hair removal still remain very low, but must be considered in patients with a temporal correlation between the outcome of disease and a laser hair removal therapy.
Therapeutic alternatives for FFD mainly aim at reducing pruritus. First line therapy consists of atopical approach with corticosteroids, calcineurin inhibitor, retinoids and clindamycin [7]; they usually act on symptom with no significant efficacy on skin lesions. New procedural therapies, such as plastical surgery, fractionated microneedle radiofrequency, fractional carbon dioxide laser, pulsed dye laser [8], may be proposed to remove the cutaneous lesions, but there is lack of evidence regarding their usefulness. In cases of laser induced FFD is also essential to stop epilation sessions, as it could act as trigger factor in susceptible patients (to FFD development).
This article has no funding source.
The Authors do not have any conflict of interest to declare.