Macrodystrophia lipomatosa is a rare congenital anomaly causing localized or generalized gigantism. Characterized by an abnormal excessive growth of mesenchymal elements in particularly fibro-adipose tissue, bone, tendon, nerves and vessels. We report our experience in surgical management of a case with Macrodystrophia lipomatosa involving the second toe of the left foot. A through clinical and radiological assessment followed by surgical second ray amputation and soft tissue debulking of the left foot. On the literature review, we found that this disorder in not common in this age group and most of the prosed treatments are suggestive of solo soft tissue debulking. In this report we describe more details about the surgical technique in term of complete resection of the diseased toe and metatarsal resection rather than multiple soft tissue debulking procedures.
Macrodystrophia lipomatosa, Macrodactyly, Local gigantism, Megalodactyly
Macrodystrophia lipomatosa (MDL) is a rare congenital anomaly not hereditary disease causing localized or generalized gigantism, which can be manifested from infancy to late adulthood [1,2]. It's characterized by an abnormal excessive growth of mesenchymal elements in particularly fibro-adipose tissue, in addition to bone, tendon, nerves and vessels [1]. Various causes exist, which can lead to increase in the size of one or several fingers or toes. But though, the exact etiology of MDL is not known [3,4]. Generally, most of the patients are asymptomatic but they seek a physician's advice for cosmetic surgery. Sometimes the patients' complaints are related to mechanical issues or symptomatic neuro-vascular compressions [5,6].
We have found multiple case reports and review articles discussing the radiological and natural history of the MDL; majority in young age groups and upper extremity cases. There were one article by Dr. Fransen [7] and his group who described a similar case of adult patient treated by soft tissue debulking.
In this report we describe more details about the surgical technique in term of complete resection of the diseased toe and metatarsal resection rather than multiple soft tissue debulking procedures.
A 26-year-old male, who has been referred from family medicine because of a congenital anomaly involving his left foot. He has been suffering of an isolated deformity of the second toe in the form of enlargement of the second toe of the left foot; medically called Macrodystrophia lipomatosa. The patient is living in a rural area where no specialized orthopedic surgeon was accessible. The patient was first evaluated for the same issue at age of 8 years. He was offered surgical intervention in the form of soft tissue debulking; however, neither medical nor surgical interventions were pursued by the family till his last visit to my clinic at age of 26 years. The patient main complaint was difficulty in finding appropriate shoes, difficulty in walking and social isolation. All because of the difference in shoe's size and social embarrassment. He reported no pain, no trauma, and no constitutional symptoms.
Physical examination upon presentation demonstrated left foot second toe enlargement with major discrepancy in shape of the left foot and second toe without significant deformity or mal-alignments (Figure 1A and Figure 1B). The medial column was stable in examination and the patient was maintaining symmetrical arch compared to the right foot. Range of motion at the second toe inter-phalangeal joints, Metatarso-phalangeal joint, and mid-tarsal joints were with in normal limits. The second toe was three times the length and five times the size of the toes in the same foot and the toes on the other foot. The ankle and hind-foot joints were comparable to the other foot with no significant abnormalities. The tibialis posterior and dorsalis pedis arteries were detected with clinical examination. The patient demonstrated intact sensations to light touch in all the areas of sensory distribution of the left lower extremity.
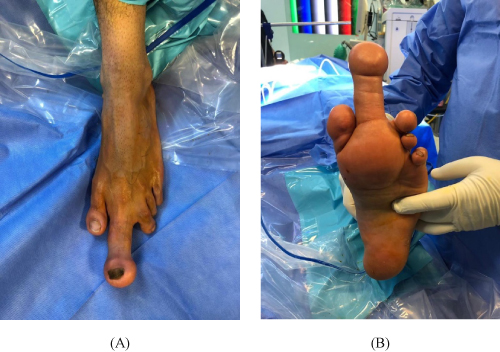 Figure 1: A) Plantar; B) Anterior-Posterior clinical photograph demonstrates the Macrodystrophia lipomatosa involving the second toe of the left foot. View Figure 1
Figure 1: A) Plantar; B) Anterior-Posterior clinical photograph demonstrates the Macrodystrophia lipomatosa involving the second toe of the left foot. View Figure 1
Radiographic examination included 3 weight bearing views of the foot and ankle. These revealed an enlargement of the second toe phalangeal bones, increased first and second web spaces, and large second metatarsal with bulky soft tissue at the second metatarsophalangeal joint (Figure 2A and Figure 2B). Given the history and clinical examination of the disorder to the second toe; MRI study was ordered to better delineate the anatomy of the forefoot. The MRI study showed an enlargement of left second toe that involving the subcutaneous fatty tissue as well as the phalanges and the distal part of the second metatarsal indicating lipomatosa dystrophy. No definite vascular malformation or focal soft tissue lesion (Figure 3A, Figure 3B and Figure 3C).
 Figure 2: Plain films A) Anterior-posterior; B) Oblique radiographic images revealing Macrodystrophia lipomatosa of the second digit of left foot. View Figure 2
Figure 2: Plain films A) Anterior-posterior; B) Oblique radiographic images revealing Macrodystrophia lipomatosa of the second digit of left foot. View Figure 2
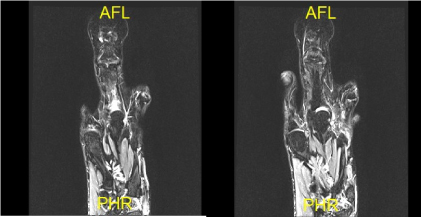 Figure 3A: Axial views of the forefoot that shows the relative size of the second toe compared to other toes with normal surrounding soft tissue. Note bone size of the proximal and distal phalanges. View Figure 3A
Figure 3A: Axial views of the forefoot that shows the relative size of the second toe compared to other toes with normal surrounding soft tissue. Note bone size of the proximal and distal phalanges. View Figure 3A
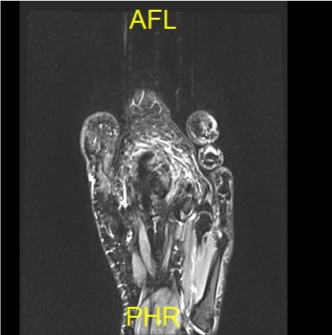 Figure 3B: MRI axial view shows the soft tissue bed of the base of the second toe. Note, wide inter-metatarsal space with normal surrounding fibro-fatty tissue. View Figure 3B
Figure 3B: MRI axial view shows the soft tissue bed of the base of the second toe. Note, wide inter-metatarsal space with normal surrounding fibro-fatty tissue. View Figure 3B
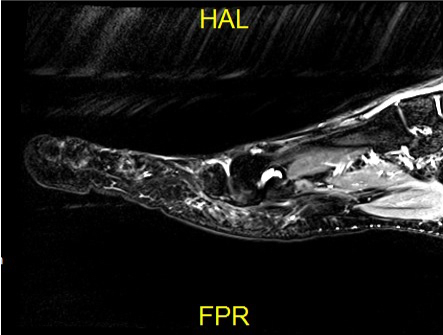 Figure 3C: MRI sagittal view of the fore-foot; second metatarsal and phalanges. It shows normal bony structure and normal cartilage cap with thick fibro-fatty plantar soft tissue. View Figure 3C
Figure 3C: MRI sagittal view of the fore-foot; second metatarsal and phalanges. It shows normal bony structure and normal cartilage cap with thick fibro-fatty plantar soft tissue. View Figure 3C
In order to provide the best treatment for this patient; we reviewed the literatures that discussed this pathology. We realized that most of them are discussing the management in the pediatrics and adolescents which is soft tissue debulking; neither one has reported a surgical technique in this age group.
The patient was given the option of surgical excision of the affected toe with soft tissue reconstruction of the forefoot. All details and expected complications were explained to him and he chooses to proceed for the surgical reconstruction of his forefoot.
The patient underwent a sciatic nerve block with concomitant femoral nerve block in order to allow use of a thigh tourniquet. The patient was positioned supine with a beanbag utilized to support the left lower extremity.
A V-shape incision on the first and second web spaces over the dorsal and plantar aspects of the forefoot were made centered about 5 cm proximal to the base of the second toe resembling an identical triangle (Figure 4A, and Figure 4B). Following identification and retraction of the extensor tendons and the inter-digital nerves in the anterior aspect, the second metatarsal was identified. Meticulous soft tissue dissection to avoid injury of any of the surrounding major structures till complete isolation of the first and third toes extensor and flexor tendons, inter-metatarsals nerves and blood vessels was done. The second metatarsal, extensors and flexors tendons of the second toe were identified successfully and confirmed by intraoperative clinical examination. I identified the inter-metatarsal ligaments between the second and first metatarsal and the second and the third metatarsals. I marked them with number 0 suture before I dissected them just at the medial and lateral edges of the second metatarsal. I realized that this step is very important to re-attach the inter-metatarsal ligaments to approximate the new web space between the first and third metatarsals. Without this step there would be a lot of tension on the soft tissue after resecting the second metatarsal and obtaining soft tissue debulking.
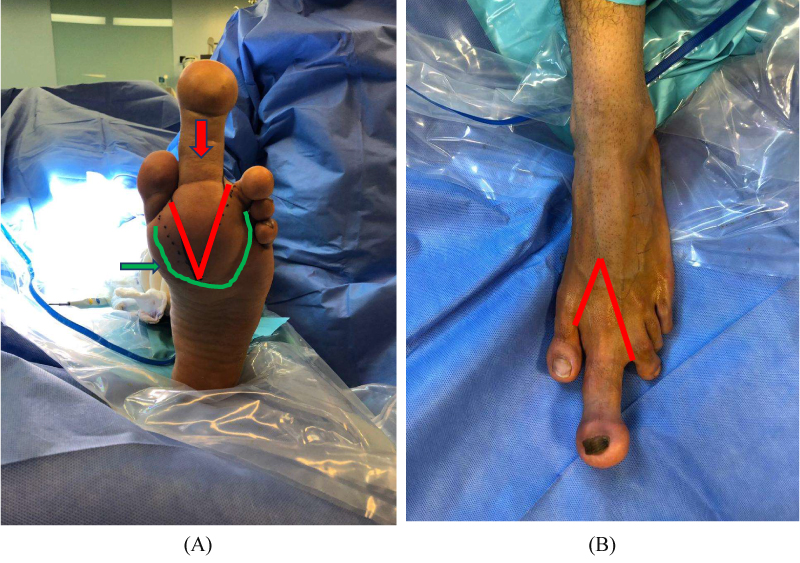 Figure 4: Pre-operative planning photograph showing A) the V-shape incision; plantar and dorsal, for soft tissue resection and amputation; B) c-shaped line that demarcates the fibro-fatty tissue needs internal debulking. View Figure 4
Figure 4: Pre-operative planning photograph showing A) the V-shape incision; plantar and dorsal, for soft tissue resection and amputation; B) c-shaped line that demarcates the fibro-fatty tissue needs internal debulking. View Figure 4
Following anatomic dissection of the soft tissue and isolating the major structures, we chose to perform a short oblique osteotomy of the second metatarsal. Using image intensification, the metatarsal osteotomy was made 2 cm distal the second tarso-metatarsal joint at the mid-foot. The osteotomy was carried out with an oscillating saw under irrigation (Figure 5A and Figure 5B). I decided to keep about 2 cm of the proximal part of the second metatarsal to maintain the Lisfranc ligament attached. This would be important step to maintain the stability of the mid-foot and maintain the foot arch. I used this bony segment later to pass a 3.5 fully threaded screw between the first and remnant segment of the second metatarsal to take the tension off the soft tissue on the proximal aspect of the forefoot despite re-attaching the inter-metatarsal ligaments at the distal part of the forefoot. The flexors and extensors tendons of the second toe were cut at the middle of the second metatarsal in order to reduce the inter-metatarsal soft tissue defect. The skin flaps were left at the toes' edges for re-attachment and final skin closure (Figure 5C).
 Figure 5A&B: A) Amputated soft tissue including distal phalanx, proximal phalanx and distal two third of the second metatarsal; B) The fibrous and fatty tissues well seen in this image. View Figure 5A&B
Figure 5A&B: A) Amputated soft tissue including distal phalanx, proximal phalanx and distal two third of the second metatarsal; B) The fibrous and fatty tissues well seen in this image. View Figure 5A&B
 Figure 5C: Intra-operative image of surgical amputation and soft tissue debulking. Note, the skin flaps were left at the toes' edges for re-attachment and final closure. View Figure 5C
Figure 5C: Intra-operative image of surgical amputation and soft tissue debulking. Note, the skin flaps were left at the toes' edges for re-attachment and final closure. View Figure 5C
I passed a temporary K-wire between the first and third metatarsals before closing the soft tissue and skin. The inter-metatarsal ligaments were re-attached with multiple figure of 8 number 0 sutures to restore forefoot stability. Final fluoroscopy images were performed demonstrating anatomic alignment of the foot with appropriate placement of hardware (Figure 6). Wound closure was performed in our standard fashion with 3-0 absorbable monofilament for the subcutaneous tissue and 3-0 nylon for the skin (Figure 7A and Figure 7B). The patient was placed in a well-padded splint in a neutral position following application of a sterile dressing.
 Figure 6: Intra-operative fluoroscopy images demonstrating anatomic alignment of the foot with appropriate placement of hardware to take the tension of the soft tissue. View Figure 6
Figure 6: Intra-operative fluoroscopy images demonstrating anatomic alignment of the foot with appropriate placement of hardware to take the tension of the soft tissue. View Figure 6
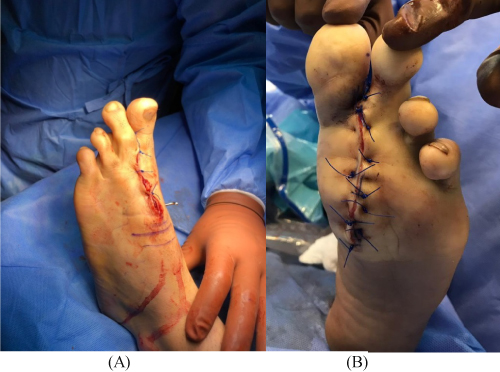 Figure 7: A) Intraoperative images after second toe amputation; B) fore-foot debulking and tentative skin closure. View Figure 7
Figure 7: A) Intraoperative images after second toe amputation; B) fore-foot debulking and tentative skin closure. View Figure 7
The splint and sutures were removed at 2 weeks; we removed this K-wire after 2 weeks when the wound completely healed. The patient was placed in a cast boot and started on active range of motion exercises. The patient was kept non-weight-bearing for 8 weeks and then allowed to bear weight as tolerated in the boot. He was transitioned to a shoe stiffener orthosis at 8 weeks and allowed to return to regular daily activities at 12 weeks, excluding impact activity, until 18 weeks postoperatively. Follow up images at 6 months post operation are included (Figure 8).
 Figure 8: Follow up 6 months after surgery with full weight bearing. View Figure 8
Figure 8: Follow up 6 months after surgery with full weight bearing. View Figure 8
Macrodystrophia lipomatosa (MDL) was first discovered by Feriz in 1925, who described it as a rare non-hereditary localized congenital gigantism. Which has become widely known as a disorder of excessive growth of mesenchymal tissue with disproportionate increase in the amount of fibro-fatty tissue involving single, multiple digits or the entire limb resulting in gigantism [2,3]. Corresponding to the median nerve and medial plantar nerve distribution in the upper and lower limbs, the second and third digits of the hands and feet are most frequently involved, respectively [4].
Usually it presents at birth, causing a problem as the child grows [2].
Patients are usually present with mechanical and functional impairment, such as difficulty in walking or grasping. Which may interfere with their daily activities, social interaction, self confidence in addition to repeated injuries [8]. The Abnormal growth velocity may differ from region to region which continues to grow until puberty at that time it reaches a plateau [4].
The incidence of the condition is unknown due to rarity of this disorder, with an equal male and female ratio [9].
The exact etiology of MDL remains not known. However, multiple hypotheses have been established regarding the etiology of MDL (Abnormalities of the fetal circulation, errors of the intrauterine segmentation, hypertrophy of the involved nerves) [3]. But in this case no link to the mentioned conditions could be established. The diagnosis of MDL is made through clinical presentation, radiographic evaluation and eventually can be confirmed on histopathological examination [3]. However, radiographic examination alone might be sufficient to diagnose MDL. The typical Radiological examination of MDL showed radiolucent areas with an excessive growth of soft tissue as well as osseous tissue [10,11].
Surgical treatment remains a mainstay in the management of MDL. The patients usually seek medical intervention for cosmetic appearance and symmetrical reasonable shoes sizes and appearance [12]. There is no agreed on treatment algorithm for this cases; however, we suggest complete surgical excision of the toe and surrounding soft tissue and resection of the second metatarsal rather than multiple debulking procedures.
It has been reported that recurrence rate is 33%-60% which has been seen following surgical treatment.
Macrodystrophia lipomatosa is a rare form of congenital localized or generalized gigantism. The surgical correction is intended to preserving the normal function in addition to provide an acceptable cosmetic appearance in order to ensure social integration of the patient.
In our case, we reached a favorable outcome with no significant complications in terms of functional recovery and aesthetic results complete surgical excision of the toe and surrounding soft tissue and resection of the second metatarsal.