Multiple mononeuropathy is not unusual in Churg-Strauss Syndrome. Presenting symptoms may be subacute and the differential diagnosis became complicated, particularly when neuropathy is the sole manifestation of disease. We report a clinical case of an adult man hospitalized complaining symptoms of subacute neuropathy succes-sively recognized as multiple mononeuropathy. Histological examination of sural nerve showed the evidence of systemic necrotizing vasculitis with eosinophils infiltration, confirming the diagnosis of CSS. Clinical and neuro-physiological findings are discussed.
Churg Strauss Syndrome, Vasculitic neuropathy, Mononeuritis multiplex, Systemic vasculitides, Eosinophilia
Churg Strauss Syndrome (CSS) constitutes with Wegner's granulomatosis and microscopic polyangiitis, a group of small vessel systemic vasculitides involving venules, capillaries and arterioles [1-3]. Diagnosis is suspected in presence of asthma, purpura, mononeuritis multiplex, cardiomyopathy or pulmonary infiltrates and more rarely a rapidly progressive glomerulonephritis or diffuse alveolar haemorrhage [4]. In CSS eosinophilia is common (> 1000/mmc) frequently associated with serum antineutrophil cytoplasm antibody (ANCA) (35-40%) [1]. Histopathology shows granulomatous response in vessels walls, in perivascular and in extravascular tissues with necroziting vasculitis and tissue eosinophil infiltration [5]. Complete remission after corticosteroid and immunosuppressive drugs treatment is frequent, even if relapses may occur in 25% of cases [3]. Subacute neuropathy may precede the general involvement, the clinical suspicion in the acute phase is thus fundamental to direct the correct diagnostic pathway.
A 68-year-old man previously healthy man with history of mild bronchial asthma was hospitalized complaining since three days diffuse muscular pain, paresthesias at inferior limbs with rapid extension in few days to superior limbs with and hands hyposthenia. Neurological examination revealed on the right upper limb a diffuse hyposthenia with areflexia, whereas the left superior limb was normal. Feet dorsiflexion was impaired with severe steppage gait and distal areflexia. Multiplex monononeuropathy was therefore suspected. Electroneurography-electromiography (ENG-EMG) investigation showed diffuse presence of A waves from tibial nerve bilaterally, severe acute denervation activity from the both anterior tibial muscles, normal F ratio, normal findings in both superior limbs.
Routine laboratory tests evidenced leukocytosis (15.100/mmc), with marked increased of eosinophils (7.960/mmc) that represented 52.8% of total white blood cells. CPR was 5.7 mg/dl -n.v.0.8 mg/dl), autoantibodies examination resulted completely normal including c-ANCA (0.4; normal value < 2) and p-ANCA (0.3; normal value < 6). Lumbar puncture showed normal findings. Computed tomography of paranasal sinuses showed hypertrophy of right inferior turbinate with flogosis. Bone marrow biopsy was performed, revealing 30% eosinophilis of the total cells. FIP1L1-PDGFRa analysis in order to exclude an idiopathic eosinophilia syndrome resulted normal. Sural nerve biopsy showed focal severe axonal degenerations and eosinophilic necrotizing vasculitis of a small epineurial artery (Figure 1 and Figure 2) confirming the diagnosis. The patient was treated with prednisone 100 mg/die and he referred progressive improvement of weakness. The following neurological examinations confirmed the presence of diffuse severe distal muscular atrophy more prominent in the upper limbs particularly in the right side mainly involving the intrinsic musculature of hands (4/5 rated according to Medical Research Council) with also bilateral hyposthenia of foot dorsiflexion (4/5) and eversion (4/5 bilaterally), and steppage of gait. Diffuse tendon areflexia persisted. Mild sensory deficits are clearly defined only in the superficial peroneal nerve distribution at feet associated with bilateral legs hypopallesthesia. ENG still showed a severe axonal sensory motor neuropathy sparing only the left ulnar and radial nerve (Table 1) (Figure 3). An immunosuppressive treatment was proposed initially with corticosteroids (prednisone 100 mg/day) then cyclophosphamide 100 mg/die first and finally with azathioprine 100 mg/die.
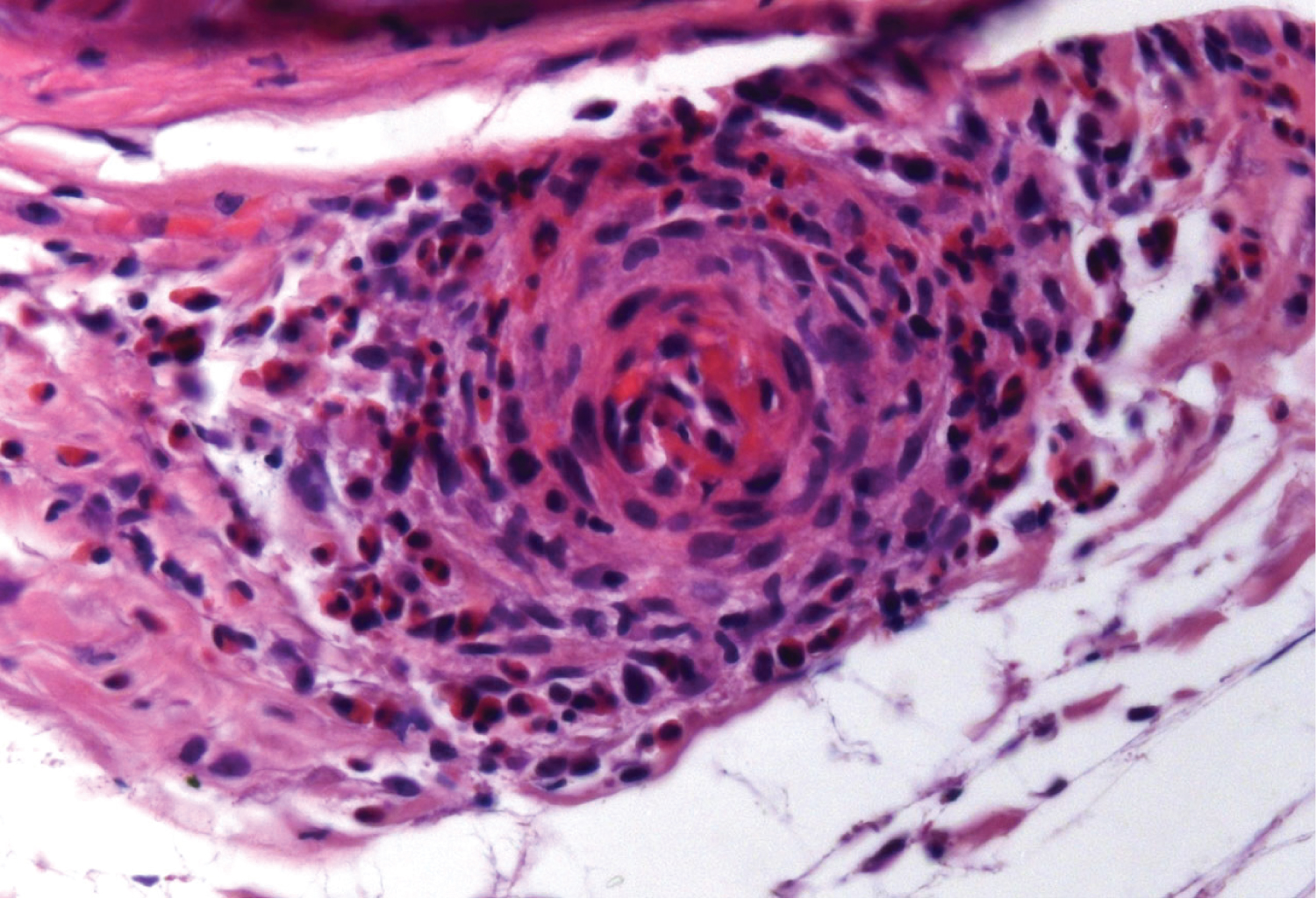 Figure 1: Necrotizing vasculitis of epineurial vessel wall with eosinophil infiltration (sural nerve biopsy, paraffin section, H-E stain).
View Figure 1
Figure 1: Necrotizing vasculitis of epineurial vessel wall with eosinophil infiltration (sural nerve biopsy, paraffin section, H-E stain).
View Figure 1
 Figure 2: Fascicles of sural nerve with focal loss of fibers and axonal degeneration (semithin section, Toluidin Blue stain.
View Figure 2
Figure 2: Fascicles of sural nerve with focal loss of fibers and axonal degeneration (semithin section, Toluidin Blue stain.
View Figure 2
 Figure 3: F waves from right and left tibial nerves with evidence of A waves.
View Figure 3
Figure 3: F waves from right and left tibial nerves with evidence of A waves.
View Figure 3
Table 1: Motor nerve conduction velocity and Sensory nerve conduction velocity. View Table 1
Multiplex mononeuritisis as acute neuropathy resembling Guillain Barre syndrome [6-8], may be the initial symptom of CSS, usually evolving in a distal sensorimotor polyneuropathy [5,9,10]. Cranial nerves neuropathy is uncommon [8]. Studies of biopsied sural nerves indicate axonal degeneration as the major pathological process. Neurological symptoms can improve, but the sequelae of axonal damage may become persistent [8].
The clinical suspicion permits to correctly steer the diagnostic pathway particularly when the internistic disease is not so clear expressed, hence influencing the precocious immunosuppressive treatment crucial to limit the axonal damage responsible of the ultimate clinical sequalae.
Nil.
The authors declare that they have no conflict of interest.
Informed consent was obtained from all individual participants included in the study.
The authors declare that they acted in accordance with ethical standards laid down in the 1964 Declaration of Helsinki.