Severe Acute Respiratory Syndrome corona virus-2 (SARS-CoV-2) also known as COVID-19 primarily affects the respiratory system. There are however atypical presentations that involve other systems. This report aims to highlight the clinical features of a patient who presented to the eye clinic with complaints of blurry vision and binocular diplopia. Ocular examination unaided distant visual acuity was 6/6 in the right eye and 6/4 in the left eye. The near visual acuity was N5 in each eye at 33 cm. Ocular motility showed right esotropia of about 60 prism diopters due to an isolated right abducens nerve palsy and unexplained bilateral disc edema. Investigations for a suspected optic neuritis were carried out. Due to his bizarre symptoms, a nasopharyngeal swap was also taken for SARS-CoV-2 polymerase chain reaction. The COVID-19 test came out positive and the other test results were essentially normal. The patient subsequently developed rashes one week after a diagnosis of COVID-19 was made. A brain magnetic resonance imaging (MRI) performed in the fifth week showed features of small vessel ischemia. The patient was seen fortnightly during the follow up period. His vital signs, oxygen saturation, visual acuity testing, OCT and skin examination were performed and the signs and symptoms resolved in the order of their onset over a three month period without any medications for COVID-19. An informed consent was obtained from the patient and ethical approval was gotten from the Health Research Ethics Committee (HREC) of the hospital following the tenets of the Helsinki on studies involving human subjects.
Abducens Nerve Palsy, COVID-19, Optic Disc Edema, Diplopia, Rashes
Severe acute respiratory syndrome corona virus-2 (SARS-CoV-2) is a 29,903 bp single-stranded RNA (ss-RNA) coronavirus that causes a SARS-like coronavirus infection. This infection was first reported in Wuhan China in December 2019. It spreads rapidly and attained the status of a global pandemic in less than six months. This infection shares similarities with severe acute respiratory syndrome (SARS-CoV) and Middle East respiratory syndrome coronavirus MERS-CoV, so it is possible that the trio share a similar mechanism of infection. Studies suggest that widespread deregulation of homeostasis involving the pulmonary, renal, cardiac, and circulatory systems account for the morbidity and mortality seen in COVID-19. Pseudo-frost bites, hives, maculopapular rashes, urticarial lesions, vesicles and pustules have also been reported in patients with SARS-CoV-2 in patients who have or do not have respiratory symptoms. Recent reports have found that blurred vision, dry eye, and conjunctival injection occurred commonly in patient that developed rashes. About 0.2% of the patients with COVID-19 reported from China had petechial rashes. This was also reported by Beuy to be seen in the majority of patients in Thailand and these patients were misdiagnosed as having dengue fever [1-5]. Another report obtained from Spain after the examination of 375 patients with COVID-19 described the common presentations as maculopapular (47%) with some macular papules described as perifollicular and some described as infiltrated papules [6]. Other common presentations described in this study included urticarial lesions (19%) and pseudo-chilblain lesions. Pseudo-chilblain was a common presentation in the younger age group while maculopapular lesions were seen in the middle age group. Maculopapular lesions were also reported to last for a mean of 8.6 days and may either be pruritic (especially when associated with urticarial forms) or non-pruritic [7]. Loss of the sense of taste and smell has also been reported. Although there has been no direct relationship between SARS-CoV-2 and the eyes, studies have shown the presence of the virus in the ocular secretions of humans and non-human primates presenting with SARS-CoV-2. The ocular features of COVID-19 include: ptosis, ophthalmoplegia, conjunctivitis, dry eyes, retinitis and optic neuritis. The mechanism of invasion of the central nervous system by COVID-19 has not been fully understood. Research suggests that it could be either due to a direct viral tissue invasion, or an indirect auto inflammatory or autoimmune process [6-11]. It is postulated that angiotensin-converting enzyme-2 ACE2 receptors in glial cells and neurons make neuronal tissues a target for COVID-19 [1,2]. These receptors are also found on lung parenchyma, vascular endothelium, kidney cells, and small intestinal cells [2]. The expression of ACE2 receptors is also seen in ocular surfaces such as the conjunctiva and cornea which makes the eye a potential site for the transmission of SARS-CoV-2 [4]. The virus attaches to the cell membrane by the use of a spike protein- S1. This spike protein is similar for SARS-CoV and SARS-CoV-2 but has a 10-20 times higher affinity for ACE2 in COVID-19. Animal studies have shown the spread of the virus from the respiratory tract through the olfactory epithelium into the brain, leading to brain death. The role of the blood-brain barrier in the spread of the virus needs to be explored as evidence from animal studies has shown the presence of the virus in cerebrospinal fluid and neuronal death in the absence of encephalitis [1,8]. An observational case series of 214 hospitalized patients with a laboratory-confirmed diagnosis of severe COVID-19 in Wuhan China, grouped the main neurological manifestations into three: Central nervous system (CNS); dizziness (16.8%) and headache (13.1%), peripheral nervous system (PNS) (8.9%), and skeletal muscle injury (10.7%). An elaboration of the CNS manifestations showed that the most common reported symptoms were dizziness (16.8%) and headache (13.1%). Among patients manifesting PNS symptoms, the most common reported symptoms were aguesia (5.6%) and anosmia (5.1%). In children, abducens nerve palsy has been associated with viral infections and immunization [12,13] and cases of ophthalmoplegia in the setting of COVID-19 have been reported [8-11].
A 37-year-old man who presented with a five-week history of headache and malaise. A week after the onset of these symptoms, he noticed blurry vision in the right eye, binocular horizontal diplopia, and a reduction in color perception. The headache was worse after taking alcohol and relieved with over-the-counter analgesics. There was no history of pain with eye movement, scalp pain, drooping of the eyelids, facial weakness, hearing loss, numbness, insomnia, anosmia, ageusia, muscle weakness or gait abnormality, tingling sensation, and hearing loss. He had no history of head or ocular injury, fever, vomiting, diarrhea, cough, difficulty in breathing, weight loss, rhinitis, and allergies. He was not on treatment for any chronic conditions such as diabetes mellitus, hypertension, and acquired immunodeficiency syndrome (AIDS). He was also not on any over-the-counter medications or drug supplements. On physical examination, he was in no obvious distress sitting with a compensatory head tilt to the left. Vital signs showed the following: Temperature- 36.5 ℃, pulse-rate of 83 b/m, respiratory rate of 20 cycles/min and blood pressure of 172/97 mmHg. Oxygen saturation was 98%. Anthropometric measurements showed a height of 1.77m and weight of 110 kg (BMI-38 kg/m2). On ocular examination, unaided distant visual acuity was 6/6 in the right eye and 6/4 in the left eye. The near visual acuity was N5 in each eye. Ocular motility showed right esotropia of about 60 prism diopters, see (Figure 1). Mydriacyl bottle test showed red desaturation in the right eye. Anterior segment examination was normal and pupils were round and reactive to light. Intraocular pressure was 16/18 mmHg (Goldman). Optical coherence tomography showed bilateral optic disc edema, see (Figure 2 and Figure 3). The differential diagnoses that were entertained include: Space-occupying lesion, hypertensive retinopathy, multiple sclerosis, optic neuritis, idiopathic intracranial hypertension, and COVID-19. The consideration for COVID-19 was with reluctance. An oropharyngeal swab for a qualitative real-time reverse- transcriptase–polymerase-chain-reaction test (rRT-PCR) was taken. Blood samples were taken for the following investigations: Complete blood count, lipid profile, ESR, VDRL, C-reactive protein, ANA, Hepatitis-B screening, HIV, Serum electrolytes urea, and creatinine. Other investigations included resting ECG and urinalysis. He tested positive to COVID-19 and after one week, he developed skin colored papules that were perifollicular, non-itchy and widely distributed over the trunk. An impression of COVID-19 induced folliculitis was made. He described them to be mildly prutitic. A repeat test (rRT-PCR) for COVID-19 after three weeks came out negative. At week 8, he was reviewed and had a resolution of the esotropia, bilateral disc edema and the rash was observed to be healing with some hyperpigmented macules and papules, which are features of a post-inflammatory rash, see Figure 4B. A repeat of the MRI was scheduled to be carried out at three months but the patient was not able to visit the clinic for follow up due to financial constraints. He was however contacted on the phone and he confirmed that the skin rashes had resolved and he had no other symptoms.
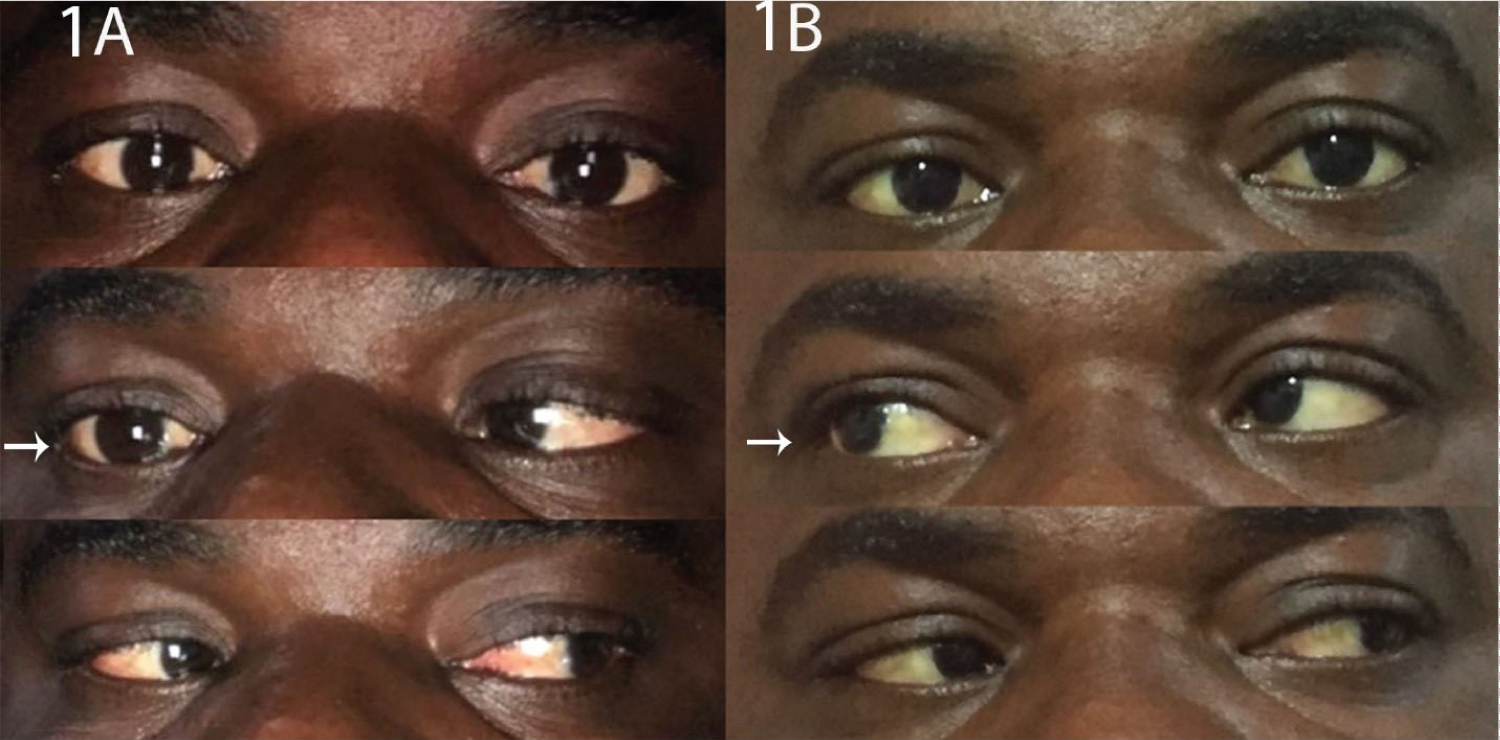 Figure 1: Pane 1A shows abdction deficit of the right lateral rectus muscle due to abducens nerve palsy at presentation. This is indicated by the white arrow while pane 1B shows resolution of the deficit at week eight.
View Figure 1
Figure 1: Pane 1A shows abdction deficit of the right lateral rectus muscle due to abducens nerve palsy at presentation. This is indicated by the white arrow while pane 1B shows resolution of the deficit at week eight.
View Figure 1
 Figure 2: Panes 2A1 and 2A2 show the colour and red free fundus phtographs of the right and left eye respectively taken at week one while 2B1 and 2B2 show the images taken at week eight. The optic disc is indicated by white arrows. The margins of the optic disc were blurred in week one due to edema but were more distinct at week eight. The disc edema was due to an inflammation of the optic discs caused by COVID-19 infection.
View Figure 2
Figure 2: Panes 2A1 and 2A2 show the colour and red free fundus phtographs of the right and left eye respectively taken at week one while 2B1 and 2B2 show the images taken at week eight. The optic disc is indicated by white arrows. The margins of the optic disc were blurred in week one due to edema but were more distinct at week eight. The disc edema was due to an inflammation of the optic discs caused by COVID-19 infection.
View Figure 2
 Figure 3: Panes 3A and 3B show the optical coherence tomography findings of both eyes at week one and week eight respectively. The RNFL thickness graphs indicated by red arrows, show the lines outside of the green zone for both eyes. The black line represents the right optic disc while the blue line is the left optic disc. The lines of the graph fall within the green zone in both optic discs at week eight. There is also an over estimation of the cup to disc ratio in the right eye at week one, which resolved at week eight, indicated by the green arrow. The disc edema distorted the anatomy of the optic disc which resulted in the erroneous estimation of the cup to disc ratio (CDR) of 0.92 × 0.96 in the right eye. The edema in the left optic disc was less hence the accurate CDR of 0.22 × 0.23. The vessels were of normal volume and caliber bilaterally. The RNFL thickness increased at week one and was within normal range in week eight bilaterally, this is indicated by yellow arrows. The macula appeared normal over the study period.
View Figure 3
Figure 3: Panes 3A and 3B show the optical coherence tomography findings of both eyes at week one and week eight respectively. The RNFL thickness graphs indicated by red arrows, show the lines outside of the green zone for both eyes. The black line represents the right optic disc while the blue line is the left optic disc. The lines of the graph fall within the green zone in both optic discs at week eight. There is also an over estimation of the cup to disc ratio in the right eye at week one, which resolved at week eight, indicated by the green arrow. The disc edema distorted the anatomy of the optic disc which resulted in the erroneous estimation of the cup to disc ratio (CDR) of 0.92 × 0.96 in the right eye. The edema in the left optic disc was less hence the accurate CDR of 0.22 × 0.23. The vessels were of normal volume and caliber bilaterally. The RNFL thickness increased at week one and was within normal range in week eight bilaterally, this is indicated by yellow arrows. The macula appeared normal over the study period.
View Figure 3
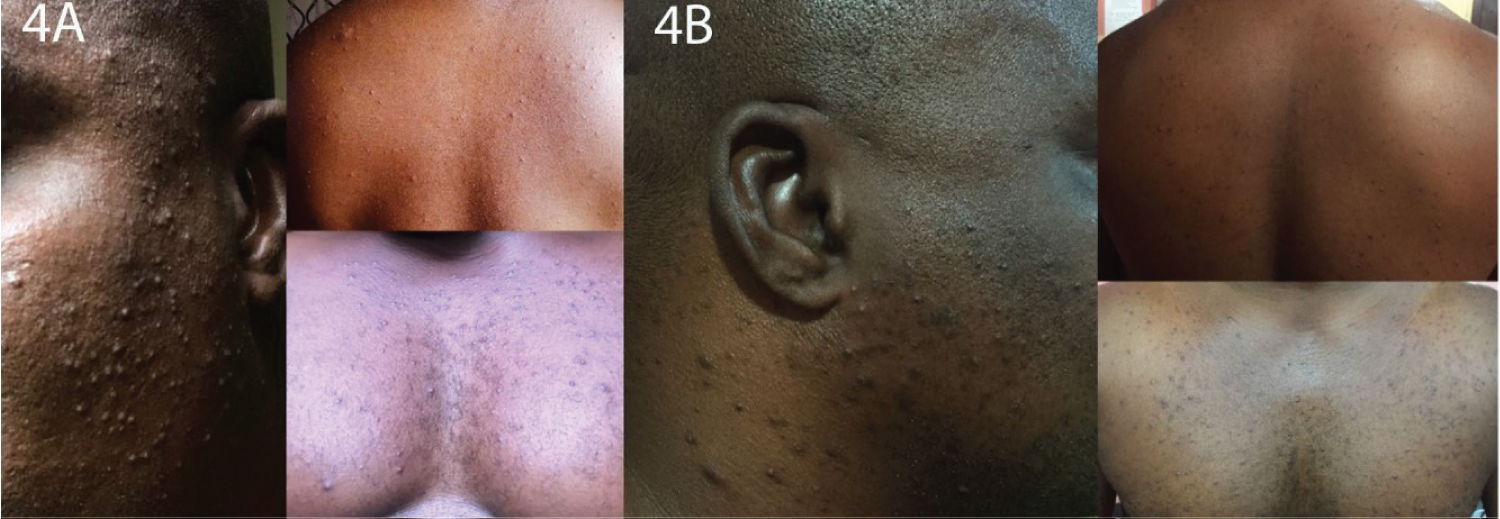 Figure 4: Panes 4A and 4B show skin rashes on the upper back, the chest and malar regions at week one and week eight respectively.
View Figure 4
Figure 4: Panes 4A and 4B show skin rashes on the upper back, the chest and malar regions at week one and week eight respectively.
View Figure 4
Optical coherence tomography showed bilateral thickening of the retinal and blurring of the disc margins consistent with optic disc edema. The disc edema distorted the anatomy of the optic disc which resulted in the erroneous estimation of the cup to disc ratio (CDR) of 0.92 × 0.96 in the right eye, see (Figure 3A). The edema in the left optic disc was less hence the accurate CDR of 0.22 × 0.23. The vessels were of normal volume and caliber bilaterally. Full blood count showed relative lymphocytosis and lipid profile showed dyslipidemia with an elevated total cholesterol of 248 mg/dl and low density lipoproteins (LDL) of 170 mg/dl, see (Table 1). Magnetic resonance imaging with T2 weighting obtained five weeks after the onset of symptoms showed multiple bilateral and asymmetrical small-sized T2/FLAIR deep white hyperintense lesions, predominantly in the centrum semiovale showing restricted diffusion with relatively high ADC values consistent with small vessel ischemia, see Figure 5.
 Figure 5: Magnetic resonance imaging with T2 weighting obtained five weeks after the onset of symptoms showed multiple bilateral and asymmetrical small sized T2/FLAIR deep white hyperintense lesions, predominantly in the centrum semiovale. These lesions show restricted diffusion with relatively high ADC values- consistent with small vessel ischemia, indicated by the red arrows.
View Figure 5
Figure 5: Magnetic resonance imaging with T2 weighting obtained five weeks after the onset of symptoms showed multiple bilateral and asymmetrical small sized T2/FLAIR deep white hyperintense lesions, predominantly in the centrum semiovale. These lesions show restricted diffusion with relatively high ADC values- consistent with small vessel ischemia, indicated by the red arrows.
View Figure 5
Table 1: The values for investigations. View Table 1
Resting ECG- showed Sinus tachycardia and left axis deviation. Real-time reverse-transcriptase-polymerase-chain-reaction test (rRT-PCR) for COVID-19 was positive. A diagnosis of multi-systemic manifestations of SARS-CoV-2 (COVID-19) infection and hypertension in the young was made. The patient was counseled on his condition and placed on medications for hypertension and dyslipidemia by the family physician. He was advised to self-isolate and report to the hospital if there was any deterioration of his condition. One week after the diagnosis of COVID-19 was made, the blurry vision and diplopia persisted, his vital signs were normal and his saturation was 97% in room air. He developed skin colored papules that were perifollicular, mildly pruritic and widely distributed over the trunk. An impression of COVID-19 induced folliculitis was made, see (Figure 4A).
This patient presented with a myriad of atypical symptoms of COVID-19. Previous reports show that patients may present with neurologic symptoms such as double vision, ptosis, blurry vision, various degrees of visual impairment, dizziness, headache, impaired consciousness, acute cerebrovascular disease, and impairment in smell and taste [10,12,14,]. The commoner symptoms include: Fever, cough, diarrhea, malaise, impairment in smell and taste [11,12]. The clinical findings of abducens nerve palsy, blurry vision, bilateral optic disc, macula edema, and intracranial small vessel ischemia are likely due to a direct invasion of brain tissues by this neurotrophic virus. The optic disc edema may be due to direct invasion of the optic nerves and subsequent disruption of axoplasmic transport. This also suggests a breach of the blood retinal barrier by the virus. It could also be due to a diffuse invasion of the brain parenchyma, the optic nerve is a direct extension of the brain.
The ocular manifestations of COVID-19 include conjunctival injection, blurry vision and dryness [4]. The findings of isolated right abducens nerve palsy in our patient is similar to a case that was described by in a 71-year-old woman with hypertension who presented with a two day history of painless diplopia of the right eye and subsequently found to be positive for COVID-19 [14]. The optic disc of the said patient was however normal on funduscopy unlike in the index patient in whom we found bilateral disc edema. In another report of left abducens nerve palsy in the setting of COVID-19 in a 36-year-old man, atrophy of the lateral rectus muscle was seen on MRI and attributed to infection with COVID-19 [10]. Previous researches have reported that COV viruses can cause severe damage to the structure and function of the nervous system of their hosts. SARS-CoV-2 has been shown to have affinity for neural tissues because of the high levels of ACE-2 enzyme in neural tissues Neurological conditions such as viral encephalitis, cerebrovascular diseases and toxic encephalitis have been found in patients with COVID-19 [13].
The mechanism by which CoVs affect the nervous system can be linked to their direct invasion of the tissues of the system with genetic materials passing through neuronal pathways such as the olfactory bulb, and blood circulation; although, the invasion of the SARS-CoV-2 virus through the blood is rare. High levels of D-dimer were found in patients with the critical SARS-CoV-2 viral infection and thus predisposing them to acute cerebrovascular diseases, this was found in 5.7% in a review of 214 COVID-19 patients carried out in Wuhan, China [13,14]. The multiple bilateral and asymmetrical small-sized T2/FLAIR deep white hyperintense lesions, predominantly in the centrum semiovale were due to a diffuse viral invasion of the brain tissues.
The mechanism of by which CoVs affect the skin is poorly understood. The most commonly reported symptoms are those of maculopapular exanthem, urticarial rashes, petechiae or purpura, chilblain-like acral lesions and erythema multiforme. Rarely, there have been descriptions of perifollicular papules and acral infiltrated papules. This patient presented with perifollicular papules and his symptoms began to resolve in eight days. This is consistent with previous literature that has described the maculopapular and papular lesions to occur during the active phase of the disease and resolve after 5-8 days. The lesions in this patient healed with post-inflammatory hyperpigmentation. The rash did not resemble the characteristic pattern description of the maculopapular rashes described in literature. Its perifollicular pattern was however similar to a sub pattern of maculopapular rash described by Galvan. The distribution of the rash in our patient was however similar to the distribution reported by Recalcati among Italian patients [15]. They found that rashes presented in different forms among eighteen COVID-19 patients in Alcona. The manifestations were described as; erythematous in fourteen patients, wide spread urticaria in three patients, chicken-pox like in one patient. These lesions involved mainly the trunk and are similar to the presentation in our patient. Estébanez, also found confluent erythematous-yellowish papules skin lesions that involved the heels [5]. Rashes in COVID-19 patients were also found to persist even after such patients tested negative to the rtPCRT. Our findings were similar to those observed in Spain by Fernandez-Nieto, et al. They found that skin lesions manifested as a late presentation in COVID-19 patients. In testing these subjects for COVID-19, only 2 out of 11 patients tested positive [16]. The symptoms resolved in our patient over the study period. He was not placed on any medication for COVID-19. Our patient may be the second reported case of rash due to COVID-19 in blacks. A case has been previously reported in a South African girl [17].
COVID-19 can present as a multi-systemic disease. In this case; the eyes, brain and skin were affected in an unusual manner which suggests that the full range of the clinical features of the disease is yet to be determined.
Clinicians should look out for extra-pulmonary features of COVID-19, which at present remains a disease in evolution.
The authors are grateful to the management of Lily hospital limited for providing a safe and conducive atmosphere for working and learning. Professor Macdonald Idu proofread this article, we appreciate his masterly guide. We are grateful to Miss Onavwose Princess for providing technical assistance for this work.
No funding or grant support.
There is no conflict of interest to declare.
Ejike Egbu: Conceptualization, Methodology.
Ejike Egbu, Chidi Ihemedu, Ayobami Chioma Olokode, Ugochukwu A. Eze, Onuwaje Mayomi, Chioma Uchendu: Data curation, Writing- Original draft preparation.
Ejike Egbu, Chidi Ihemedu, Onuwaje Mayomi, Sanni-Manuel, Olatayo Francis, Kimoni Ikutegbe: Visualization, Investigation.
Chidi Ihemedu, Chioma Uchendu, Omobamidele Betiku: Supervision and validation.
Precious Uduasobor, Ayobami Chioma Olokode, Ugochukwu A. Eze: Writing- Reviewing and Editing.