To assess central fractional anisotropy changes of the white matter in subjects with spasticity treated with botulin toxin.
Seven subjects with spasticity that developed 2-22 years after cerebrovascular accidents (CVA) were studied with 3T MRI of the brain including diffusion tractography (DTI) and fractional anisotropy (FA) measurements of the white matter of the corticospinal tracts (CST), corpus callosum (CC) and cerebral lobes of the affected and contralateral sides prior and after the injection of botulin toxin at the contours of peripheral nerves of the affected side.
All 7 subjects improved their preexisting spasticity after the injections of botulin toxin. 4 out of 7 showed FA changes post injection in the CST of the affected side. The latter had CVAs occurring 5-15 years prior to the development of spasticity. 3 out of 7 subjects did not show significant FA changes post-treatment. They had CVAs occurring less than 5 years and more than 15 years prior to the development of spasticity. There was regression between 'years of evolution', as a dependent variable, and the square of pre and post injection differences of FA on the contralateral CST, as well as white matter of the parietal and frontal lobes as independent variables.
Botulin toxin injections improved spasticity in all the subjects of our cohort. There also were FA changes in the white matter of the CST of the affected side in those subjects with CVAs happened between 5-15 years prior to the development of spasticity, while those with lesions of less than 5 years and more than 15 years did not show statistically significant FA changes post treatment.
Fractional anisotropy, Spasticity, Botulin, Diffusion tractography, Magnetic resonance imaging
Spasticity is a physiological consequence of damage to nerve cells or their pathways that control muscle movement within the brain or spinal cord. It results in uncontrollable stiffening or straightening of muscles, shock-like contractions of all or part of a group of muscles and abnormal muscle tone which can have harmful effects such as pain, deformity, impaired function and severe disability with costly consequences. In severe cases it requires perineural injections of botulin toxin to alleviate disability and to improve quality of life.
Although the signs and symptoms caused by spasticity that affect activities of daily living are well recognized, the understanding of its causes and when it develops with respect to the time of onset of the neurological lesion are less well understood [1].
It is estimated that around 75% of patients with severe traumatic brain injury, 20% of stroke survivors and 60% of subjects with moderate to severe Multiple Sclerosis require specific spasticity treatment [2].
The neurological lesions of subjects with spasticity can be studied with non-invasive imaging techniques, particularly those related to MRI. Diffusion tractography imaging (DTI) is an advanced magnetic resonance imaging (MRI) tool based on the diffusion of water molecules within cells. In the case of neurons, it helps to image nerve bundles of white matter tracts [3-8]. Furthermore, it also provides quantitative markers such as fractional anisotropy (FA) and Anisotropy diffusion coefficient or Apparent diffusion coefficient (ADC) [9]. In the cerebral white matter, contributions to these indicators come from fibre arrangements, degree of myelination, and axonal integrity [10], and are useful indicators to assess the severity of already known pathological conditions [11-13]. As an indicator of myelin sheath integrity, FA has already been correlated with electrophysiology studies, confirming the technique as particularly sensitive to distal motor latency and sensory nerve conduction velocity changes [14]. FA has been also used as a reliable indicator to evaluate the normalization of neuron structure in white matter lesions after therapy in demyelinating conditions showing neuroprotective effects of some drugs [15], and to assess pathological changes reflecting alteration of neuron integrity in neurodegenerative diseases [16] and traumatic brain injury [17].
ADC measurements for complicated systems as living tissues depend on the diffusion time and weighting used, or b factor, in a given volume unit or voxel. In this study, the diffusion tensor expressed by FA was preferred over ADC as the former reflects the underlying directional diffusion properties of the tissue independently of its orientation in the magnetic field while Te latter is influenced by how the subject has been placed in the scanner magnet and gradient coils [18,19].
The main purpose of this pilot study was to evaluate if there were quantitative changes in the nerve bundles of the central white matter in subjects who developed spasticity after a CVA which could be identified with DTI-FA after the injection of botulin toxin on the affected side.
A secondary purpose of this work was to investigate if there was a relationship between years of evolution after the lesion and FA values in the central white matter.
The Bioethics approval for this study was obtained from the Health Research Authority, NRES Committee South Central-Oxford, in the United Kingdom (13/SC/0561; IRAS 140861). The institutional approval was granted by Research & Development of East Kent Hospitals University NHS Foundation Trust (2013/RADIO/02) and individual subject consents were obtained before the first scan in what concerns imaging aspects of this pilot study. Separate individual consents were obtained by the Department of Neurorehabilitation before the treatment.
The initial cohort included 12 subjects who had developed spasticity due to upper motor neuron lesions. They had single hemispheric post ischaemic or haemorrhagic parenchymal sequelae affecting the gangliocapsular area with extension to the cerebral lobes. The lesions took place within a range from 1 to 25 years before development of a handicapping degree of spasticity requiring peripheral injections of botulin toxin. The subjects were studied with Magnetic Resonance Imaging of the head before and after the treatment.
The spasticity scores were obtained according the Disability Assessment Scale [20] pre and post-injection.
Two subjects were excluded immediately after the initial MRI series for technical reasons (metallic fragments causing inhomogeneity in the magnetic field). The remaining ten were studied with MRI of the brain at a magnetic field strength of 3 Tesla and following a protocol that included localizers, isovolumetric T1, isovolumetric T2, axial and coronal FLAIR, axial Proton Density and T2, axial susceptibility weighted images (SWI) and diffusion tractography series (DTI) with 32 directions (Table 1), before and eight weeks after the peripheral perineural injection of botulin toxin (200 units, diluted in 4 ml of saline solution 9%).
Table 1: MR imaging protocol. View Table 1
Three subjects were excluded after the full initial scan due to poor imaging quality (movement artifacts or inability to complete the imaging protocol). Seven subjects were included and were studied before and after the injections. The obtained images were post processed in an independent workstation using Syngo Via® software to image the corticospinal tracts of the affected and contralateral sides (Figure 1 and Figure 2), the corpus callosum (Figure 3) and the tracts in the white matter of the frontal, parietal, temporal and occipital lobes of the affected and contralateral sides. The seeding points for tractography [21] were placed in the rostral cerebral peduncles on axial plane for the corticospinal tracts, in the corpus callosum on the sagittal plane, and in the white matter of the cerebral lobes within the boundaries set by the Talairach Atlas on axial plane. Fractional anisotropy values were obtained for each of the tracts. Each measurement was repeated three times to ensure consistency.
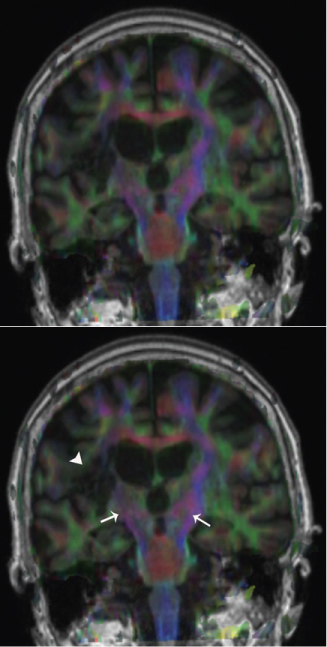 Figure 1: FA maps fused to coronal T1 sectioning rostrally the cerebral peduncles showing CSTs in blue (white arrows). Note the lesion (white arrowhead) on the affected side on the patient's right (left side of the image) and how it extends to the right CST. View Figure 1
Figure 1: FA maps fused to coronal T1 sectioning rostrally the cerebral peduncles showing CSTs in blue (white arrows). Note the lesion (white arrowhead) on the affected side on the patient's right (left side of the image) and how it extends to the right CST. View Figure 1
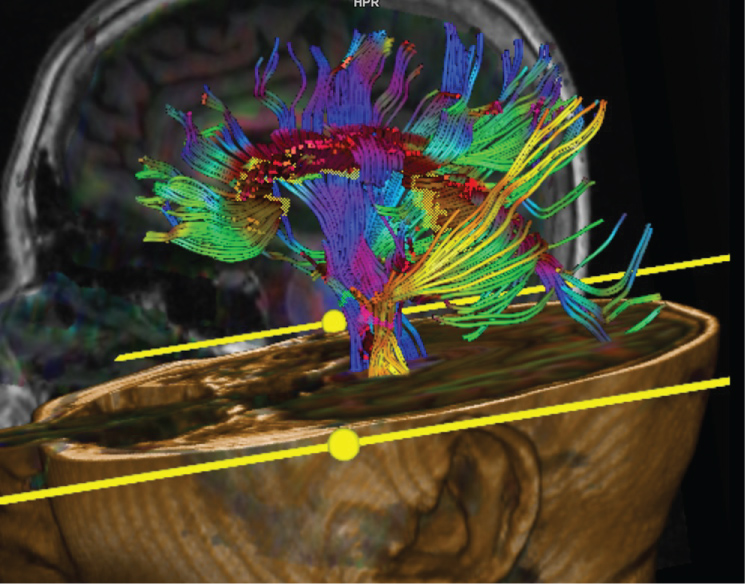 Figure 2: DTI fused to 3D T1 showing CSTs (yellow and blue) and CC (purple). View Figure 2
Figure 2: DTI fused to 3D T1 showing CSTs (yellow and blue) and CC (purple). View Figure 2
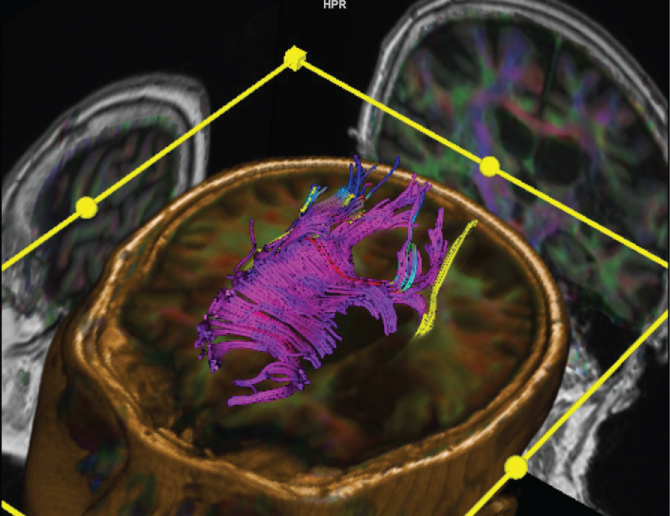 Figure 3: DTI fused to 3D T1 showing CC in purple. Some of its fibres are affected by the lesion on the right side of the patient (and also right side of the photo). View Figure 3
Figure 3: DTI fused to 3D T1 showing CC in purple. Some of its fibres are affected by the lesion on the right side of the patient (and also right side of the photo). View Figure 3
The tabled variables included age, gender, spasticity score, presence of Wallerian degeneration, score of disability assessment scale pre and post injection and fractional anisotropy (FA) values of the corticospinal tracts (CST), corpus callosum (CC), frontal (FL), parietal (PL), temporal (TL) and occipital lobes (OL) of the affected (aff) and contralateral (cont) side. In the case the CC, as a midline structure, there were single pre and post injection measurements.
The square powers of differences between pre and post injection FA values of each measurement were also tabled.
Calculations carried out were basic statistics, potency tests for dependent samples, T-tests for dependent variables and Forward Stepwise Multiple Regression analysis. The latter considered the years elapsed from the onset of the lesion to the development of spasticity as a dependent variable and the transformed variables as independent, for each one of the areas, which included CST, CC, FL, PL, TL and OL of the affected and contralateral sides. All the quantitative variables were plotted in graphs jointly and separately on the y-axis versus years of evolution on the x-axis. The fittings were both linear and least squares in all the graphs. After obtaining the results as shown below, all the FA values were entered multiplied by 1000 (x = FA × 1000) to do the calculations with integer numbers.
The seven subjects in this cohort included 2 males and 5 females, with an average age of 49 years (24-71) and an interval evolution of 10 years (1-25) since the onset of the causative central nervous system lesion. Two had imaging signs of Wallerian degeneration with bright signal on T2 and FLAIR in the CST at the rostral aspect of the cerebral peduncles on the affected side (Table 2).
Table 2: Qualitative variables in the cohort. View Table 2
The degree of spasticity improved in all subjects after the injection of botulin toxin. Their mean spasticity score in the Disability Assessment Scale improved from 2.5 (2-3) previously to the injection to 1 (0-2) post-injection.
Pre-injection mean FA values for CC were 0.448 and on the affected side 0.462 for CST, 0.355 for FL, 0.372 for PL, 0.363 for PL, and 0.388 for OL. Pre-injection FA values on the contralateral side were 0.485 for CST, 0.370 for FL, 0.406 for PL, 0.413 for TL and 0.395 for OL. Post injection FA for CC was 0.457. On the affected side FA was 0.470 for CST, 0.340 for FL, 0.358 for PL, 0.380 for TL and 0.394 for OL. Post-injection FA values for the contralateral side were 0.480 for CST, 0.388 for FL, 0.411 for PL, 0.408 for TL and 0.420 for OL (Table 3).
Table 3: Quantitative variables in the cohort. View Table 3
The mean values of transformed variables were 833 for CC and on the affected side 203 for CST, 972 for FL, 783 for PL, 6302 for TL and 1143 for OL. The mean values of post injection transformed variables on the contralateral side were 647 for CST, 984 for FL, 1112 for PL, 176 for TL and 1954 for OL (Table 4). On (Figure 4) the linear graph shows FA values of affected CST tracts on y-axis versus years of evolution on the x-axis before and after the injection of botulin toxin, with least squares fitting. On (Figure 5) the box graph shows the distribution of FA values of affected CSTs pre and post injection for all 7 subjects.
Table 4: Transformed variables. View Table 4
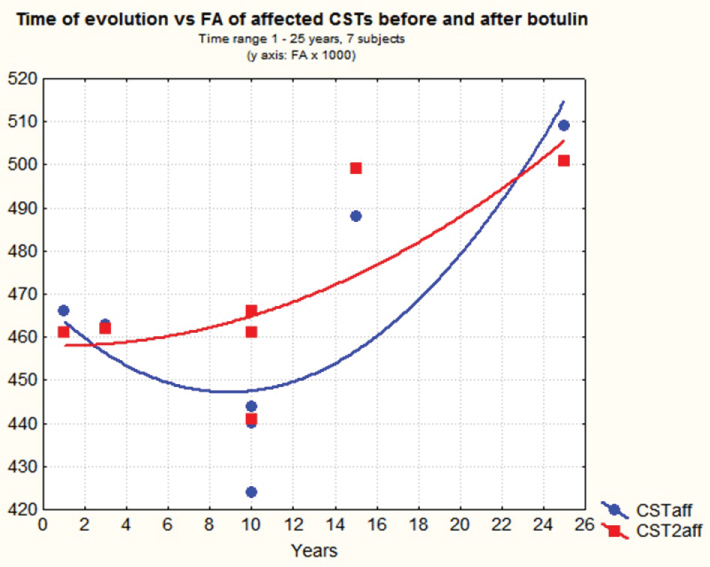 Figure 4: Time of evolution with range 1-25 years on x-axis vs. fractional anisotropy of the affected corticospinal tract before and after the injection of botulin in all 7 subjects. FA has been multiplied by 1000 to convert it into an integer. View Figure 4
Figure 4: Time of evolution with range 1-25 years on x-axis vs. fractional anisotropy of the affected corticospinal tract before and after the injection of botulin in all 7 subjects. FA has been multiplied by 1000 to convert it into an integer. View Figure 4
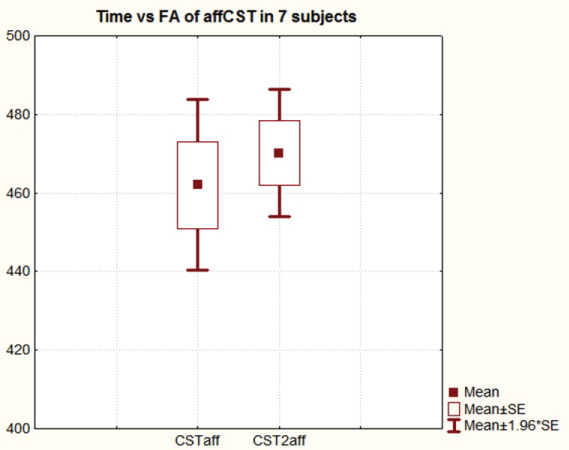 Figure 5: Fractional anisotropy of the affected corticospinal tracts pre and post botulin injection. FA is multiplied by 1000 to convert it into an integer. All 7 subjects were included. Evolution time range 1-25 years. View Figure 5
Figure 5: Fractional anisotropy of the affected corticospinal tracts pre and post botulin injection. FA is multiplied by 1000 to convert it into an integer. All 7 subjects were included. Evolution time range 1-25 years. View Figure 5
The obtained power calculation of two-means T test for dependent samples was 0.81 with an alpha error of 0.05.
T tests for dependent variables, considering the pre and post injection spasticity scores (DAS), were significant (t = 7.07). T tests for dependent variables were not significant when all seven subjects were considered (Table 5), although they became significant when only the subjects with a lesion evolution between 5-15 years were included (4 out of 7 subjects) (Table 6); the subjects with lesions of less than 5 years and more than 15 years of evolution since onset (3 out of 7) were excluded (Figure 6). The latter were carried out after noting maximal FA differences in subjects within that range on graphs that plotted years of evolution on x-axis and pre and post-injection FA values in all four of them on y-axis, while no such changes were depicted for subjects with lesions that happened less than 5 and more than 15 years from the development of spasticity that affects activities of daily living (Figure 4, Figure 5, Figure 6, Figure 7 and Figure 8). Potency tests for dependent samples were again calculated including only the 4 subjects with lesions with an evolution within a range of 5-15 years, showing similar results to those obtained when considering all 7 subjects.
 Figure 6: Fractional anisotropy values of the affected corticospinal tracts in 4 subjects, whose time of evolution after the causing lesion ranged 5-15 years. FA is multiplied by 1000 to convert it into an integer. View Figure 6
Figure 6: Fractional anisotropy values of the affected corticospinal tracts in 4 subjects, whose time of evolution after the causing lesion ranged 5-15 years. FA is multiplied by 1000 to convert it into an integer. View Figure 6
 Figure 7: Evolution time range 1-25 years on x-axis vs. fractional anisotropy values of the affected corticospinal tracts pre and post injection of botulin on y-axis in all 7 subjects. FA values are multiplied by 1000 to convert them into integers. View Figure 7
Figure 7: Evolution time range 1-25 years on x-axis vs. fractional anisotropy values of the affected corticospinal tracts pre and post injection of botulin on y-axis in all 7 subjects. FA values are multiplied by 1000 to convert them into integers. View Figure 7
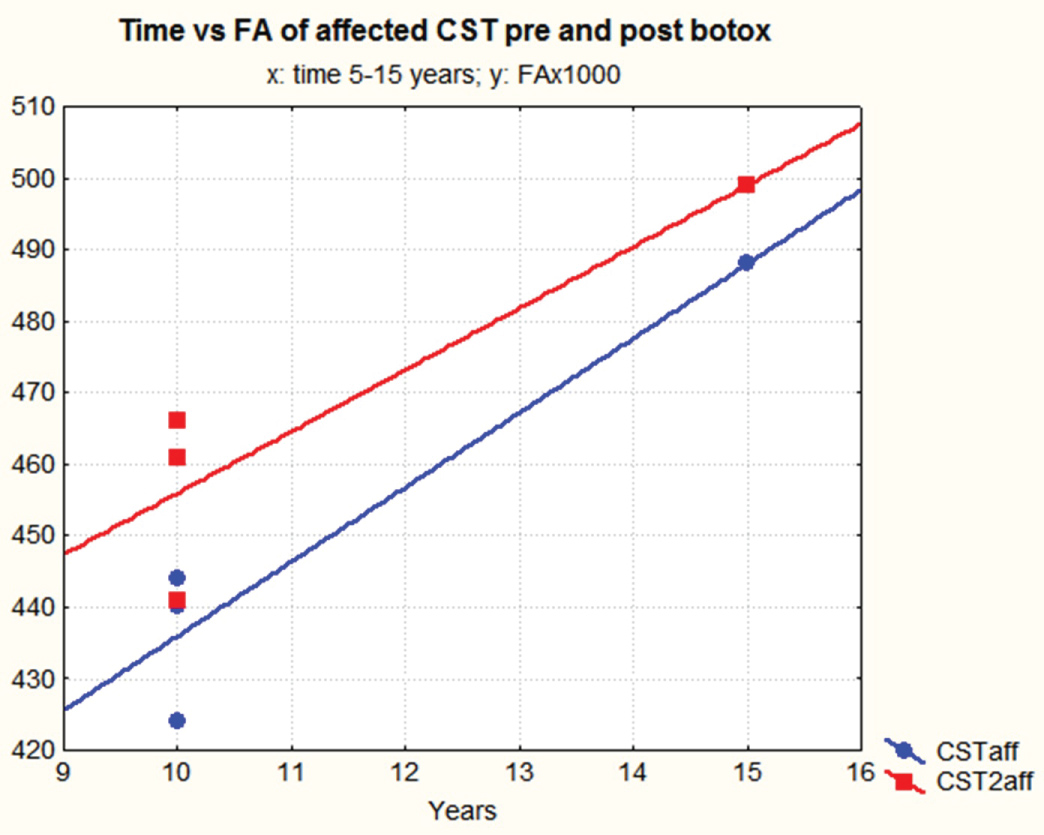 Figure 8: Evolution time range 5-15 years vs. fractional anisotropy values of the affected corticospinal tracts on y-axis, pre and post injection of botulin, in 4 subjects. FA values are multiplied by 1000 to convert them into integers. View Figure 8
Figure 8: Evolution time range 5-15 years vs. fractional anisotropy values of the affected corticospinal tracts on y-axis, pre and post injection of botulin, in 4 subjects. FA values are multiplied by 1000 to convert them into integers. View Figure 8
Table 5: T tests for dependent samples in all 7 subjects, time range 1-25 years since from the causing lesion. View Table 5
Table 6: T tests for dependent samples in 4 subjects with in a time range of 5-15 years from the causing lesion. View Table 6
Multiple regression analyses for 'years' as a dependent variable, and transformed FA differences as independent variables showed the following values: R = 0.92, R2 = 0.84 and adjR2 = 0.69 with F(3,3) = 5.5, p < 0.05 (Table 6).
Spasticity indicates upper motor neuron dysfunction and when it is severe it usually leads to handicapping motion restriction and serious disability [22]. It is a common problem in patients following head trauma and cerebral vascular accident (CVA) [1,23] and may develop shortly after the onset of the initial lesions or several years afterwards.
Depending on its severity, spasticity may be improved by the perineural injection of botulin toxin close to the peripheral nerves controlling the affected muscle groups, mostly to improve quality of life [24] as performed with all the subjects included in this study. Post botulin injection changes may last for a variable period of time [25-27].
For these cases of subjects with handicapping spasticity, the status of white matter tracts were assessed with DTI to obtain not only qualitative assessment of the affected white matter but also a to measure FA as a quantitative indicator of the bundles microstructure [9,10,28]. Changes in this indicator usually predict evolution in acquired brain injuries and neuroinflammatory conditions [4,28,29].
Some authors have reported central changes after peripheral treatments with botulin toxin [30-37]. However, it is unclear why FA changes post injection were identified in the four subjects of our cohort with an evolution that ranged from 5 to 15 years since the initial lesion while the remaining three, with an evolution of less than five years and more than fifteen years, did not show significant changes [38-41]. It has been shown that FA changes occur in given periods of time in linear studies of subjects with Parkinson's disease [42] and hypertonia [43]. It may be hypothesized that microstructural changes related to neuroplasticity are favoured once all the inflammatory changes after the initial lesion are resolved and cease after a given period of time [44-48], as no further tissue repair can take place. Further linear studies with a more extensive cohorts would be required to ascertain it.
Clinically, however, all of the subjects showed clinical improvement of spasticity post injection of botulin toxin [39].
It is accepted that fractional anisotropy values change with age [49-52] and may also vary according to which of the two main measurement procedures is used. One measurement method is based on tracing regions of interest (ROI) in selected areas, as performed to obtain the white matter tracts and their FA in this pilot study. The other method is based on statistical parametric mapping (SPM), which is a more standardized and automated procedure [53]. In our group of subjects, the youngest showed the highest FA values and no significant post injection changes, which may have been influenced by the time of evolution as the lesion occurred in early infancy and more than 20 years had elapsed to the development of the episode of handicapping spasticity considered in this study.
FA values in the subjects of this cohort have decreased with age, as noted then plotting age on x-axis and pre-post injection FA on y-axis (Figure 7).
Additionally, it was unclear why those subjects with imaging signs of Wallerian degeneration in the affected corticospinal tract showed both clinical and FA post injection improvement as it has been found by other authors [54], although there is contradictory evidence in this regard in the literature [55,56].
Direct effects of botulin neurotoxin have been described by some authors [57] suggesting that indirect plasticity of central circuits subsequent to a reduction of sensory input from the injected muscles may be one of the explanations [58-60]. An alternative hypothesis is direct influence of the neurotoxin on central circuits, similar to that seen with tetanus neurotoxin [61,62].
The results of the forward stepwise multiple regression that considered years of evolution as dependent variable and the square of the pre and post injections FA differences for each area, could be due to fractional anisotropy variations related to time elapsed after the lesion, neuroplasticity and influenced by the subjects age (Figure 9 and Figure 10), as the regression did not show significant post injection FA values on the affected side but high correlation (r) and good prediction (r2) values for structures on the contralateral side.
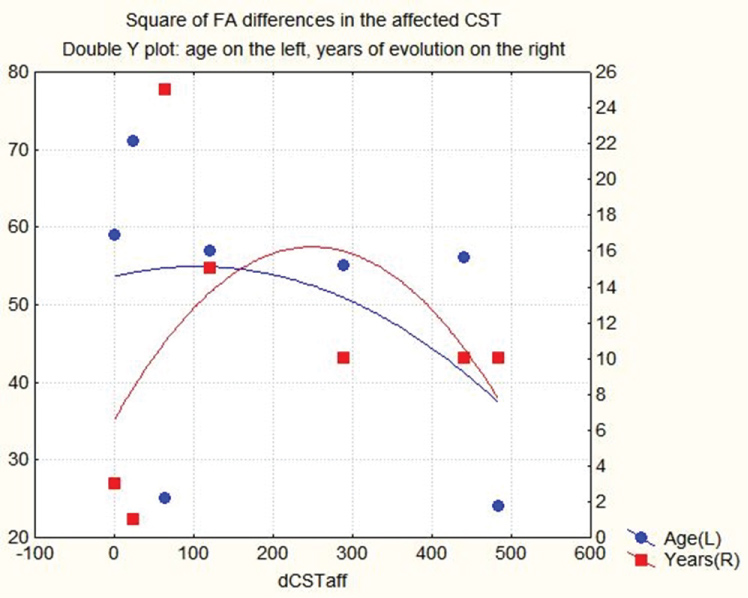 Figure 9: Double y-axis plot of square of the FA differences of the affected CST on x-axis, versus subjects age, on left y-axis, and years of evolution after CVA on right y-axis. (FA values are converted into an integer by multiplying them by 1000). View Figure 9
Figure 9: Double y-axis plot of square of the FA differences of the affected CST on x-axis, versus subjects age, on left y-axis, and years of evolution after CVA on right y-axis. (FA values are converted into an integer by multiplying them by 1000). View Figure 9
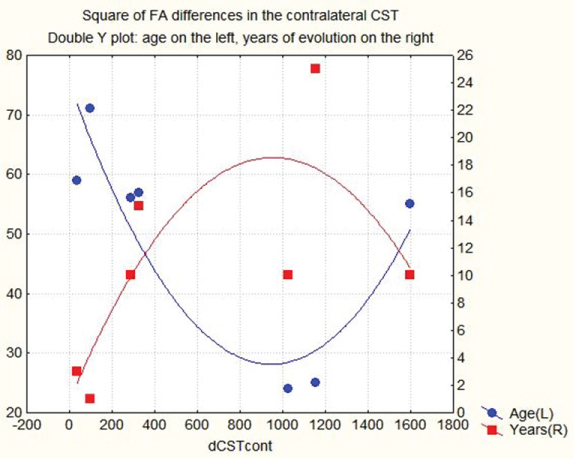 Figure 10: Double y-axis plot of square of the FA differences of the contralateral CST on x-axis, versus subjects age, on left y-axis, and years of evolution after CVA on right y-axis. (FA values are converted into an integer by multiplying them by 1000). View Figure 10
Figure 10: Double y-axis plot of square of the FA differences of the contralateral CST on x-axis, versus subjects age, on left y-axis, and years of evolution after CVA on right y-axis. (FA values are converted into an integer by multiplying them by 1000). View Figure 10
Spasticity that developed in a time range from 2 to 22 years after a CVA improved clinically after the peripheral perineural injections of botulin toxin in all 7 subjects of our cohort.
Additionally, 4 out of 7 subjects with lesions acquired 5 to 15 years prior to the development of spasticity showed statistically significant FA changes in the affected corticospinal tracts after the injections of botulin toxin.
3 subjects with lesions occurred outside that range, i.e. less than 5 and more than 15 years, did not show statistically significant FA variations in the corticospinal tracts of the affected sides.
There was regression between years of evolution as a dependent variable and FA values of the contralateral (non-affected) corticospinal tracts, and white matter of the parietal and frontal lobes of the contralateral side, as independent variables.
Further assessments of a larger cohort of patients should be pursued to confirm these preliminary findings.
The authors wish to express their gratitude to Mark Kerr, Librarian of East Kent Hospitals University NHS Foundation Trust, for his assistance with searches and retrievals of references used throughout this research, and also to both Dr Thomas Webb, Consultant in Stroke Medicine at East Kent Hospitals University NHS Foundation Trust, and Dr. Sofia Bertoni, for their assistance in preparing this manuscript.