Goals of this single-case study are to assess whether tests according to Control Mastery Theory (CMT) can be reliably identified by trained raters and to examine whether the Psychotherapy Process Q-Sort method can adequately represent the test situation.
A single case was analyzed by well-trained psychology graduates on the basis of the Plan Formulation Method. The interrater reliability of the identified tests was examined. In addition, the tests were classified according to the Psychotherapy Process Q-Sort.
70 test situations were identified with acceptable overall interrater reliability and slightly better values for single categories. The Q-Sort analysis indicated 34 items that were assigned more than 5 times to 3 tests. Overall, a combination of more than five Q-Sort items represented one test situation.
These findings demonstrate that even well-trained graduates can identify tests. Indeed, the Psychotherapy Process Q-Sort does not suffice to adequately represent the test concept according to CMT.
Psychotherapy, Control mastery theory, Single case study, Psychotherapy process Q-Sort, Reliability
Control Mastery Theory (CMT) is a cognitive-psychodynamic-relational theory developed by Joseph Weiss, Harold Sampson and the Mount Zion Psychotherapy Research Group [1]. The theory describes and explains the behavior of a patient as well as the therapist's interventions during psychotherapy. The theoretical assumptions are based on Freud's later ideas, particularly on his hypotheses of the unconscious ego and superego [1]. Weiss [1] assumed that people adapt to the environment from their first years of life because attachments to significant others are important for the representation of self and others. Thereby people develop conscious and unconscious constructs of themselves and their environment that are based on their experiences and guide their behavior [2]. According to Weiss [3] these constructs can be dysfunctional because of traumatic experiences. These constructs are called pathogenic beliefs and are the result of the adaptation process, which is typically unconscious. For example, "a young boy who experienced himself as neglected by his parents, developed the pathogenic belief that he would and should be neglected, not only by his parents, but also by others" [4].
Pathogenic beliefs impede the normal development of the child [5]. These beliefs tell the person that if he or she wants to achieve a certain realistic and reasonable goal, that person will endanger him-or herself or loved others. Pathogenic beliefs are developed in early childhood within the relationships with significant others (e.g., parents) upon which the child depends for survival. Thus, every threat to this relationship is traumatic for the child.
Traumatic events can be classified into shock trauma and stress trauma. Shock trauma is defined as a severe traumatic event, such as the illness or death of a parent. The child may feel responsible for the death or disease; the child may think that a certain wish or behavior caused this event. For example, a child who is hostile to his parent before the parent's unforeseen death may assume that his hostility caused the parent's death. This pathogenic belief can be permanent because the consequence was so dramatic and traumatic [1].
Stress trauma occurs if the child thinks that a certain wish or goal endangers his relationship with his parents. The child then avoids this wish or goal and develops a pathogenic belief, for example, "It is dangerous to become independent". Children often feel responsible for everything that occurs. They think they deserve the trauma and therefore tend to repeat the traumatic situation even if it causes the child to suffer [1]. Pathogenic beliefs often influence a person's control over his unconscious mental life. Such beliefs are a powerful source of motivation that can lead people to behave against their conscious will to avoid danger. However, a pathogenic belief is constricting and inhibiting and is accompanied by feelings of shame, guilt and anxiety. Thus, people are highly motivated to overcome their pathogenic beliefs [1].
Patients who enter psychotherapy are seeking help to disconfirm their pathogenic beliefs [6]. Weiss [3], Silberschatz [7] and Curtis and Silberschatz [8] developed the plan concept that describes how patients pursue an unconscious plan for seeking help to solve and master their problems and disconfirm their pathogenic beliefs. There are three methods with which to disconfirm pathogenic beliefs: (1) Developing insight, (2) Using the therapeutic relationship or (3) Directly testing with the therapist [6].
Tests are experimental actions that the patient uses to verify the validity of his pathogenic beliefs. He unconsciously hopes that the therapist will act in a manner that disconfirms those beliefs, allowing the patient to develop a healthier or an alternative behavior. In a test situation, the patient acts according to his pathogenic belief, which tells the patient that his behavior will endanger his relationship with the therapist. If the therapist is not affected by this behavior, the patient becomes less anxious and can take a step toward disconfirming his pathogenic belief because the belief becomes more conscious and some repressions can be lifted. However, if the therapist is affected by the patient's behavior and confirms the pathogenic belief, the patient becomes more anxious and constricted [1].
Weiss [1] differentiated between transference tests and passive-into-active tests. In a transference test, the patient attempts to determine whether the therapist will cause trauma as his parents or significant others did. In this test, the therapist assumes the role of the parents. For example, a patient who was often criticized by his parents will manifest behavior in therapy that the patient assumes will lead the therapist to criticize him, e.g., being late for the sessions. Turning passive into active tests, the patient assumes the role of the parents and behaves in a traumatizing manner toward the therapist. The patient described above, for example, may criticize the therapist for his high fee or his unhelpful treatment. Both types of tests repeat the patient's traumatizing experiences with his parents. Both behaviors are strategies of defense and simultaneously strategies to overcome the problem. If the therapist reacts in a manner that helps the patient to disconfirm his pathogenic belief, the therapist passes the test and his behavior is called pro-plan. If the therapist's reaction confirms the belief, the behavior is anti-plan [1].
Generally, patients are testing more or less continuously during therapy, using minor and major tests. Several studies provide evidence that a high rate of passing tests is directly associated with better outcomes compared with a high rate of failing tests [9-11]. Silberschatz and Curtis [10] demonstrated that therapeutic interventions, which are pro-plan and disconfirm the patient's pathogenic beliefs, lead to immediate improvement for the patient. Silberschatz [10] observed a similar result: if the therapist passed a test, the patient became less anxious and more friendly and relaxed. Sammet, et al. [9] observed a higher level of insight with good pro-plan interventions.
Although these studies confirm the hypotheses of CMT, there has been relatively little direct empirical evidence for the reliability of Weiss's [3] test concept until now. Silberschatz and Curtis [11] examined the interrater reliability of five independent raters in the identification of two patients' tests. The analysis showed good reliability of r(k) = 0.50 and r(k) = 0.75 (3). Another analysis of the interrater reliability of the identification of tests was demonstrated by Silberschatz [10]. Nine graduate students analyzed verbal transcriptions of 100 psychotherapy sessions of a patient and identified test sequences. Subsequently, three psychoanalytically skilled raters identified key tests, observing 46 central test sequences with a very good reliability of rkk = 0.82 (rll = 0.63) [10].
A method to analyze the patient's plan is the Plan Formulation Method developed by the Mount Zion Psychotherapy Research Group [12]. According to Caston [13], the patient's plan is a complex psychoanalytic formulation that describes the problem the patient wants to solve consciously or unconsciously. The method contains (1) Goals, (2) Traumatic experiences, (3) Obstructions, (4) Tests and (5) Insights of the patient. Goals are healthy and natural thoughts, feelings and behavior that the patient abandoned because of his unconscious pathogenic beliefs. However, the patient unconsciously suffers from not being able to realize those reasonable goals and is motivated to acquire healthy behavior. CMT assumes that all goals are healthy; unhealthy thoughts, feelings and behavior are always consequences of pathogenic beliefs. Goals are often unconscious because the pathogenic beliefs cause the goals to remain unconscious [2]. Obstructions constrain the patient from pursuing his goals. According to Rappoport [2], obstructions comprise two elements: the key trauma and the pathogenic belief. To overcome his obstructions, the patient uses tests and insights. Insight is the patient's awareness of the nature and cause of his problems. Often, but not necessarily, awareness arises after an interpretation of the therapist, when the patient feels [2]. Developing such a plan for the patient can help the therapist react to the patient's tests in a pro-plan manner.
A central topic of CMT is the relationship between patient and therapist during the therapy process. Another manner in which to understand the interaction between therapist and patient is the Psychotherapy Process Q-Sort [14].
Jones [14] determined that in the course of psychotherapeutic treatment, certain interaction structures between patient and therapist recur. Changes in these interaction structures relate to changes in the patient's symptoms and his psychological structure. According to Jones [14], the therapist influences the patient and the patient influences the therapist. An instrument to map these interaction structures is the Psychotherapy Process Q-Sort (PQS), developed by Ablon and Jones [15]. The PQS has previously been the topic of several empirical studies [16-18]. Some of this research has focused on single case studies. For example, Jones and Windholz [19] used the Psychotherapy Process Q-Sort intensively in their analysis of Mrs. C to examine the therapeutic process. The study of Ablon, Raymond and Smith-Hansen [20] summarized previous research and findings regarding the PQS and demonstrated its effectiveness in the implementation of various psychotherapy concepts, such as psychodynamic, cognitive-behavioral, client-centered therapy. Analysis of the interrater reliability for each item of the PQS has shown scores from 0.83 to 0.89. This instrument is thus able to identify process variables in psychotherapy. Only one study combined the methods of the PQS and the Plan Formulation Method to analyze the psychotherapy process. Dorber [21] examined the psychotherapy process in four therapy cases using the Psychotherapy Process Q-Sort and the Plan Formulation Method according to CMT and concluded that only a combination of both methods can develop satisfying insights into the psychotherapy process [21]. However, it has not yet been investigated whether specific test situations according to CMT can be identified using the PQS.
CMT, including the plan formulation method, provides methodological tools to investigate the dynamics of the unconscious during the therapeutic process. The plan formulation method operationalizes the identification of unconscious tests and pathogenic beliefs and proposes how to study the patient's and the therapist's reactions to interventions. Thus, CMT essentially contributes to the empirical knowledge of psychodynamic theory.
However, such contribution requires that the central criteria of CMT can be reliably assessed. Ideally, ratings on tests and pathogenic beliefs should follow the manual and be relatively independent from clinical experience. Thus, the goals of this study were the identification of tests according to Control Mastery Theory by well-trained raters and assessment of the reliability ratings of tools. Furthermore, based on the reliable identification of the test situation, the goal of the study was to examine whether the PQS method is appropriate for identifying tests according to CMT. The ability to identify tests could facilitate conducting single case studies on a broader basis.
Therefore, the research questions were the following: (1) Is it possible to identify tests according to Control Mastery Theory by well-trained raters? (2) How reliable are independent ratings of unconscious tests? (3) Is the PQS method appropriate for identifying tests according to the Control Mastery Theory?
This single case analysis is based on the transcript of a 35-session, short-term psychodynamic psychotherapy. The sessions occurred twice a week for seven months. The first five sessions were not recorded. There are verbal transcriptions for the remaining sessions, which were analyzed. The case, called "Ice Bear", was provided by Prof. Dr. Erhard Mergenthaler from the Ulmer database in Germany. The study was conducted by two independent raters who were graduate students in psychology at the Alpen-Adria University Klagenfurt with a psychodynamic teaching profile. Their CMT trainer was a licensed clinical psychologist and psychodynamic therapist who had received intensive CMT training according to the method of the San Francisco Psychotherapy Research Group. According to the plan formulation method, the first four available sessions of the transcripts were used to analyze the patient's plan. This process follows the assumptions of the plan formulation method, that the patient's plan and goals become obvious primarily at the beginning of therapy with the unconscious goal of providing the therapist with the necessary information.
The patient was a 33-year-old craftsman who was married and had two children. He came into psychotherapy because of chronic headaches after inflammation of the sinuses and depressive symptoms. Moreover, the patient abused analgesics (10 to 15 pills daily). At the beginning of therapy, the patient had been incapable of working for 4 months. During the course of therapy, his complaints improved, and the analgesics abuse declined. When the patient began to work again, therapy ended successfully, and the outcome was stable after a 3-year follow-up period.
Because the transcripts of the first five sessions were missing, the plan analysis of the Ice Bear was conducted using sessions six to nine. The two raters and the trainer independently identified the patient's goals, traumata, pathogenic beliefs, possible tests and helpful insights. The results were then combined, and the most relevant items were selected for the plan formulation (Table 1). Consequently, and according to the plan formulation method, three categories arose from the analysis (Table 1).
Table 1: Plan formulation of the "Ice bear" case. View Table 1
In further descriptions, the tests are called "Test 1", regarding the goal to develop more self-esteem, "Test 2", regarding the goal of assignment and "Test 3", regarding the category dominance.
Ablon and Jones [15] developed a pan-theoretical psychotherapy process measure, the Psychotherapy Process Q-Sort (PQS). According to Jones [14], this measure was developed to identify the interaction structure between the therapist and the patient. The measure comprises 100 items describing patient attitudes, behaviors or experiences; the therapist's actions and attitudes; and the nature of their interaction. Item 4, for example, reads "Therapeutic goals for the specific patient are discussed": Place toward characteristic if what the patient desires to have as an outcome of therapy is discussed in therapy. These desires might refer to personal changes or "internal changes" (e.g., "I started my therapy to overcome depression") or to life-linked changes (e.g., "I question whether therapy can help me get married"). Place toward non-characteristic if there are no references or allusions made by the therapist or the patient to the possible consequences of therapy [14].
To assess the interrater reliability of the identified tests, Cohen's κ was calculated using the SPSS statistics software, version 21 [22]. Cohen's κ is a standardized measure of the degree of agreement that deviates from random expectations [23]. In addition to the widely used Cohen's κ, we assessed the agreement rates with Yule's Y coefficient for each category because Yule's Y is independent of any base rate [23]. Interpretations of kappa coefficients were assigned according to Fleiss and Cohen [23], which was also used to interpret Yule's Y. Fleiss and Cohen [23] classified kappas as poor (0.00 to 0.40), fair (0.41 to 0.59), good (0.60 to 0.74) and excellent (≥ 0.75). In addition, to obtain an effect size, Cramer's V was estimated. According to the Cohen values of Cramer's, V = 0.10 is small, V = 0.30 is medium and V = 0.50 is a large effect size [24]. To obtain more detailed information regarding agreement, Cohen's κ was also estimated for the separate test categories according to the plan formulation method of the CMT (self-esteem, assignment and control/dominance).
For interpretation according to the PQS, each test-sequence was assigned to the 100 items of the Q-Sort method and allocated to a "characteristic pole", an "uncharacteristic pole" or a "neutral pole". Three clusters were developed: items that could be allocated to a CMT test sequence at least five times, items that were assigned fewer than five times, and items that could not be allocated in any test sequence.
Overall, 70 tests of the CMT could be identified; 45 were rated as tests by both independent raters, and 38 were assigned to the same test. Figure 1 shows the frequency of the identified tests by the two raters in the initial phase, the middle and the end of therapy. In the initial phase, the patient tests strongly on the topic of dominance, which decreases considerably in the course of therapy. Self-esteem tests, which represent the patient's needs, most frequently occur in the middle phase of therapy, whereas in the end, assignment tests are more frequent.
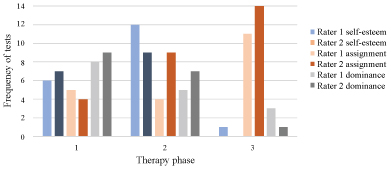 Figure 1: Frequency of tests for both raters and therapy phases.
Figure 1: Frequency of tests for both raters and therapy phases.
Note: Phase 1 = sessions 6 - 15; phase 2 = sessions 16 - 25 and phase 3 = sessions 26 - 35.
View Figure 1
Table 2 presents the agreement rates of the tests and the categories. Data analysis for the overall ratings showed a significant Cohen's κ of 0.38 with an effect size of Cramer's V = 0.52. Higher scores on agreement were reached for individual tests. In rating Test 1 (self-esteem), there was an agreement of κ1 = 0.51 and Y1 = 0.56.
Table 2: Agreement rates of the identified tests according to the Control Mastery Theory. View Table 2
An example of a test-sequence that was evaluated as Test 1 (self-esteem) by both raters is a situation in which the patient discussed his dream of becoming a writer and his doubts regarding that goal:
[...] One thinks repeatedly, 'Why can't you do what you want?' or the - (sniffs) and then I should talk about that with my wife, while she just said '[...] You can't do that and it's too expensive' and so on and so on, -(sniffs) but actually I do always hope that it will be fe-feasible one day (clears his throat).
What, - what (clears his throat).
Yes, just-to be somehow active as a writer.
Hmhm, you have already done it, when you are writing poems - - -
Well, it always was my dream to earn money with those things I like, you know, writing stories and short things like that, and that's.
Hmhm [...] well, (clears his throat) of course, that's a long way, but I believe the substantial information is that there're, there's a desire inside you (patient sniffs) which is unfulfilled [...].
Both raters categorized this as Test 1 (self-esteem) because the patient tested the therapist to determine whether the therapist would prevent the patient from giving up his desire.
A test of Category 2 (assignment) was a relapse of the patient's headache after the therapist forgot a session. In the following example, the therapist passed the patient's test. This relapse was perceived as a punishment and an assignment from the therapist:
There has been a relapse after the last session. Did something bother you? Before our last conversation? ----
Yes, of course (1) I mean, - there're always these, ------- [...] I'm so, I have a lot of time to think and to reflect and I think a lot about our conversations and - what we already have exposed, my faults or what I have, my false opinions that I have or had and, the conversations certainly had an effect and I do now, - don't have regrets that I have started that what we do that (little moan) ---- it's just that there isn't a direct relation to my headaches --- I still can't find it.
Well, such a direct relation is hard to establish. It's even astonishing why you, last Thursday, caught a cold after the session.
Why is it astonishing? -
Yes? You also could have caught a cold on Monday or Wednesday, or not at all, - but it was obviously the time following the session where you caught something. I think about the possibility that it has to do with this session. - If there maybe was something like a cold shower for you, -------- Why have you felt so bad in the last several days? -------- (patient coughs).
If I, if I, if my headache would have become stronger, then I would have felt worse, then I would have seen it directly in relation. But the last time I had, ehm, a heavy cold, ------
Well, whether it's more headaches or the cold, I don't believe it's that essential. The important thing is that you feel much worse again, ------ (patient breathes out audibly and clears his throat) and next week we don't have a session and (clears his throat) last time at the end I also forgot today's session? So I think that maybe could play a role, that you feel left alone? In the next time and that's something, as we know, not really easy for you. (patient takes a deep breath) -----
For sure (3), yes. I also thought about that and, --- (coughs) an ehm - somehow I will miss it. I like to come around here and -----just as today where you didn't think about it - I thought about that too - actually it disturbed me less, - (clears his throat) it's more that you are more human or more likeable for that, what I've discovered, --- anybody may forget something, so actually - sometimes it's good when something happens to someone else [....].
For ratings of Test 2 (assignment), analysis indicates κ2 = 0.46 and Y2 = 0.51. For the final category, Test 3 (control/dominance), there were scores of κ3 = 0.64 and Y3 = 0.69.
A frequent test of Category 3 implies that the patient wants the therapist to decide whether the patient is sufficiently healthy to return to work:
[...] Yes it gets, ehm, - I don't say it gets better from day to day, but it still stays better and has gotten better, - and actually, ehm, as soon as it gets better, I actually get into a little moral conflict: namely, I ask myself, ehm, is it okay to stay sick at home for so long? Stay there until I'm entirely recovered, or shall I try to work again? I don't have an answer to that anymore. -----
Hmhm, that's a similar problem as in the beginning. - Shall I still work, or is it okay to be ill, isn't it? ---- (patient breathes in and out).
So I want - would like to go to work - but I'm also afraid, that maybe I'll get sick again, so that I just can work for a few days or one week or two weeks and that I then - get sick again and everything maybe gets even worse and, - - (short sound and steps on the corridor during the pause) (little moan).
And that you then will be disappointed, ------ (patient sniffs, clears his throat) you say, now, so officially, 'It doesn't matter to still have headaches and go to work?' but, how does it look below? - -
Well, on the other hand (1), somehow, I wish for no headaches anymore, so that I can stand it, – so that I don't have headaches and don't need pills anymore - - -
Hmmh, that's what one wishes for, yes ---
Yes, one thinks that maybe one could try it, maybe it works, completely - - - -
It doesn't matter if your head hurts (clears his throat) - such as you told the club fellow who let you down, 'It doesn't matter' - - - - (steps and noises in the corridor) so, if you now work for fourteen days and it's a torture? and it gets worse again? - Then, you probably have the feeling that no one took good care for you, - nobody paid attention that it is too early, in fact? That you still have headaches, that you feel even worse, no one has taken your headaches seriously (steps in the corridor) such as in the beginning. - - -
Yes, for sure, I have that fear that ------
Hmhm, right, and thereby your worries are confirmed again? What happened before again and again, you have a wish or a concern, and it's not been taken seriously. [...].
The PQS [14] and tests according to CMT [3] indicated that 34 Q-Sort items were assigned more than 5 times and fewer than 21 times to the 3 CMT tests. An additional 35 items were selected for the 3 CMT tests fewer than 5 times. Thirty-one items of the Q-Sort were not selected for this case (e.g., use of humor). A combination of Q-Sort items represented one test situation according to CMT.
The majority of those items that were assigned more than five times to tests refer to the relationship between therapist and patient, such as Item 20, "Patient is provocative, tests limits of the therapy relationship"; Item 30, "Discussion centers on cognitive themes, i.e., ideas or belief systems"; Item 88, "Patient brings up significant issues and material"; and Item 97, "Patient is introspective, readily explores inner thoughts and feelings" [14]. These items present aspects that helped the patient to identify his position in the therapeutic process, the availability of the therapist and his personal development. In one testing situation that contained, for example, Item 88 and Item 97, the patient discussed his guilty conscience because he did things that were not good for him. This response suggests Item 88 because the patient became aware of his behavior and Item 97 because the patient explored his feelings and thoughts.
[...] When I don't do anything for a long time, I start to - to feel sick 'cause something's missing, ehm, - so it gets worse for me, - for a certain time, it's okay to do nothing and but then, ---
Then the idleness becomes a problem [...].
Fewer than five times, assigned items represented the behavior of the therapist the majority of the time, e.g., Item 6, "Therapist is sensitive to the patient's feelings, attuned to the patient; empathic", or Item 86, "Therapist is confident or self-assured" [14]. The example described above also includes Item 6 because the therapist reacted sensitively and empathically to the patient's worries.
The results show that tests could be identified with acceptable reliability and patterns in the frequency of the tests can be identified. We also found that PQS is not a practical tool for identifying tests. There are already many individual case studies on CMT and also on PQS. However, there are only a few studies on the reliability of test situations and there is no study on the operationalization of tests so far.
The results of the study demonstrate that well-trained students are able to identify tests according to the CMT, as Silberschatz and Curtis [11] and Silberschatz [10] assumed in former studies. The interrater reliability of the present study for the overall score (κ = 0.38) was lower but nevertheless acceptable for tests, which are mostly unconscious [10,11]. In the study of Silberschatz and Curtis [11], five independent raters identified tests in the therapies of two patients with an interrater reliability of r(k) = 0.50 and r(k) = 0.75. The study by Silberschatz [10] examined the verbal transcripts of 100 sessions of a patient. Nine graduates identified a total of 87 test sequences that were rated once again by three psychoanalytically trained raters. Those raters identified 46 central test sequences with a reliability of rkk = 0.82 (rll = 0.6) [10]. The results of these studies indicate moderate to very good reliability. For individual categories, the scores were even higher (Y1 = 0.56; Y2 = 0.51; Y3 = 0.69). These agreements range from acceptable to good. Differences in the category ratings can be attributed to the problem that tests could not always be clearly assigned to one category. Frequently, one rater allocated a test to Category 1 (self-esteem) and the other to Category 3 (control/dominance). For example, if the patient talked excessively although the patient asserted that he scarcely talked, one rater allocated this incident to the "self-esteem" category because the patient appeared to seek attention; however, the other rater interpreted this incident as the patient's attempt to control the therapist by his flow of words. This difference is a problem for research questions but less so in clinical practice. During the flow of therapy, the therapist can check the patient's reactions to his interventions and make corresponding corrections in his understanding. For research, the recommendation is to decide on diverging judgements by discussion and achieving consensus to arrive at an unambiguous case understanding.
Nevertheless, the plan analysis for the "Ice Bear" case can be judged to be appropriate and goal-oriented considering the therapy goal of 'patient's working ability' according to CMT [3]. The postulated 'expected behavior' of the patient and the therapist was confirmed during the course of therapy. The overcoming and disproving of the pathogenic beliefs by the patient's test and the therapist's pro-plan reaction led to awareness in the patient. Because the plan was exclusively formulated for the single case of the "Ice Bear", the plan cannot be compared with other single case studies. Weiss [1] demonstrated the reliability and the predictive validity of the plan formulation. By confirming the postulated 'expected behavior' during the course of therapy, the empirical evidence is strengthened by further studies [3,12,25]. The predictive validity of the plan formulation of the "Ice Bear" plan was also confirmed. The occurrence of the formulated expected behaviors was demonstrated to the therapist and was particularly distinct for the patient. The three categories of the "Ice Bear's" plan display particular intersections with regard to the interpretation of the particular formulation and rating of the situation. Thus, seven test situations, which were isolated by Rater A and Rater B, were not assigned to the same subject. Of those seven test situations, Rater A assigned the majority to the category "assignment", and Rater B assigned the majority of the situations to the category "control". This difference is the result of the intersection or rather the insufficient definitions of categories and the raters' subjectivity in their evaluating of particular situations. This dichotomy necessitates further research in terms of the definition of the test concepts according to the plan formulation method of CMT.
The process and the order of the test situations, which was developed by both raters, show the accumulation of test situations toward one topic until the process was concluded, as described in the theory [3,12,25,26]. According to CMT [3], a topic becomes restaged between patient and therapist until it is possible to classify the topic as 'solved'. Similar tests of that topic become rare and serve as ensuring verification, which describes the general statement concerning the 'testing in the therapeutic alliance' in Control Mastery Theory. The specific test order (model) was confirmed by the accumulation and progression of tests during the course of therapy in the "Ice Bear" case (Figure 1). If the patient began to increase the tests on the subject of 'control/dominance', these tests were followed by an accumulation of test situations on the topic of 'self-esteem'. With the approaching end of the therapy, the patient frequently created test situations on the topic of 'assignment' regarding the therapeutic alliance. This circumstance was accompanied by the patient's self-determined end of therapy, which moved the disengagement of the therapeutic alliance into the focus of testing. The therapist's interventions and behaviors, consciously or unconsciously, influence the form and frequency of the tests during the therapy process. The therapist's 'pro-plan' interpretations and reactions can shift the priorities of topics, explaining the progression of tests in the "Ice Bear" case, which described the subjects of conflict in different categories.
During the therapeutic work in the "Ice Bear" case, there were few (so defined) 'anti-plan' reactions by the therapist. The therapist's behavior during the therapy process conformed to the plan-defined therapist's behavior 'to overcome the pathogenic beliefs' and therefore was successful. The therapist's 'pro-plan' behaviors can be rated as a relevant factor in the psychotherapy of the "Ice Bear" case.
Another aspect of Control Mastery Theory is the trust in the therapeutic relationship. The more safe and stable the therapeutic relationship is, the more likely are frequent, intensive and risky tests during the course of therapy [27]. This issue was also addressed by the newly developed Patient's Experience of Attunement and Responsiveness Scale (PEAR) [28,29]. Based on the assumptions and the test concept of CMT [3], Snyder and Silberschatz [29] developed and evaluated patient and therapist versions. The authors measured attunement and responsiveness in a psychotherapy session to provide feedback to patients and therapists. The value of feedback provided directly to patients and therapists after each session based on CMT should be the focus of research in the near future.
The tests also imply the patient's ability to criticize the therapist as a person and the therapist's methods and interventions. In the "Ice Bear" case, this 'criticism of the therapist' could be identified in the category 'self-esteem'. Sammet, et al. [27,30] and Albani, et al. [31] described the recurring chance for the therapist to react in a 'pro-plan' manner during therapy after acting in an 'anti-plan' manner. Such a situation occurred in the "Ice Bear" case. The possibility of correction for the therapist arose from the patient's attitude toward a shared solution for the problem. Thus, the three categories ("self-esteem", "assignment" and "control") were successfully processed during therapy.
Q-sort items with a frequency of more than five test situations were primarily items that addressed the therapist and the therapist's behavior. Examples are Item 6, "Therapist is sensitive to the patient's feelings, attuned to the patient; empathic" [14], and Item 62, "Therapist identifies a recurrent theme in the patient's experience or conduct" [14]. These items suggest that the therapist's behavior in test situations and his professional input play a minor role compared with the patient's developing insight. Silberschatz [32] noted that "(...) patient factors clearly play an important role in many facets of therapeutic change processes (...)" [32]. The importance of patient factors also applies to those Q-sort items that occurred more than five times. Substantially, the therapeutic interaction and the quality of the therapeutic alliance were confirmed by the high frequency of those Q-sort items. It is important to consider that the Q-Sort method was not applied to the entire therapy process in the "Ice Bear" case. Only the test situations were examined using the Q-Sort method; thus, only the test situations that were relevant to the therapy process of the "Ice Bear" case were examined.
The Q-sort items that were attributable to one of the three plan categories ("self-esteem", "assignment" and "control") are particularly relevant. Those items include information regarding the modality of CMT tests in the context of the particular topics. For example, the category "self-esteem" was frequently assigned to Item 6, "Therapist is sensitive to the patient's feelings, attuned to the patient; empathic", and Item 35, "Self-image is a focus of discussion" [14]. Items such as Item 40, "Therapist makes interpretations referring to actual people in the patient's life", and Item 43, "Therapist suggests the meaning of others' behavior", often illustrated the category "assignment" [14]. The category "control" was assigned to Item 14", Patient does not feel understood by therapist", and Item 34, "Patient blames others, or external forces, for difficulties" in many cases [14]. It is important to consider that the Q-sort items that relate to one of the three plan categories reflect the character of the underlying patient's 'pathogenic beliefs' and the modality of the particular test. Thus, the result of the study is that test components can be assigned to items of the Q-Sort but not the complex interaction during a test according to CMT [21,33]. Further research should address this issue by developing and testing an instrument that measures typical test situations according to CMT. According to Silberschatz and Curtis [11], the therapist's pro-plan interventions are related to better therapeutic outcome, so it is important to be able to clearly identify the patient's tests. This can give therapists clearer indications of what they should pay attention to in their patient's actions. To this end, it would be important in future research to formulate and operationalize frequent tests and to develop a self-assessment instrument for patients. This could help to provide information across therapy approaches in everyday clinical practice on how patients can be helped to master their problems in a more targeted manner.
A central limitation of this study is that there were no outcome measures available to the patient; one central hypothesis of CMT, that passing a test is associated with better outcomes, could not be tested.
CMT assumes that the primary information the therapist requires for treatment is presented in the first therapy sessions. In this case, the analysis and the creation of the plan by the plan formulation were hindered by the missing transcripts of the first interview and the following five therapy sessions. Therefore, the plan formulation had to be conducted using an uncommon procedure given that the first patient-therapist interactions could not be used to develop the plan. Perhaps relevant data was thereby lost, such as possible relations with earlier sessions. References to earlier missing therapy sessions may have led to misinterpretation. Missing data are a primary problem of this study if one takes CMT for granted; however, the assumption that the first sessions are the most important for basic information is unproven, never having been empirically investigated. In everyday clinical practice, the collection of relevant data is often not limited to the beginning of therapy. Important information sometimes only appears during the course of therapy. Thus, we can assume that the material we assessed provided the necessary information. There are other studies in which the first interview is missing for the plan formulation, e.g., in the single case study "Amelie" of Albani, et al. [31].
To summarize, we determined that tests according to CMT could be reliably identified, but the PQS is not in fact feasible and cannot represent the complex interaction during these test situations. In addition, it would be necessary to measure this central hypothesis of CMT. Thus, further research can focus on formulating items for typical test situations to aid the therapist in identifying pro- and anti-plan interventions for the patient and to examine the relationship with regard to the outcomes for patients.