The electrical stimulation therapy (EST) of the Lower Esophageal Sphincter (LES) is a new treatment for Gastroesophageal reflux disease (GERD) that was always used in adult patients. In this work we describe the first two cases in children with GERD, treated with EST, the device improves the pressure of the LES, without interfering with its relaxation.
To describe the first two cases in pediatric population with the use of ENDOSTIM, and to show an alternative in the treatment of GERD by electrical stimulation.
Female, 12-years-old with GERD, with chronic pain, semi choking episodes, heartburn, regurgitation, who does not response to proton pump inhibitors with abnormal esophageal ph Demeester score of 63.2, hiatal hernia less than 3 cm and los angeles grade C esophagitis, evaluated by endoscopy and biopsies reporting chronic esophagitis, manometry with pressure at rest 10.1 mmHg (normal up 14), complete relaxation. The mother refused to perform Nissen fundoplication. The case was evaluated and approved by the Bioethics Committee of the hospital.
Male, 2-years-old with GERD, down syndrome, 9.1 kg weight, growth and with failure, aspiration pneumonia due to gastroesophageal reflux, with no response to proton pump inhibitors for about a year, endoscopy with los angeles grade C esophagitis, pathology with reflux, ph metry with 95% acid reflux, manometry relax pressure 10 mmHg.
Two Bipolar stitch electrodes were placed in the LES using laparoscopy and a dispositive was placed in a subcutaneous pocket. The electrical stimulation was delivered at 20 Hz, 215 ns, 3-8 mA, in 30 minutes session, with a recess of 90 minutes. Without chance of these parameters, the patient was evaluated using GERD daily symptom and medication use, endoscopy, esophageal ph and high resolution manometry.
One female patient, on chronic acid-suppressive therapy who underwent successful laparoscopic implantation of the LES stimulation system, surgery time 1 hour, trans surgical endoscopy with absence of perforation, closure of pillars; measured by GERD daily symptom diaries the patient symptoms improved soon. Two weeks after the surgery, the patient reported better symptom control without the intake of PPI, and the absence of heartburn and regurgitation. One month follow-up with esophageal ph shows decrease of the Demeester score to 20.2, and 3 months esophageal ph shows decrease to 3.9 (Normal Demeester score less than 14) manometry with primary peristalsis in 80% of swallowing, complete relaxation, pressure at rest EEI 16.9 mmHg, endoscopy with biopsies reported los angeles grade A esophagitis, without affection of the quality of life. The follow up 6 and 12 months after surgery describes the absence of any symptom, 6th postsurgical month ph Demeester index 9, manometry pressure at rest EEI 33, at normal endoscopy, 12th month Demeester 12, normal biopsies and endoscopy. One male patient, adequate laparoscopic implantation of LES stimulation system, 1 week after the surgery the patient has a normal feeding, decrease in symptoms, 3 weeks post-surgical weight increases 900 grs., first post-surgical month ph metry Demeester index 6, 28% of acid reflux, with improvement in their quality of life, 3rd post-surgical month endoscopy los angeles grade A esophagitis, ph 12% acid reflux, manometry pressure at rest EEI 17 mmHg, 6th month 0% ph with 0% acid reflux, endoscopy grade a los angeles esophagitis.
These are the first two pediatric cases in the world with electrical stimulation as a treatment for GERD. The results show that electrical stimulation of the LES can improve symptoms of GERD, reduce esophageal acid exposure augmenting esophageal sphincter pressures and reducing the need for PPI medication without Gastroesophageal side effects typically seen with other anti-reflux procedures that involve mechanical alteration of the gastroesophageal junction. Formal randomized clinical trials will test the true rate of operative complications and side effects and the studies could assess whether the device is restricted to patients with no hernia or if it is suitable for use after the repair to know the real benefit and safety of this study.
The term gastroesophageal reflux is purely descriptive and it refers to the involuntary and retrograde passage of gastric contents into the thoracic esophagus. It is a physiological phenomenon that occurs throughout life, so it is necessary to distinguish this physiological GERD (normal occurrence with no symptoms or signs of tissue damage that occurs in healthy individuals and that is very common in infants) from the pathological GERD or "gastroesophageal reflux disease", which is a condition capable of producing symptoms or histological lesions of the esophagus, as well as adverse effects in other systems.
The GER involves a physiological process in healthy children from 1 to 4 months of age, self-limited, with symptoms disappearing within 10 months (55%), 18 months (81%), and 2 years (92%). Boyle mentioned that 50% of patients have no symptoms at 6 months, 75% at 12 months and 95% at 18 months. The GERD and the gastroesophageal reflux disease have clear differences. The GERD is a pathological process with clinical manifestations, which occurs in 1 out of 300 children. Nelson SP reported an incidence of 2 to 7%. A higher prevalence has been observed in children with a history of esophageal atresia, neurological dysfunction and hiatal hernia, and it has been associated with chronic bronchitis and bronchiectasis [1-20].
The main anti-reflux mechanism is the competence of the lower esophageal sphincter (LES) or gastroesophageal sphincter. Often GERD episodes are produced by transient relaxations of the LES unrelated to swallowing, and to a lesser extent by increased abdominal pressure that overcomes the pressure of the sphincter. In infants and newborns this is an adaptive mechanism that allows the emission of belching with or without gastric contents, or is a response of the distension of the stomach lining, especially after feeding. Thus, the distension receptors present in the gastric walls help allow over distension, which is produced at high volumes of swallowed food and air. Therefore, paradoxically, breast-fed infants who are gaining weight perfectly or that even present overweight, tend to have more frequent episodes of GERD.
The contrast radiological study of the digestive tract was one of the first techniques used in the study of GERD in children. It is a test that has high sensitivity (i.e. it shows most episodes of GERD occurred in a period of time); however, its specificity is low and sometimes it cannot distinguish with certainty physiological GERD from pathological GERD.
The esophageal manometry consists of measuring pressure of lower and upper esophageal sphincters, as well as the evaluation of esophageal motility.
In cases of esophagitis, alterations of esophageal motility have been observed in the distal esophagus, with a decreased frequency and amplitude of peristalsis, and an occurrence of simultaneous contractions. Loss peristaltic activity of the distal esophagus may be responsible for the slowing of esophageal sweeping, shown in patients with severe esophagitis.
The prolonged esophageal pH registration or pH-meter of 24 hours shows the variations of esophageal pH, resulting from GERD episodes during an extended period (24 hours). Operationally, in this test it is defined as gastroesophageal reflux every episode of esophageal pH drop below 4.
Surgery is considered the definitive treatment for those children with refractory gastroesophageal reflux disease or where this is secondary to an anatomical alteration.
The proper surgical control of GERD in children needs an anti-reflux technique to maintain a good performance and that is intact over a long period of time; with this idea different surgical techniques were designed, with excellent results, introducing the belief that all these techniques were excellent options to cure the symptoms of our patients and that they could be applied to any of them with full warranty, regardless of the different clinical characteristics of patients.
However, in recent years, most of the literature about the reflux surgery refers the multiple complications that surgeons find in the medium-term follow up of operated patients, which allow observing some sort of post-surgical problem, even in 40% of the cases; these data suggest that the outcome of surgical treatment of GERD in children is not optimal.
Every time we come to agree more with the idea that there is not a perfect intervention for reflux control, this being the reason why the results of anti-reflux surgery in children are not optimal; therefore we propose an adaptation of the technique to perform according to the different anatomical and physiological characteristics of each patient.
Since this method recently used offers the beginning for oral treatment at 12 hours post-surgery, as well as the no modification of the anatomy of the esophageal hiatus, half-life of the implant of 12 years, the ability to program the intensity of the stimulation in out-patients.
The aim of anti-reflux surgery is to restore the cardia competition, mechanically improving its function to prevent the occurrence of gastric reflux into the esophagus, while the ability to swallow normally is preserved, relieving bloating and vomiting when necessary.
The electrical stimulation therapy of the lower esophageal sphincter is a method having adequate safety and efficacy for treatment of patients with gastroesophageal reflux because it achieves the control of symptoms in the patient without changing the esophagus anatomy.
A prospective, descriptive, observational study treatment trial conducted in a hospital. This study was approved by the Bioethics Committee. All patients have the inform consent form duly completed and signed, with the following inclusion and exclusion criteria (Table 1).
Table 1: Inclusion and exclusion criteria. View Table 1
Two electrodes with fixators directed to a bipolar stimulation, an implantable pulse generator, an external programmer (Figure 1), electro-stimulator cables that measure 45 cm and contain electrodes with fixators of platinum-iridium, bipolar, sterile in its distal portion which is implanted in the lower esophageal sphincter. The pulse generator is constructed of titanium and contains a lithium battery of medical grade, microelectronics communication coils and an accelerometer to detect the position of the patient. It is hermetically sealed to prevent damage of the device by biological secretions; the generator is connected and permanently implanted in a subcutaneous pocket in the lower left quadrant. The external programmer is similar to other devices, which allow the proper synchronization via laptop using specific software.
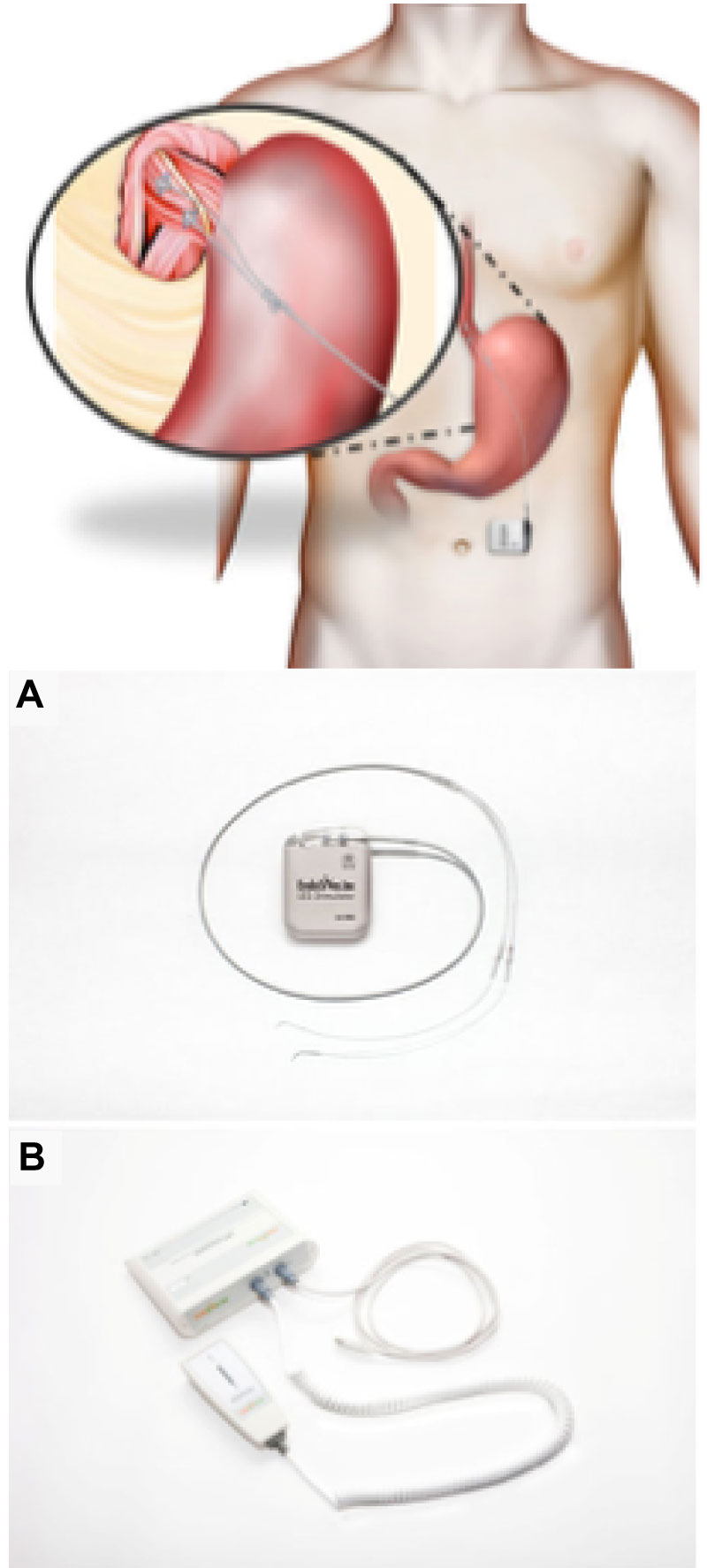 Figure 1: Position of the electrodes in the LES with one cm of distance between each one. A) Electrical stimulation therapy (65 mm × 48 mm × 12 mm, 49 grs, the programme, B) The programmer is external, executing by RF signal. View Figure 1
Figure 1: Position of the electrodes in the LES with one cm of distance between each one. A) Electrical stimulation therapy (65 mm × 48 mm × 12 mm, 49 grs, the programme, B) The programmer is external, executing by RF signal. View Figure 1
The placement of the stimulator of the lower esophageal sphincter is performed using standard laparoscopic techniques. The patient is positioned in the Trendelenburg position; before starting the procedure the area where the bag is placed must be marked in a length of 3 to 5 cm; the abdomen must be prepared in a sterile manner. Five trocars, two ports to mobilize the tissue, one trocar to mobilize the liver, a port of attendance and a viewing port are placed (all these trocars of 5 mm). The exposure of the esophagus is performed by electrocautery, with proper monitoring of the vagus nerve. In case is observed by a trans-surgical way it must be closed at that time. Through direct vision the fixation is performed with no absorbable suture in the muscular portion, with a distance of 1 cm placing a proximal electrode and a distal electrode. A surgical trans-endoscopy is performed in order to evaluate the absence of perforations. When the electrodes are fixed they are connected to the generator and placed in the reservoir bag made previously. At the time of completion of the procedure, a scan generator is performed through an extracorporeal programmer in order to modulate the intensity of the electrical pulse. The esophageal sphincter stimulation starts 12 hours after the implant procedure.
The system maintains stimulation according to the needs of each patient, using a pulse of 215 microseconds, 20 Hz, 3 to 8 mA sessions of 30 minutes. The number and duration of the stimulus is assessed according to the gastroesophageal reflux profile of each patient. The pressures are assessed by manometry, and acid exposure. The stimulation parameters can be adjusted and additional sessions can be added or adjusted or even been modified according to the symptoms presented by the patient during its follow-up. The generator has an accelerometer that can detect the supine position and it can generate additional sessions. The average battery life with typical use is 15 years and after that time it can be replaced without added complications.
Patients with inform consent form duly completed and signed by their parents or guardians who had inclusion criteria, who entered to the operating room for the placement of the device by laparoscopic technique described previously. The therapy with proton-pump inhibitors for two postsurgical weeks tracking patients is presented as follows (Table 2).
Table 2: Monitoring of studied patients. View Table 2
To assess the efficacy and safety of the electrical stimulation device of the lower esophageal sphincter and to evaluate potential adverse effects; to assess the symptom reduction calculated and evaluated with a questionnaire from three months post-surgery; to assess the exposure of the esophagus to acid, the degree of esophagitis; to evaluate the pressure increase at the end of exhalation of the lower esophageal sphincter; to assess the reduction of the intake of drugs (proton-pump inhibitors); and to assess the improvement in quality of life.
| Age | 2, 11 years old |
| Gender | |
| Male | 1 |
| Female | 1 |
| Duration of symptoms | 2 years |
| Duration of treatment (proton-pump inhibitors) | 2 years |
| Frequency of retrosternal pain (everyday) | More than 1 time per day |
| Frequency of regurgitation (everyday) | More than 1 time per day |
| Duration of nighttime reflux | 2 to 4 hours |
| Endoscopy | Los Angeles grade Cesophagitis |
| Hiatal hernia | 2 cm |
Female patient, 12-years-old, MODY diabetes, heartburn, sternal retro pain, episodes of semi drowning predominantly at night, nighttime cough, halitosis, chronic intake of proton-pump inhibitors, with no improvement, poor quality of life, poor school attendance, with an endoscopy with los angeles grade C esophagitis, hiatal hernia of 2 cm, ph metry with Demeester index of 68.2, manometry of 9 mmHg (Figure 2a and Figure 2b, Figure 3).
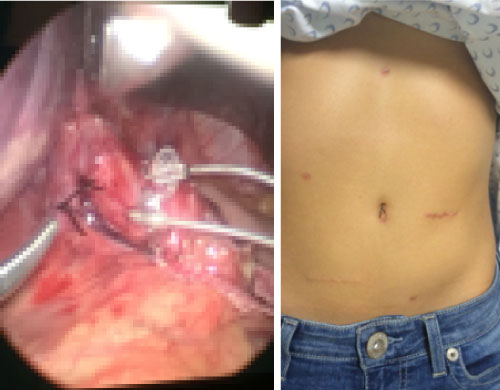 Figure 2: A) Image post surgical; B) Image trans surgical. View Figure 2
Figure 2: A) Image post surgical; B) Image trans surgical. View Figure 2
 Figure 3: Female patient, 12-years-old, MODY diabetes, heartburn, sternal retro pain, episodes of semi drowning predominantly at night, nighttime cough, halitosis, chronic intake of proton-pump inhibitors, with no improvement, poor quality of life, poor school attendance, with an endoscopy with los angeles grade C esophagitis, hiatal hernia of 2 cm, ph metry with Demeester index of 68.2, manometry of 9 mmHg. View Figure 3
Figure 3: Female patient, 12-years-old, MODY diabetes, heartburn, sternal retro pain, episodes of semi drowning predominantly at night, nighttime cough, halitosis, chronic intake of proton-pump inhibitors, with no improvement, poor quality of life, poor school attendance, with an endoscopy with los angeles grade C esophagitis, hiatal hernia of 2 cm, ph metry with Demeester index of 68.2, manometry of 9 mmHg. View Figure 3
Male patient, 1 year 9-months-old, 9 kg weight, Down syndrome, surgical history of PCA closure, dysphagia, heartburn, endoscopy with los angeles grade C esophagitis, hiatal hernia of 2 cm, ph metry with more than 95% of symptomatology (+) for acid reflux, manometry with pressure of 14.7 mmHg (Figure 4a and Figure 4b, Figure 5).
 Figure 4: A) Image postsurgical; B) Image trans surgical. View Figure 4
Figure 4: A) Image postsurgical; B) Image trans surgical. View Figure 4
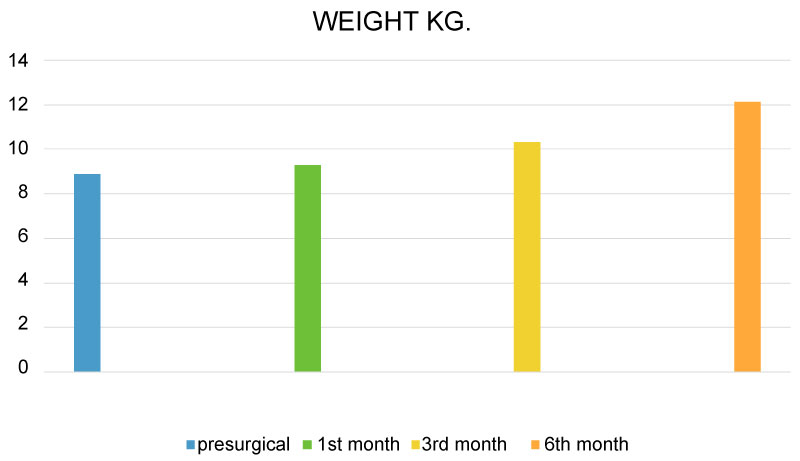 Figure 5: Male patient, 1 year 9-months-old, 9 kg weight, Down syndrome, surgical history of PCA closure, dysphagia, heartburn, endoscopy with los angeles grade C esophagitis, hiatal hernia of 2 cm, ph metry with more than 95% of symptomatology (+) for acid reflux, manometry with pressure of 14.7 mmHg. View Figure 5
Figure 5: Male patient, 1 year 9-months-old, 9 kg weight, Down syndrome, surgical history of PCA closure, dysphagia, heartburn, endoscopy with los angeles grade C esophagitis, hiatal hernia of 2 cm, ph metry with more than 95% of symptomatology (+) for acid reflux, manometry with pressure of 14.7 mmHg. View Figure 5
Post-surgical evolution described in (Table 3 and Table 4).
Table 3: Basal symptoms and post-surgical evolution with electrical stimulation therapy. View Table 3
Table 4: Basal symptoms and post-surgical evolution with electrical stimulation therapy. View Table 4
This is the first clinical trial in pediatric patients about the use of electrical stimulation of the lower esophageal sphincter for treating gastroesophageal reflux. The results show that electrical stimulation of the lower esophageal sphincter can safely reduce secondary symptoms of gastroesophageal reflux, measured by a personal diary of symptoms. Acid esophageal exposure can be reduced by increasing the sphincter pressure and eliminating the need to ingest proton-pump inhibitors chronically, as well as achieving the absence of typical side effects observed typically in other anti-reflux procedures involving a mechanical alteration of the gastroesophageal junction. Any adverse effects or abnormal feeling have been reported and specifically without interfering with the physiological relaxation of lower esophageal sphincter, without the presence of postsurgical dysphagia (Figure 6 and Figure 7).
 Figure 6: A) Initial Ph score; B) Ph score 12 times or more. View Figure 6
Figure 6: A) Initial Ph score; B) Ph score 12 times or more. View Figure 6
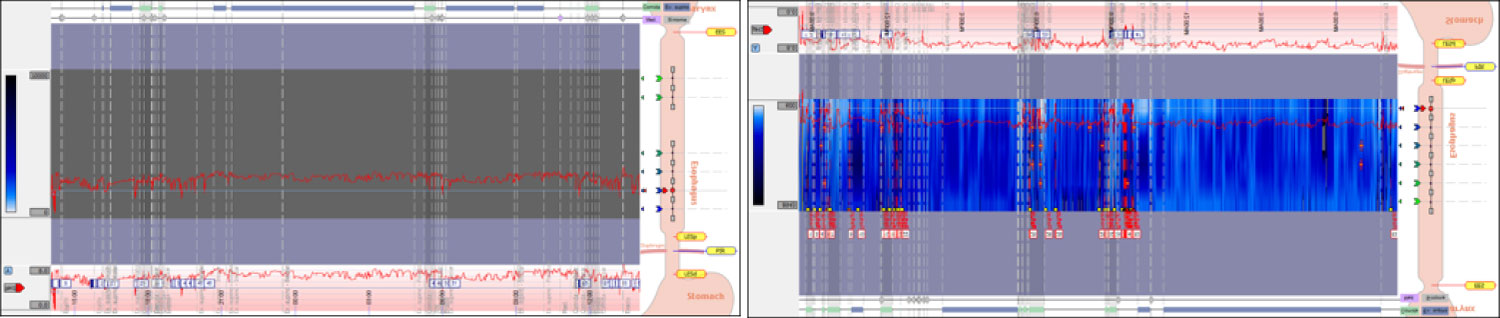 Figure 7: A) Initial Ph score; B) Ph score at the sixth month. View Figure 7
Figure 7: A) Initial Ph score; B) Ph score at the sixth month. View Figure 7
Surgical treatment guidelines of the American Society of Gastroenterologists and Endoscopists surgeons (SAGES) recommend surgery to patients whose treatment had failed, with poor quality of life, complications of gastroesophageal reflux disease, and Barrett's esophagus. In the same way, the established goals for anti-reflux device include the elimination of symptoms, the improvement of esophagitis, the prevention of complications and the maintenance of remission. The results observed in our patients suggest that the electrical stimulation of the lower esophageal sphincter in the long term, using a prolonged implanted device, can achieve these treatment goals. The improvement of the symptoms in its entirety is observed from the first post-operative month valued by the symptoms diary. There is a significant improvement of esophagitis from post-surgical third month. In a very significantly way, the electrical stimulation has no effect on the residual pressure of the esophageal sphincter and none of the patients in this study reported the presence of dysphagia.
This study describes the first two pediatric patients in the world with electrical stimulation of the esophageal sphincter as a treatment of gastroesophageal reflux. The results show that electrical stimulation of the sphincter can improve secondary symptoms of reflux, and also reduce the esophageal exposure to the acid, increasing the pressure of the lower esophageal sphincter, reducing the need to administer proton-pump inhibitors persistently, and achieving the absence of side effects from a surgical procedure involving a mechanical modification of the gastroesophageal junction. More randomized trials are needed to reinforce the effectiveness of this type of therapy in the pediatric population.