Allergic bronchopulmonary aspergillosis (ABPA) is an immunologically mediated lung disease caused by principally spores of Aspergillus fumigatus especially in asthmatic patients. Various set of diagnostic criteria has been advocated in different studies without a prevailing definition Treatment is based mainly on oral corticosteroids with the possible addition of antifungal agents.
We present a case of ABPA in an asthmatic patient who suffered of dyspnoea, coughing with green-brown sputum, pain in the left hemithorax, that has been admitted to our pulmonology department, with an initial suspicion of pulmonary neoplasm and pneumonia. CT scans showed consolidation at left ilo-apical site of the lung. Following blood tests and results of endoscopic examination that reports positivity for Aspergillus fumigatus, we make diagnosis of allergic aspergillosis and we start therapy with oral corticosteroid and antimycotic drug. At the follow up we found an exacerbation, but continuing therapy the symptomatology has improved.
ABPA is a well-established entity but the lack of uniform classification criteria creates further difficulties in the diagnosis. Analysis of anamnestic and radiological data with blood tests can help in the identification of this pathology that can mimicky other entities as in our case.
Aspergillosis, Asthma, Bronchiectasis
ABPA: Allergic Bronchopulmonary Aspergillosis
Allergic bronchopulmonary aspergillosis (ABPA) is an immunologically mediated lung disease that predominantly affects patients with asthma and cystic fibrosis [1]. The spores of Aspergillus (principally Aspergillus fumigatus), a fungus found worldwide, are dispersed by wind in the atmosphere and can be inhaled. Repeated inhalation of the spores can induce an allergic response in susceptible hosts, that can be IgE-mediated (type I) IgG-mediated (type III) and cell-mediated (type IV) [2]. A set of minimal essential diagnostic criteria has been advocated by GREENBERGER [1], which includes: 1) Asthma; 2) Immediate cutaneous reactivity to A. fumigatus; 3) Total serum IgE > 1000 ng/mL (417 kU/L); 4) Elevated specific IgE-/IgG- A. fumigatus, and 5) Central bronchiectasis in the absence of distal bronchiectasis. Conventionally, five stages of ABPA were identified: 1) Acute, 2) Remission, 3) Exacerbation, 4) Corticosteroid-dependent asthma, and 5) Fibrotic lung disease [3]. Treatment of ABPA is based mainly on oral corticosteroids [4]. An antifungal agent helps in suppressing the inflammatory response by mitigating the antigenic stimulus [5]. We present a case of ABPA in a patient who has been admitted to our pulmonology department, with an initial suspicion of pulmonary neoplasm and pneumonia.
The patient is a 46-year-old woman with asthma and atopy. In the anamnesis she has an history of severe endometriosis with removal of the right and partially left ovary, exploratory laparoscopy to clear further abdominal sites, IgA nephritis, hepatitis C, upper right lobectomy for bronchiectasis an year before. She came to our attention for persistence from several months of exercise dyspnoea, coughing with green-brown sputum that did not improve with antibiotic intake, pain in the left hemithorax. The sputum culture test showed positivity for Klebsiella pneumoniae and Acinetobacter baumannii. Levofloxacin therapy according to antibiogram was prescribed for 15 days without improvement. Therapy with piperacillin-tazobactam was then prescribed. On the advice of thoracic surgery of this hospital, which carried out the right superior lobectomy, performed chest CT with iodinated contrast medium that showed parenchymal consolidation at left ilo-apical site of the lung with bronchogram without evidence of ilar and mediastinal lymphnode swelling (Figure 1a and Figure 1b). We decided, therefore, the hospitalization in our department.
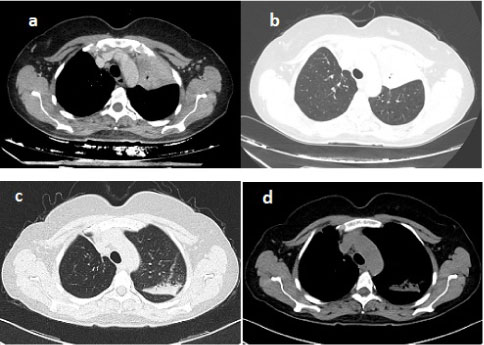 Figure 1: Initial CT scans that show parenchymal consolidation at the upper left lobe (a,b); CT scans at the same level after one month of therapy (c,d). View Figure 1
Figure 1: Initial CT scans that show parenchymal consolidation at the upper left lobe (a,b); CT scans at the same level after one month of therapy (c,d). View Figure 1
During the hospitalization, blood tests were performed showing leucocytosis with 2530 eosinophils/ml (15% of leukocytes), C reactive protein 5.62 mg/dl, total IgE 2602 KU/L, negative Interferon Gamma Release Assay (IGRA). We also performed sputum culture examination that showed positivity for Aspergillus fumigatus. We therefore decided to perform bronchoscopy: the anterior segmental bronchus of the left upper lobar bronchus appeared reduced in size with inflamed mucosa. At this level samples were taken for microbiological and cytological examination and transbronchial biopsies were performed for histological examination. The result of the microbiological examination has confirmed the presence of Aspergillus fumigatus. The cyto-histological examination showed inflammatory cells, bronchial elements with reactive appearance, pulmonary macrophages and eosinophils in a context of chronic non-specific inflammation. We decided to check for the presence of specific IgE for Aspergillus Fumigatus which were positive (1.69 KU/L). The patient was also tested for immediate cutaneous reactivity to Aspergillus fumigatus which was positive. Then we started therapy with Itraconazole 200 mg per day and Prednisone 25 mg per day. A week later, the patient underwent a new bronchoscopy in which a caliber increase was seen in the anterior segmental bronchus of the left upper lobar bronchus. The microbiological examination again confirmed the presence of Aspergillus fumigatus and the cytological examination also showed occasional Charcot Leyden crystals (Figure 2). We therefore decided to continue therapy and to recheck the patient with a chest CT scan after one month (Figure 1c and Figure 1d). New chest CT showed complete resolution of parenchymal consolidation in the left anterior ilo-apical site, persistence of point-like nodular consolidation, increased parenchymal consolidation with air bronchogram in the left posterior ilo-apical site. After another month of therapy with prednisone and itraconazole, chest CT was newly performed that highlights consolidation with cylindric bronchiectasis in the medial segment of the middle lobe, consolidation in the posterior and upper site of left lung, dense fibrotic bands in the lingula. Blood tests were almost normal. So we can consider first a stage 1 (acute) and then a stage 3 (exacerbation) diseases.
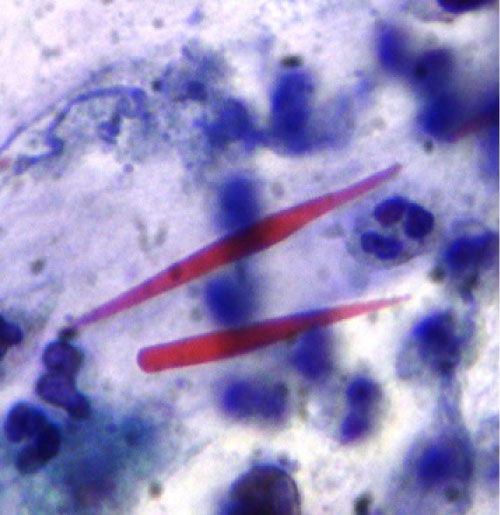 Figure 2: Charcot Leyden crystals. View Figure 2
Figure 2: Charcot Leyden crystals. View Figure 2
ABPA is a well-established entity but its exact prevalence is yet to be estimated. The lack of uniform classification criteria creates further difficulties in the identification of this pathology. Therefore the diagnosis of ABPA is based on an integrated analysis of anamnestic and radiological data with blood tests. At a first evaluation of the CT images, our patient showed a pulmonary consolidation at the upper left lobe that posed the suspicion of a lung tumor. For this reason a bronchoscopy was also performed. Considering histological, cytological and microbiological results and integrating the anamnestic data of bronchiectasis and bronchial asthma, following the blood tests, we diagnosed ABPA. In conclusion, presence of pulmonary consolidation in patients with a history of bronchectasis and bronchial asthma, it should always be considered ABPA in the differential diagnosis of other diseases that may have the same appearance on radiological examinations.
Not applicable.
The patient consents to publish her data including images.
The datasets analysed during the current study are available from the corresponding author on reasonable request.
The authors declare that they have no competing interests.
All authors read and approved the final manuscript.