Avulsion fractures of the anterior superior iliac spine are uncommon without established treatment guidelines. Deciding between nonoperative versus surgical management depends on the grade of displacement, skeletal maturity, type of sport/activity, and competitive/career requirements.
We present a young athlete who sustained an ASIS avulsion fracture while playing baseball that was treated with open surgical reduction and fixation using absorbable sutures with an emphasis on mobilizing the TFL to reapproximate the avulsed segment without tension.
The patient was started on a progressive physical therapy protocol that did not involve any weight-bearing or range of motion restrictions. He was jogging in the third postoperative week and returned to full-play in the 6th week. As of 12 months postop, there were no complications and he is playing at his pre-injury level of performance without pain.
Operative treatment of avulsion fracture of the ASIS without bone anchors or screws highlights the importance of soft tissue mobilization and reduction of tension. Additionally, the relatively rapid return to activities and lack of immobilization minimizes deconditioning, which might be an advantage over non-operative management. Athletes with ASIS avulsion fractures repaired with this technique can expect to return to play within 6 weeks.
Tensor fascia latae (TFL), Anterior superior iliac spine (ASIS), Avulsion fracture, Core muscle injury
ASIS: Anterior Superior Iliac Spine; TFL: Tensor Fasciae Latae; MRI: Magnetic Resonance Imaging
Avulsion fractures of the anterior superior iliac spine are uncommon and there are no established treatment guidelines. The decision between nonoperative versus surgical management depends on the grade of displacement, skeletal maturity, type of sport/activity, and competitive/career requirements.
The Anterior Superior Iliac Spine (ASIS) serves as the origin of the sartorius muscle and of parts of the Tensor Fasciae Latae (TFL). Avulsion injuries of the ASIS constitute 1.4% of injuries of the hip and pelvis and 19% of avulsion injuries of the pelvis [1,2]. A sudden forceful strain on the sartorius or the tensor fasciae latae during the starting phase of running or jumping is the most common mechanism of accident. Apophysis ossification of the ASIS usually occurs between the age of 21 and 25. Prior to the ossification, the epiphyseal plate is weaker than the myotendonous junction or pelvic bone, making avulsions more likely in younger athletes [3].
We present the case of a young athlete who sustained an ASIS avulsion fractures while playing baseball that was treated with open surgical reduction and fixation using absorbable sutures with an emphasis on mobilizing the tensor fascia latae to reapproximate the avulsed segment without tension.
The patient is a 16-year-old, Risser stage 2, high-level high school baseball player who felt a pop and sudden, sharp pain at the right ASIS while simultaneously running the base path and shifting his hips to his right to avoid a tag [4]. Upon examination two days later, he had profound weakness and pain with right hip flexion. Pelvic x-ray and magnetic resonance imaging (Figure 1A and Figure 1B) demonstrate a 2.5 cm avulsion of the right TFL with a 2.2 × 0.8 cm chip of bone displaced inferolaterally from the ASIS and an intervening hematoma.
 Figure 1: (A) X-ray; (B) MRI (STIR) demonstrating the avulsed ASIS. The bone fragment is displaced inferolaterally (white circle). View Figure 1
Figure 1: (A) X-ray; (B) MRI (STIR) demonstrating the avulsed ASIS. The bone fragment is displaced inferolaterally (white circle). View Figure 1
The procedure was performed under general anaesthesia with Laryngeal Mask Airway (LMA) intubation. The patient was not given paralytics so that resting tone would allow better approximation of the tension on the muscles. The patient was placed in supine position and the anterolateral pelvis and thigh was prepped and draped. A vertical 3 cm skin incision was made below and just lateral to the ASIS. The fascia was divided longitudinally while taking care to protect the lateral femoral cutaneous nerve. This allowed entry into the hematoma cavity and palpation of the bony fragment distally. The origins of the sartorius muscle and the tensor fascia lata remained attached to the flake (Figure 2A). Following a combination of blunt and sharp dissection within the fascial compartment of the TFL and along the TFL and sartorius fascia, the bone fragment could be reapproximated to the avulsion site (Figure 2B).
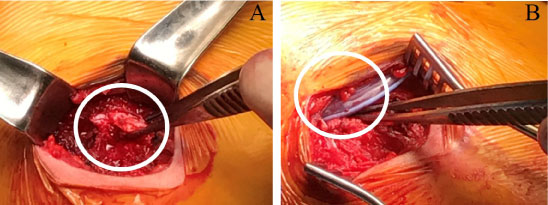 Figure 2: Intraoperative photos (A) The avulsed bone fragment with attached TFL and sartorius (white circle) is held in the forceps; (B) The forceps point to the location of the bone chip (white circle) after it has been reapproximated. A blake drain is superficial to the repair. View Figure 2
Figure 2: Intraoperative photos (A) The avulsed bone fragment with attached TFL and sartorius (white circle) is held in the forceps; (B) The forceps point to the location of the bone chip (white circle) after it has been reapproximated. A blake drain is superficial to the repair. View Figure 2
Absorbable sutures (0-PDS) were then placed between the myontendonous origins of the TFL and sartorious and the surrounding periosteum and soft tissue (external oblique, intact iliotibial band fibers, and gluteus maximus). A blake drain was placed on top of the repair.
The patient was started on a progressive physical therapy protocol that did not involve any weight-bearing or range of motion restrictions. The drain was removed on postoperative day 6. He was jogging in the third postoperative week and returned to full play in the 6th week. As of nine months postop, there were no complications and he is playing at his pre-injury level of performance without pain.
There are no established treatment guidelines for avulsion fractures of the ASIS in the literature. The two most-commonly recommended treatment options are non-operative management and open reduction with screw or anchor fixation. Non-operative treatment can involve immobilization with the hip and knee in flexion to off-load the area of injury [5,6]. This combined with NSAIDs and subsequent gradual mobilization is a commonly-reported approach for non-displaced or minimally displaced fractures. Open reduction and screw fixation has been recommended in cases involving greater displacement of the bone fragment. Surgical treatment has been associated with a shorter rehabilitation period allowing an earlier return to athletic activities [7]. In a comparison of 23 adolescent patients with avulsion fractures of the ASIS of whom 10 were treated conservatively and 13 operatively, the final outcome after 1-year-did not show any differences between the two treatment groups as assessed by the visual analog scale and range of motion [1].
The history of trauma, clinical examination, and standard radiographs can be sufficient for a correct diagnosis. The avulsed fragment usually is displaced distally and laterally [8]. In addition to standard radiography, Magnetic Resonance Imaging (MRI) is useful in cases with inconclusive X-ray findings [9]. Avulsed ASIS usually have an associated hematoma and severe cases with extensive callous formation have been mistaken for bone tumors or infectious processes [10]. Severely displaced fragments may also lead to compression of the lateral cutaneous nerve causing meralgia paraesthetica [11,12]. MRI is also helpful in defining the extent of the soft tissue injury and the structures involved.
Operative treatment of avulsion fracture of the ASIS without bone anchors or screws highlights the importance of soft tissue mobilization and reduction of tension on these repairs. Applying mobilization techniques, we have developed in treating adductor avulsion injuries reduces tension on the repair and obviates the need for bone fixation. Additionally, like the surgical approach described by Wilinger, et al. [3], this surgical approach does not violate the chondral growth zone of the pelvic apophysis and allows the injury to heal with less of a risk of growth disturbances as compared to screw fixation through the bone fragment [12]. The relatively rapid return to activities and lack of immobilization minimizes deconditioning, which might be an advantage over non-operative management. Athletes with ASIS avulsion fractures repaired with this technique can expect to return to play within 6 weeks.