Non traumatic acute abdomen is an acute onset of abdominal disease entities that require immediate surgical intervention in most of the cases. The causes of non-traumatic surgical acute abdomen and their relative incidence vary in different populations.
The aim of this study was to assess the management outcome and associated factors of surgically treated non-traumatic acute abdomen.
Hospital-based prospective cross sectional study was conducted on surgically treated non-traumatic acute abdomen cases admitted at Attat catholic hospital surgical ward starting from January 2017 to September 2018. Data was collected using history, physical examination, patients' card and operation registration book as necessary. The collected data were checked for incorrectness and inconsistencies and SPSS version 21 used for the descriptive, binary and multivariate logistic regression analysis of the data. On binary logistic regression analysis a p-value < 0.25 was used as a candidate for multivariate logistic regression analysis. Statistical significant association was tested at a p-value of < 0.05.
There were 192 non-traumatic emergency surgical acute abdomens admitted in surgical ward and 171 (89%) of cases were managed surgically while 11% were managed conservatively. The three top causes of acute surgical abdomen were acute appendicitis accounting 48% followed by bowel obstruction 28% and Peritonitis 24%. Late presentation of patients before intervention, sex, age and postoperative complications were independent predictors with management outcome in our study. The total postoperative complication rate was 17% of which the commonest early postoperative complications were wound infection (5.4%), sepsis (4.3%) and pneumonia (2.3%). About 90.1% were discharged well while 9.35% were passed away in the hospital which is unacceptably high mortality.
The overall mortality was more in cases from rural area due to delay at presentation, on higher extreme age patients, those who developed peritonitis and postoperative complications. To decrease this problem, creation of health awareness on acute abdomen to the general population and to the low and mid-level health care providers for early referral, pre and postoperative management to decrease postoperative complications and death has great importance.
Surgically treated, Non-traumatic surgical acute abdomen, Complications, Outcome
BP: Blood Pressure; EOPD: Emergency Outpatient Department; GLBO: Gangrenous Large Bowel Obstruction; GSBO: Gangrenous Small Bowel Obstruction; ICU: Intensive Care Unit; IEOS: Integrated Emergency Obstetrics and Gynecology and Surgery; IO: Intestinal Obstruction; Km: Kilometer; LBO: Large Bowel Obstruction; ACH: Attat Catholic Hospital; NRH: Nekemte Referral Hospital; NTAA: Non Traumatic Acute Abdomen; PPUD: Perforated Peptic Ulcer Disease; RLQ: Right Lower Quadrant; SBO: Small Bowel Obstruction; SPSS: Statistical Package for Social Sciences; TAH: Tikur Anbesa Hospital
Acute abdomen is an acute onset of abdominal disease entities that require immediate surgical intervention in most of the cases. It is the most common presenting surgical acute abdominal emergency that has been estimated at least 50% of general surgical admissions are emergencies and 50% of them present with acute abdominal pain and encompasses a spectrum of surgical, medical and gynecological conditions, ranging from the trivial to the life-threatening, which require hospital admission, investigation and treatment [1].
Non traumatic surgical acute abdomen is a part acute abdomen caused by surgical cases excluding trauma and it is common challenging clinical scenario requires a thorough and expeditious workup to determine the need for operative intervention and to initiate appropriate therapy. Many diseases, some of which are not surgical or intra-abdominal can produce acute abdominal pain and tenderness. The diagnoses associated with an acute abdomen vary according to age and gender. Appendicitis is more common in the young whereas biliary disease, bowel obstruction, intestinal ischemia and infarction, and diverticulitis are more common in elderly patients [2].
The causes of acute abdomen are several and their relative incidence varies in different populations. Several factors are described to be responsible for these differences. Socioeconomic factors and diet have mostly been incriminated to be responsible for the observed differences [3].
Worldwide, appendicitis, bowel obstructions, incarcerated or strangulated hernias, volvulus, and acute biliary pathology remain the most common causes of the non traumatic surgical acute abdomen. The most common symptoms are abdominal pain and vomiting whereas tenderness and guarding are the most frequent clinical signs. It is common surgical emergency accompanied with high morbidity and mortality if not managed properly [4,5-8].
Intestinal obstruction has been the leading cause of acute abdomen in several African countries whereas acute appendicitis is the most frequently seen cause in the developed world. The leading causes of intestinal obstruction in Africa have mostly been hernia and volvulus whereas adhesions are most frequent in the developed world [3,5,9]. In Ethiopia, especially in SNNR, little is known about non traumatic surgical acute abdomen. But some evidences show that it is a commonly encountered condition accounting for 9.3% total surgeries to 79% of the surgical emergency surgeries. The overall mortality of 18.6% and post-operative hospital mortality rate of 14%. Wound infection, sepsis and pneumonia are the most common postoperative complication and associated with long hospital stay [10-12].
Acute abdomen is often a surgical emergency and a challenge to any surgeon. It is one of the commonly encountered emergencies in the practice of general surgery and for which emergency surgical operation commonly performed [1,9,13].
Non traumatic acute abdomen is an integral of acute abdomen and is an important public health problem that remains a primary concern to both patients and surgeons. It is relatively non preventable common global emergency consuming much in terms of surgical services. It represents up to 54% of general surgical admissions in some Asian countries whereas up to 88.2% of total emergency operations in few African countries. Despite of modern surgery is being practiced; the mortality rate following non traumatic acute abdominal surgical emergencies is still high worldwide being the highest at the extremes of age [9,10,14].
Lack of health education, improper health care facilities and late presentations are common factors for increased morbidity and mortality. Old age (> 55-yrs) and duration of illness greater than two days were factors statistically associated with postoperative complication. Emergency procedures generally are associated with increased morbidity and mortality rate in elderly patients (the overall mortality reaches 22% [3,11,15]).
The magnitude of non-traumatic surgical acute abdomen is different in deferent areas due to socioeconomic, demographic factors and diet habit. In addition to this, the incidence of post-operative complications varies in different regions and setups [8,16-18].
The pattern of the disease changes from time to time and needs periodic studies to evaluate the etiological factors and behavior of the disease. Global as well as regional variations in the pattern of non traumatic acute surgical abdomen and changes in the disease pattern over the years are well documented in the literature [16,18-20].
In Ethiopia, especially in Southern Nations and Nationalities Regional state, very little is known about outcome and associated factors of surgically treated non-traumatic acute abdomen and there is no literature that indicates the associated factors and final outcome of patients who are managed operatively for the diagnosis of NTSAA in Attat Hospital. This study is therefore, aimed at assessing this problem.
This study was conducted at Attat Catholic Hospital (ACH) which is found 175 km southwest of Addis Ababa and is 410 km far from the regional capital, Hawassa. The Hospital was established in 1961 E.C with a religious mission and still now governed by religious missionary and mainly centered for Cheha Woreda of Gurage Zone, Southern Nations and Nationalities Regional state. Its catchment population is 1,279,646 of which 51.2% females and 48.8 % males. The Zone has 40 Health Centers and two newly established primary Hospitals which are government owned and ACH serves as referral center to these hospitals and health centers. This hospital has 103 beds including surgical ward which give 24 hours services and it has multidisciplinary staffs (one general surgeon, one gynecologist, two emergency surgeons, 8 general practitioners, two pharmacists (degree holder), 8 pharmacy technicians (Diploma holders), two radiographers, two lab technologist (degree holder), 6 lab technicians (Diploma holders), 15 Bachelor degree and 40 Diploma clinical nurses, 10 midwives, and 3 anesthesia professionals). A facility based cross-sectional study was conducted from January to September 2018.
A hospital based cross-sectional study design was conducted. All surgical acute abdomen cases admitted in ACH surgical ward within the study period prospectively in nine months.
All surgically treated non-traumatic surgical acute abdomen patients admitted at ACH surgical ward within the study period.
All cases that surgical management was performed for the diagnosis of non-traumatic acute abdomen during the study period were included in this study.
• Traumatic, gynecological and medical acute abdomen.
• Patients with diagnosis of non-traumatic surgical acute abdomen who were managed conservatively.
• Patients operated out of ACH and admitted after operation to ACH.
• Management outcome of surgically treated non-traumatic acute abdomen.
• Age
• Sex
• Place of residence
• Care given to patients
• Type of procedure
• Intra-operative finding
• Causes of illness
• Duration of illness before management
• Clinical features
• Occupation
• Duration of hospital stay
• Data collection methods
For data collection, four clinical nurses working at Attat hospital and one BSc nurse was recruited. The principal investigator gave training for data collectors on how to fill the prepared checklist, the importance of data quality and the relevance of the study (Annex 1). Two BSc nurses supervise the daily activity, consistency and completeness of the checklist alternatively and appropriate support was given during the data collection process and checked the daily activities of data collectors and supervisor. A checklist was developed based on objectives of this study from different literatures and by principal investigator using English language to extract relevant information and was taken place at inpatient ward.
The checklist had different parts including;
Part I. Socio demographic characters
Part II. Presenting complaints and signs of the patient
Part IIІ. Diagnosis
Part IV. Management outcomes
Patients admitted to Attat hospital surgical ward with the diagnosis of non-traumatic surgical acute abdomen within the study periods were identified by taking history, physical examination, intra-operative findings and post-operative results were used to collect important information.
After data was collected, it was coded, entered and cleaned to Epidata computer software; it was exported to SPSS windows version 21 for descriptive and logistic regression analysis of the data. Descriptive, binary and multivariable logistic regression analyses were used. On binary logistic regression analysis a p-value < 0.25 was used as a candidate for Multivariable binary logistic regression analysis. Data was presented by frequency tables and figures. Association between dependent and independent variables was checked by using logistic regressions model. The result was presented using frequency tables, graphs and percentage. Statistical significance was based on a p-value of < 0.05 with a confidence interval (CI) of 95 % to check the association between outcome variables and certain independent variables.
Before data collection, the prepared checklists in English was assessed and commented by research advisors. The facilitators and supervisor were trained for two days. During data collection, in order to avoid the interpersonal variation between data collectors, data was collected by the same data collectors throughout the data collection. Regular, twice per week supervision was taken placed for checking the consistency and completeness of checklist by the principal investigator. Before starting data analysis, completeness was rechecked.
• Acute abdomen-Any sudden condition with chief manifestation of pain of recent onset in the abdominal area which may require urgent surgical intervention.
• Non traumatic acute abdomen-Acute abdomen which is not secondary to trauma diagnosed by top senior (general surgeon) in the ward.
• Surgical acute abdomen-Acute abdomen secondary to surgical cases.
• Appendicitis-Inflammation of appendix.
• Appendectomy-Surgical Removal of appendix.
• Colostomy-Connecting the colon to the abdominal wall for stool drainage.
• Intussusceptions-Invagination of one part of bowel lumen in to the other.
• Laparotomy-Incision through the abdominal wall.
• Peritonitis-Inflammation of peritoneum.
• Intestinal obstruction (IO)-Intestinal obstruction is prevention of passage intestinal contents.
• Wound dehiscence-Is facial disruption due to abdominal wall tension overcoming tissue or suture strength, or knot security.
• Clinical manifestation-Sign and symptom of the case.
• Anastomosis-The surgical union of two hollow organs, e.g. parts of the intestine, to ensure continuity of the passageway and anastomosis leak refers to leakage through surgical union site.
• Intra-operative procedure-The procedure that can be done after laparotomy which can be resection & anastomosis or colostomy or etc. depending on the causes& intra-operative finding of obstruction.
• Intra-operative finding-The finding after abdomen is opened which can be gangrenous bowel or viable bowel, etc.
• Non operative management (conservative)-Means management of patients with appendiceal mass, partial bowel obstruction, recurrent adhesive obstruction, or during the early postoperative period with NGT suction, IV fluids and frequent clinical reassessment to rule out bowel strangulation which may need operative management.
• Operative management-Means surgical exploration of the abdomen.
• Favorable outcome-Patients with a clinical diagnosis and operatively managed for acute abdomen then improved and discharged from the hospital.
• Unfavorable outcome-Patients with a clinical diagnosis and operatively managed for acute abdomen but not improved on discharge (including death, referral, worsened).
Ethical clearance was obtained from institutional Health Research Ethics Review Committee of Jimma University College of Health and Medical Science (COHMS). A formal letter was written from the coordinator of Integrated Emergency Obstetrics/Gynecology and surgery to the hospital administrator office. The Hospital medical director was permitted us to conduct the study. All information was obtained using client interview by structured questionnaire and observing the procedure by filling the prepared checklist. The filled checklists will be destroyed after the study has finished. Issues of risks, benefits and rights were also being considered.
During the nine months study period, there were 423 total surgical admissions in Attat hospital surgical ward. The number of patients admitted with the diagnosis of non traumatic surgical acute abdomen was 192 of which 171 were for surgically treated non traumatic acute abdomen that we retrieved which made the basis of this study. 89% of these NTAA cases were managed surgically while others managed conservatively. There were 107 (62.6%) male and 64 (37.4%) female with male to female ratio of 1.7:1 respectively (Table 1). The age ranged from 01 to 69 years with a mean age of 31.46 ± 17.4 (SD) years. 115 (67.3%) patients were rural and 56 (32.7%) patients were urban dwellers. The duration of illness before operation ranges from 4hrs to 9 days with mean of 3.54 days. 75 (43.9%) of patients came within 48 hrs of illness while 96 (56.1%) came after 2 days of illness. Abdominal pain (100%), vomiting (80.1%), constipation (48.3%) and abdominal distension (53%) were the main presenting symptoms whereas abdominal tenderness, distension and guarding were the most frequent clinical signs found (90.6%, 46.8% and 40.4% respectively) (Figure 1). 73.7% of patients had blood pressure of >= 90/60 mmhg and 26.3% were in shock (BP < 90/60 mmhg). 63.7% of patients were tachycardic (Pulse rate > 100 bpm and 46.8 % of patients were febrile (temp >37.5 c (Table 1). The three top causes of acute surgical abdomen (Figure 1) were acute appendicitis accounting 82 (48%) followed by bowel obstruction 48 (28%) and Peritonitis 41 (24%).
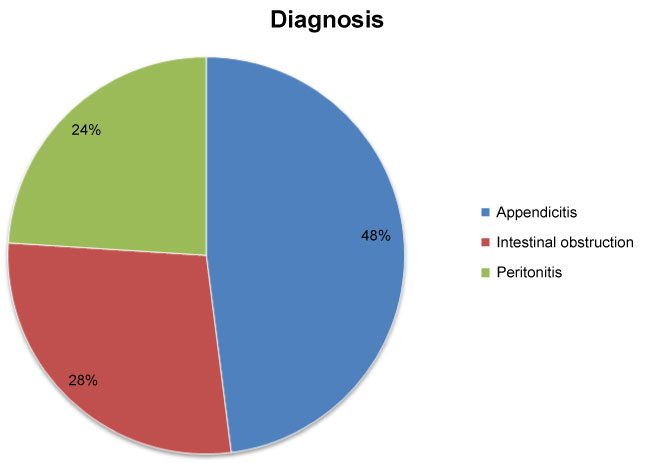 Figure 1: Type of surgically treated non-traumatic surgical acute abdomen diagnosed in ACH surgical ward from January to September 2018. View Figure 1
Figure 1: Type of surgically treated non-traumatic surgical acute abdomen diagnosed in ACH surgical ward from January to September 2018. View Figure 1
Table 1: Sociodemographic characteristics and clinical features in patients with non traumatic surgical acute abdomen in Attat Primary Hospital, from (January 1, 2018-September 30, 2018 G.C). View Table 1
Appendicitis is the leading causes of acute abdomen 82 (48%), among 82 cases of appendicitis 55 (67%) were males and 27 (33%) were female. 44 (53.6%) of patients came from rural while 46.4% were from urban. Appendicitis was high in prevalence in 2nd and 3rd decades 43 (52%) from surgically treated NTAA and low in both extreme age groups. Students account for 34 (41.5%) of appendicitis followed by farmers 23 (28%). Abdominal pain (100%), vomiting (79%) and nausea (81%) were the main complaints of appendicitis. Half of patients had a body temperature of >= 37.5 c 41 (50%) and the rest < 37.5 ℃. Acute appendicitis (simple) contributes 85.4% and high in 2nd decade, appendiceal abscess (6.1%) and perforated appendicitis accounts 8.5%. All appendicitis cases admitted to surgical were managed surgically of which 70 (85.4% were appendectomies followed by appendectomy with abscess drainage 6.1% and others were managed with appendectomy plus lavage. Twelve patients developed postoperative complications and surgical site infection was the leading 7 (8.5%) followed by pneumonia 3 (3.6%), two sepsis and one death following appendectomy plus abscess drainage (Table 2). The complication was within 5th and 6th decades and who comes after two days of illness.
Table 2: Prevalence and management outcome of appendicitis APH in the year of January-September, 2018. View Table 2
The second common cause of non traumatic surgical acute abdomen in patients admitted at APH surgical ward was intestinal obstruction 48 (28%). 27 (56.25%) of obstruction occupied by those age greater than 45 years and 62.5% were farmers. Males were 61.9% and females were 38.1% and male to female ratio was 1.6:1. Most of the patients were from rural area 38 (79%).
The leading cause of intestinal obstruction was small bowel obstruction 30 (62.5%) and adhesion/band were 13 (43%) of which 94.9% had history of abdominopelvic operation and nine primary volvulus, five hernias and three intussusceptions contributed 57%. Abdominal pain (100%), vomiting (96.6%) and abdominal distension (84%) were the common presentations. 20% of patients were in hypotension, tachycardic (48.3%) whereas 36% were febrile To >= 37.5 c. Abdominal distension was the commonest physical finding (78%) followed by tenderness (62%). 60% of them comes within 48 hrs of illness and 45% > 48 hrs with mean duration of presentation = 2.54 days. Patients managed surgically for small bowel obstruction were 30 of which eleven laparotomy plus resection and anastomosis were done, eight laparotomy and adhesion release done for adhesion, six laparotomy and reductions done for two intussusceptions and four incarcerated hernia. There were no postoperative complications following SBO but one death.
Large bowel obstruction contributes 18 (37.5%) from total bowel obstruction. The leading causes of large bowel obstruction were sigmoid volvulus 14 (77.7%), ileosigmoid knotting 3 (16.7%) and there was one colorectal cancer. Males were 61% and females 39%. 61% of patients were in >= 45 years of age group and male to female ratio was and 1.4:1. Most of the patients were from rural (94%). The four main complaints were abdominal pain (100%), abdominal distension (97%), constipation (97%) and vomiting in 67% and only 32% of patients were in hypotension (BP < 90/60 mmHG), 59% tachycardia and 50% were febrile (To >= 37.5c). Abdominal tenderness was the commonest physical finding (100%) next distension (97%).The mean duration of illness presentation was 2.84 days. Sigmoid volvulus was the commonest cause of which 100% were managed surgically of which six end colostomy were done for two gangrenous sigmoid volvulus, three gangrenous ileosigmoid knotting and one colorectal cancer. Ten primary resection and end to end anastomosis for sigmoid volvulus and two derotations were done. There were eight complications (two wound site infections, three anastomosis leaks, two pneumonia cases). The mean of hospital stay after management was 11.23 days. Four out of the 18 patients with large bowel obstruction had died giving a mortality rate of 22% (Figure 2).
 Figure 2: Common clinical symptoms and signs among surgically treated patients in ACH from January to September 2018. View Figure 2
Figure 2: Common clinical symptoms and signs among surgically treated patients in ACH from January to September 2018. View Figure 2
Peritonitis was the 3rd common cause of non traumatic surgical acute abdomen which accounts 41 (24%). Perforated appendicitis was the leading cause of peritonitis 20 (46%) followed by gangrenous SBO 9 (22%) followed by gangrenous large bowel 7 (17%) and perforated peptic ulcer disease 6 (15%). Males were 22 (53.6%) with ratio of 1.2:1. Perforated appendicitis was common in lower extreme age i.e. less than 14 years contribute 54% of all peritonitis secondary to perforated appendix. 30 (73%) were rural and others from urban. Students were the leading group 17 (41.5%) followed by farmers 11 (27%). Abdominal pain was the common symptom (100%) then vomiting (78%) and on examination 100% of them have abdominal tenderness and guarding. 25 (60%) were in hypotension state and 94.3% were tachycardic, 42.5% were febrile. Majority of cases (78%) of cases were those who came after 48 hrs of illness before management. All are managed surgically, 19 appendectomies and lavage, 15 resection and end to end anastomosis, 6 simple omental patches and one laparotomy and end colostomy. There were twelve patients who develop postoperative complications of which the six were sepsis, five surgical site infections and pneumonia one. There were seven deaths due to sepsis after they were managed for gangrenous bowel obstruction and perforated PUD. Mean of post management hospital stay was 9 days. Death rate following peritonitis from total surgically treated non traumatic acute abdomen was 4.6%.
Using bivariate analysis, age, sex, residence, patients' complaint of abdominal distension and constipation, duration of illness before operation (in days), signs of guarding and abdominal distension, blood pressure, temperature, types of diagnosis, length of hospital stay and post-operative complications were significantly associated with patients' management outcome (Table 3).
Table 3: Bivariate logistic regression analysis of management outcome of surgically treated non traumatic acute abdomen in APH, January 2018-September 2018. View Table 3
Numerous associations were found to be significant in the bivariate analysis. Therefore, a multivariable approach was applied to determine which factors best explained and predict management outcome of patient. All explanatory variables showing significant association with dependent variable were analyzed using multivariate logistic regression model to avoid the possible confounding variables. As a result, age, sex, duration of illness before operation, body temperature and post operation complications were significantly associated with patients' management outcome (Table 4).
Table 4: Multivariate analysis on factors associated with favorable outcome among surgically treated patients at ACH in 2018. View Table 4
• Therefore, those patients whose age group less than 24 years had six times more likely to be improved compared to patients who are in the age group greater than 55 years (AOR: 6; 95% CI: 1.1, 31.1 ).
• Those who were presented less than 48 hrs of illness before operation had 5.7 times more likely to be improved compared to those presented after 48 hours (AOR: 5.7; 95% CI: 1.5, 22.2, p = 0.012).
• Those patients who did not developed postoperative complications were 5.6 times more likely to be improved compared to who had complications(AOR: 5.6; 95% CI: 1.5, 20.5, p = 0.010).
Out of 171 surgically treated NTAA admissions, hospital mortality was 9.35% and postoperative complication rate of 17%. Almost 41% of patients who developed postoperative complication died. The most common causes of death was sepsis (62.5%) followed by anastomosis leak (25%) and 81.5% of deaths were in patients who arrived at the hospital after 48 hrs of illness. Peritonitis was the most common diagnosis 8 (50%) of patients associated with mortality followed by intestinal obstruction 7 (43.75%) while acute appendicitis (simple + complicated) accounted 1 (6.25%) of post-operative mortality. 61% of death was in the age group >= 45 years that indicated high mortality in high extreme of age.
Within nine months study period (from January up to September 2018 G.C), there were 192 non-traumatic surgical acute abdomen cases admitted in Attat catholic hospital surgical ward of which 171 were treated surgically. The age ranged from 1 to 69 years with a mean age of 31.46 years. Majority of patients were in their 2nd and 3rd decades of life which was similar with the studies done in tertiary hospitals in India, Kigali teaching hospital, and other institutions [10,14,21]. Young age was significantly associated in our study (AOR: 6; 95% CI: 1.1, 31.1) i.e. age less than 24 years had 6 times more likely to have good outcome compared to >= 55 years which is similar to a study done in Nekemte Referral Hospital. In their study, patients who were < 14 years of age were 15.4 times more likely to have good management outcome as compared with other age group [AOR = 15.4, 95% CI (1.61-19.98)]. Older age also was significantly associated with mortality (p = 0.006) in Gondar university hospital [16]. This is explained by decreased functional reserve of main organs and co-morbidity in old age groups. But age didn't show any association in Kigali teaching hospital and other some institutions [14].
The duration of illness before operation ranges from 01 day to 9 days with mean of 3.54 days and 75 (43.9%) of patients came within 48 hrs of illness while 96 (56.1%) came after 2 days of illness. This was statically significant in our study that those who presented within 2 days of illness were more likely to be improved (AOR: 5.7; 95% CI: 1.5, 22.2, p = 0.012) and is similar with the study in Nekemte referral hospital that patients who had > 2 days of illness have 3.8 times more likely to have unfavorable outcome as compared to patient who came with < 2 days of duration [(AOR = 4.33, 95% CI (1.03-18.12). In Kigali teaching hospital that showed duration of symptoms on admission was (mean = 3.6 days) and majority (64.2%) of the patients presented to the hospital more than 48 hours after the onset of symptoms and in Wolaita Sodo Teaching and Referral Hospital (WSUTRH), in 2015 that showed 63.3% presented after 48 hrs [14,21] but duration of illness before operation had no association in Kigali teaching hospital.
The three top causes of acute surgical abdomen were acute appendicitis accounting 82 (48%) followed by bowel obstruction 48 (28%) and Peritonitis 41 (24%). This agrees with the findings in Tikur Anbesa Specialized Hospital, Goba referral hospital and Mekelle hospital. But contradicted with studies done in Kigali University Teaching Hospital and University of Ilorin Teaching Hospital (UITH), Nigeria which the primary causes was peritonitis while intestinal obstruction was the leading in Gondar, Wolaita Sodo Teaching and Referral Hospital [9,11,14-16,22]. This may be explained by due to diet and socio-economic factors that may or may not differ in different areas.
Appendicitis was found to be the leading cause of acute abdomen (48%). This agrees with study done in Goba referral hospital (49.2%), Tikur anbesa (52%), Saudi Arabia, this is in contrast to the study done clinical study of acute abdomen and management in India that showed peritonitis was the leading cause [1]. In this study, twelve patients developed postoperative complications and surgical site infection was the most common postoperative complication of appendicitis 6 (7.3%) followed by pneumonia 3 (3.6%) and one death (0.5%).
Intestinal obstruction was the next most common cause of non-traumatic surgical acute abdomen with 28% of which 30 (62.5%) small bowel obstruction followed by large bowel obstruction 18 (37.5%), similar with the studies done at in Tikur Anbesa Specialized Hospital, Goba referral hospital and Nekemte referral hospital [10,11,15] but in contradict to studies done at Gondar University Hospital and Wolaita Sodo teaching hospital that shows the second common cause was intestinal obstruction [16,23]. The leading causes of small bowel obstruction in this series were adhesion/band accounts (43%) followed by primary volvulus. This is in agreement with other studies done at tikur anbesa specialized hospital and Goba referral hospital [11,15] but contradicts with studies done at Adama and Nekemte referral hospitals [1,10] which had shown that intussusceptions (in 30.9% of the cases) and Primary small bowel volvulus (in 57.33% of small bowel obstruction respectively [7,10].
Peritonitis was the third cause of non-traumatic surgical acute abdomen in this series 41 (24%) of which perforated appendicitis was the leading 20 (46%) followed by gangrenous SBO 9 (22%) followed by gangrenous large bowel 7 (17%) and perforated peptic ulcer disease 6 (15%). This is in agreement with the study done in suhul general hospital [9]. But contrarily, study on nekemte referral Hospital, showed that, 12.2% of patients developed peritonitis, among which 42.59% resulted from gangrenous bowel obstruction, 20.37% from perforated appendix and 12.96% from perforated peptic ulcer disease [10]. Like the study done in Nekemte referral hospital [10], peritonitis was highly seen in patient who came late (70.7%) in > 2 days of illness before operation.
The total complications after management were 17% which was similar with the study done in Mekelle and Nekemte Referral Hospital with a complication rate of 16.9% and 16.10% respectively [9,10] and contradicts to Tikur anbesa specialized hospital and Suhul general hospital which was 28% and 20.5% respectively. The commonest early postoperative complications other than death were wound infection (7.6%), sepsis (7%) and pneumonia (4.1%) which is low when compared with studies done in Gondar University Hospital i.e. wound infection (20.6%), sepsis (17.6%) and pneumonia (9.9%). This may be due to better service at ACH after patients arrived. Postoperative complication were significantly associated with management outcome in our study (AOR: 5.6; 95% CI: 1.5, 20.5, p = 0.010) i.e. those who did not developed postoperative complication had 5.6 times more likely to improved which is similar to a study done in Tikur anbesa specialized Hospital that mortality was significantly higher in patients who developed post-operative complications (p < 0.0001).
The overall mortality rate of surgically treated non-traumatic acute abdomen was 9.35% which is lower than the study done in Tikur anbesa specialized hospital (18.6%) and Goba referral hospital 2017 (16%) but higher than the study done in Mekele and Nekemte referral hospitals which had shown 2.4% and 3.05% mortality rate respectively [9,10,15]. In this study, 81% of death was secondary to sepsis and 61% in higher extreme age group with mean age of the expired patients (43.5 years). Most of patients who died were managed for generalized peritonitis following perforated appendix followed by large bowel obstruction and perforated PUD. Eighty two percent of all deaths were those patients who were presented after 2 days of illness before operation (mean 3.6 days) which was similar to the study done in Nekemte referral hospital (66%) and Gondar university hospital [10,11]. The remaining death was secondary gangrenous small bowel obstruction and appendiceal abscess.
In this study we noticed emergency surgical operation for non traumatic acute abdomen particularly for acute appendicitis was found to be the most common surgical emergency operations performed in ACH. Non traumatic surgical acute abdomen was more common in rural dwellers and male sex. The common causes of NTAA were acute appendicitis found followed by intestinal obstructions and peritonitis. Most patients were relatively young, in the 2nd and 3rd decades of life. Longer duration of illness before intervention, age and postoperative complications were statistically significant. Over all postoperative complication was high with wound infection and sepsis predominance.
Late presentation of patients before intervention, pre and postoperative complications, peritonitis and gangrenous large bowel obstruction were the commonest cause of patients' bad outcome. The overall mortality found in this study was relatively high compared with some studies in Ethiopia even if it is lower in some areas.
• Attention should be given to high extreme of age patients as mortality is high in this age group.
• Since wound infection and sepsis were the commonest postoperative complications that lead to death, infection preventions in Attat Catholic Hospital is crucial.
• As most of the complicated cases with delayed presentation are from rural areas, another study about the acute abdomen in the community is helpful.
• It might not representative for Gurage zone population since it is institutional based.
• This study May not show long term complications.
Our special thanks go to Jimma University graduate study. We also would like to thank study participants, data collectors and supervisors.
No conflict of interest declared by authors.
Jimma University funded this study.
Data is available on the request.