The acute phase of Chagas disease can occur at any age, however the pediatric population is usually the most affected (from one to 15 years), so it is very important to detect and treat it as soon as possible to try to eliminate the circulating parasite.
The main objective of this research is to present the first seroepidemiological study of the infection by Trypanosoma cruzi, carried out to students of school age of both urban and rural primary schools in the State of Querétaro and at the same time, the validation of an enzyme excreted by the hemoflagellate parasite, Superoxide Dismutase (SODe), as an adequate molecular marker.
In this study, a total of 540 sera collected between February 2015 and May 2016 were evaluated through ELISA and Western blot tests using the marker excreted as an antigenic part, in an ELISA-SODe and a WB-SODe.
Of the total of sera studied 106 (19.6%) gave reactivity. Of these, 99 sera were reactive against ELISA-SODe (prevalence of 18.3%), whereas 100 sera were reactive for WB-SODe (prevalence of 18.52%). The results of the two applied tests were evaluated and compared, using the Western blot technique, as gold standard, to find that the sensitivity and specificity of ELISA-SODe reach respectively 93% and 99%.
Our study provides seroepidemiological data on the presence of chagasic infection in the pediatric population of rural and urban areas in Santiago de Querétaro and, at the same time, we confirm that the SODe excreted by Trypanosoma cruzi is highly immunogenic, which indicates it as an excellent tool for the early diagnosis of Chagas disease.
Trypanosoma cruzi, Superoxide dismutase, Immunogenic, Pediatric population, Rural, Urban
American trypanosomiasis is recognized by WHO as one of the 17 neglected tropical diseases in the world. Caused by the hemoflagellate parasite Trypanosoma cruzi, which in its natural form is transmitted by vectors of the order Hemiptera (Bugs), family Reduviidae, subfamily, triatominae and triatoma genus, and by non-vector mechanisms, such as blood transfusions, organ transplants, transmission orally and vertically from mother to child [1,2].
The Pan American Health Organization [3] estimates that there are currently 7.7 million people infected with T. cruzi in 21 endemic countries, with 41,200 new cases per year, and 14,400 children born annually with congenital Chagas disease. The most affected countries are: Bolivia (6.8%), Argentina (4.1%), El Salvador (3.4%), Honduras (3.1%), Paraguay (2.5%), Guatemala (2%), Ecuador (1.7%), French Guyana, Guyana, Suriname (1.2%), Venezuela (1.2%), Nicaragua (1.1%) and Brazil (1%), Panama, Peru, Mexico, Belize, Venezuela, Costa Rica, Chile and Paraguay [4].
Mexico, according to the official figures of the World Health Organization (WHO), estimates that 1.1 million people are infected with the trypanosome, and according to Hotez, et al. [5] in their research has recorded an estimate of 1-6 million infected.
The disease is considered a serious public health problem mainly in rural areas of Mexico, Central and South America. Migration has been an important factor, since there are currently cases reported from Latin America, which have been detected in the US, Europe, Japan, Australia. This is in addition to the enzootic transmission of Trypanosoma cruzi, which involves several species of mammals and vectors, some of them mention raccoons, opossums and especially domestic dogs [5,6].
Therefore, it should be considered that the acquisition of the trypanosomatid infection is not limited to rural areas, since in México, Peru, Bolivia and Venezuela cases have been reported in urban and peri-urban areas [7].
The State of Querétaro is not officially considered as an endemic area of the infection; The obligatory tests of ELISA are carried out only in blood samples from patients coming from risk areas and in reactive cases, confirmatory tests are not carried out. The above, added to the central location of the state of Querétaro, leads to a constant leakage of individuals from other states, previously transfused, or infected, ignoring whether their blood is contaminated or not, they are offered for blood donors. In 2005, the State Center for Blood Transfusion (CETS) reported 0.3% of HIV-positive Trypanosoma cruzi in its blood donors. By not having reliable statistical data to help quantify the real situation of endemic areas, Villagrán and collaborators in that same year, began a seroepidemiological cross-sectional study in 23 communities of 11 rural municipalities in the State of Querétaro. Collecting 1029 blood samples from the general population to which 4 conventional tests were applied, obtaining a seroprevalence of 6.2%, to two reactive tests, which compared to the national average of 1.6% obtained by Guzman-Bracho, et al. [8] in 2001, it exceeded by 5 times the percentage reported and by far the data contributed by the state CETS of 0.3%.
Today, the main form of infection in the rural area is not vector transmission, since the congenital transmission (transplascentary), has far exceeded the bite of the bug. In Mexico, the first case of neonatal Chagas was reported in 1998 and the following case was reported in 2012 by Jiménez Cardoso, et al. [9] who detected an average of 4.08% of specific antibodies against T. cruzi in infants of seropositive mothers in states such as Oaxaca and Jalisco.
The diagnosis of Chagas disease depends on the stage in which the disease is present in the patient and can be performed by direct techniques (visualization of the parasite in the peripheral blood), xenodiagnosis or indirect (immumological tests), and the reaction in polymerase chain. (PCR) as a last resort, 100% sensitive and specific. Due to the high costs of PCR, it is not possible to keep it viable in most clinical laboratories, in addition, the lack of protocols to standardize, the best products to amplify, the sensitivity can vary from 45% to 96.5%, therefore, false positives can be obtained [10-12]. On the other hand, the WHO [13], states that two serological tests must be performed other than the serum of a probable Chagasic case, if both are reactive, the individual is considered positive, however if one of two is negative, you must perform a third immunological test. The above reflects that the diagnosis of this disease is expensive and is beyond the reach of the population that suffers the greatest risk of acquiring it, so it is important and necessary to seek and find new reliable diagnostic tools. Many studies tend to define a specific antigen of T. cruzi that would increase the specificity and sensitivity of the serodiagnosis. A possible candidate could be the Superoxide Dismutase of iron excreted by T. cruzi (Fe-SODe or SODe), which, in previous studies, has shown to have highly specific immunogenic properties, which make it a useful, unique tool to diagnose the disease in a population from or not from an endemic area [14-17].
The epimastigote forms of Trypanosoma cruzi (MHOM/ME/2006/H-4) were cultured in axenic medium. Liquid medium for trypanosomes (MTL, Gibco) supplemented with 10% heat inactivated bovine fetal serum at 28 ℃ in Falcon flasks according to Longoni, et al. [18] was used.
Random visits were made in several primary schools in three rural areas and two in the urban area of the State of Querétaro (Mexico).
Being a cross-sectional and longitudinal study, we are guided by the seroprevalence obtained in previous investigations with the general and adult population, in the chosen areas. Public elementary schools were chosen from localities already studied and considered endemic, in addition to meeting the pediatric age limit of 18 years (According to the Ministry of Health). The minimum number of school population in each school is 200 children, and maximum of 500, so that the N real (number of real samples) of work, will be the number of surveys with the informed consent delivered and signed by the parents of family who authorize the study to be carried out on their children. The statistical program Epi-info version 2, Statcalc module, was of great help, considering an expected serological prevalence of 6.2%, for the study conducted in 2009 in rural communities and an unexpected frequency of 9%.
Initial interviews were scheduled with school principals and parents of children, where information about the importance of the study was presented. Epidemiological surveys and informed consent signed by parents authorizing research in their children and filling out the surveys with all the relevant data of their children before their examination.
The number of blood samples per rural location was as follows: Community of El Gallo, 77, (1 to 77), San Vicente Ferrer, 106, (78 to 183) and San Ignacio, 111, (335 to 445), each one of them with 1,839, 1,525 and 871 inhabitants respectively. The selected communities belong to the municipalities of El Marqués, Colón and Huimilpan, respectively. Regarding the urban area of the municipality of Querétaro, the total blood samples obtained were 244, (184 to 540). This municipality has a population of 626,517 inhabitants.
A total of 540 sera (collected from February 2015 to May 2016) were evaluated, which were not grouped in any classification category (they were only numbered from 1 to 540).
The protocol designed for the research was submitted to the Bioethics Committee of the Faculty of Medicine of the Autonomous University of Querétaro, which approved it without any observation.
A sample of 5 ml of blood was extracted from the ulnar vein of each infant, using test tubes (Vacuttainer, Beckton-Dickinson). The serum samples were kept at 4 ℃ until the diagnostic tests were applied. We worked with a negative control serum, obtained from 20 healthy humans, who had not received blood transfusion, nor organ transplantation, nor had lived in a country endemic to Chagas disease. These samples were obtained in the CETS (State Blood Transfusion Center) in the State of Querétaro.
Cell culture: As a biological material for the study and characterization of SOD, epimastigote forms of Trypanosoma cruzi, of the Cali strain, of Colombian origin, were used and perpetuated by consecutive reseeding in the laboratory. This strain has remained infective, inoculating it every six months to a golden hamster from Syria (Mesocricetus auratus), recovering after a period of twenty days highly infective trypomastigote forms, which were again adapted to culture.
The parasite was cultured in vitro at 27 ℃ in Cellstar ® tissue culture flasks (Greiner Bio-One®), using Grace's Insect Medium (Gibco®) supplemented with 10% V/V of fetal bovine serum (SBF, PAA ®), previously inactivated by heating (56 ℃, 30 min) to a growth density (estimated by counting in a hemocytometric count chamber of Neubauer®) of approximately 107 cells/mL. The flagellates were collected by centrifugation (1500 g/10 min) in the exponential phase of growth, following the methodology described by [19]. The sediment or pellet thus obtained was resuspended in Grace's medium not supplemented with SBF and cultured in the same conditions for 24-36 h, time after which the trypanosomatids were again collected by centrifugation, decanting the supernatant and keeping separately both fractions (S1 and P) for the purification stages.
Preparation of cellular extract: The fractions resulting from the centrifugation (S1 and P) were processed independently in order to purify both the total SOD activity and the excreted SOD (SODe), respectively.
First, the flagellates pellet obtained (around 0.5-0.6 grams wet weight) was subjected to a lysis or cell breakage process. For this, once the remains of the culture medium were eliminated by means of two washes with phosphate buffer (phosphate buffer saline, pH 7), said sediment was resuspended in 3 mL of buffer buffer STE Buffer 1 (250 mM sucrose, 25 mM Tris-HCl pH 7.4 and 1 mM EDTA) and cold sonicated in three cycles of 60 V and 30 s (with intervals of 1 min between cycles).
Purification of SOD: The sonicate was centrifuged (2500 gravities/10 min/4 ℃) to discard the remains of membranes and dead cells, obtaining a new supernatant that we call Homogenate (fraction H).
In parallel, the initial supernatant (S1), which contains the cell excretion products, was filtered in order to retain the residues that have escaped the centrifugation using a 0.2 μm pore size microfilter (Minisart®, Sartorius®) (Fraction F).
Subsequently, parasites in MTL medium without fetal serum were cultured for 24 hours; the supernatant was collected by centrifugation at 600 gravities for 10 minutes and then passed through a 0.45 μm pore filter and solid ammonium sulfate was added. The protein fraction, which precipitated between 35% and 85% salt concentration, was centrifuged (9000 gravities for 20 min at 4 ℃), dissolved in 2.5 ml of 20 mM potassium phosphate buffer (pH 7.8) containing 1 mM EDTA and desalted on a Sephadex G -25 column (Pharmacia, PD10), previously balanced with Buffer 2, bringing it to a final volume of 2.5 mL (SODe fraction) [20].
The fraction obtained from SODe was used as an antigen in the ELISA and Western Blot assays. The protein content was determined using a Bio-Rad test, based on the Bradford method (Sigma-Aldrich, St. Louis, M.O.), with bovine serum albumin as a standard.
The purified protein fraction (SODe) at a concentration of 1.5 μg was coated onto polystyrene microtiter plates (Nunc, Denmark) in carbonate buffer (pH 8.2) for 2 hours at 37 ℃. The antigen stuck on the plate was removed by washing three times with PBS-Tween 20, 0.05% (washing buffer). The free adsorption sites were taken by incubation (2 hours at 37 ℃) with blocking buffer (PBS-Tween 20, 0.2%, BSA 1%). Once washed as described above, the plates were incubated (45 minutes at 37 ℃) with a serum dilution of 1/80 in wash buffer. After a second wash, the plates were incubated in the dark for 20 minutes with 100 μL of an antibody conjugated with enzyme (anti-IgG human peroxidase, Sigma) at a dilution of 1:1000. The reaction of the enzyme was catalyzed by the application of the chromogenic substrate OPD (o-phenylenediamine dihydrochloride, Sigma) and 10 μL of 30% H2O2 in 25 mL for 20 minutes in the dark. The reaction was then stopped by the addition of 50 μl of 3N HCl.
Absorbance was read at 492 nm in microplate reader (Sunrise, TECAN). All samples were analyzed in triplicate in polystyrene microtiter plates. The mean and standard deviations (SD) of the optical densities of the negative control sera (20 healthy humans) were applied to calculate the cut-off value (mean + 3 × SD) [15].
The SODe antigen fraction (at a concentration of 1.5 μg protein) was in IEF 3-9 gels and then transferred to a nitrocellulose membrane (Hybond C Extra, Amersham Pharmacia Biotech) using the Phast-Transfer kit, as described by the manufacturer (Phast-System Manual). The membrane was blocked for 2 hours at room temperature using 0.4% gelatin and 0.2% Tween 20 in PBS, followed by three washes, using 0.1% Tween 20 in PBS solution (PBS-T) and incubated for 2 hours at room temperature, with donor serum at a 1/100 dilution. Before washing, the membrane was further incubated for 2 hours at room temperature with the second antibody, anti-human immunoglobulin G (Fc-specific) peroxidase conjugate (Sigma Immunochemical, 1/1000 dilution). After washing as indicated above, diaminobenzidine (0.5 mg/ml in 0.1 M Tris/HCl buffer, pH 7.4, containing 1/5000 H2O2 [10 v/v]) was added and the reaction stopped with several washes in distilled water [15].
The results obtained in the serological study for each chosen variable were processed in the Excel Program for the elaboration of the Tables. For the statistical correlation between the ELISA-SODe and WB-SODe tests, the SPSS version 11.5 program for Windows was used, calculating the parameters of Sensitivity, Specificity, Negative Predictive Value (NPV), Positive Predictive Value (PPV), Index of Kappa and Concordance Percentage.
Of the total of 540 children samples analyzed with the ELISA-SODe and WB-SODe techniques, 106 were reactive to one or another test, 99 for ELISA-SODe for T. cruzi (18.3%) and 100 reactive sera for WB-SODe (18.52%) (Table 2).
Table 2: Relationship of reactive sera from pediatrics (rural and urban population) of Queretaro (Mexico) by ELISA and Western Blot using SODe antigen fractions of T. cruzi associated with age and gender. View Table 2
The SPSS program, version 11.5, showed a sensitivity of 94%, specificity of 98%, PPV was 98% and NPV was 98%. The Kappa index presented a value of 0.95, which confirmed the agreement, between both tests, ELISA-SODe and WB-SODe (Table 3).
Table 3: Evaluation of the reliability to detect T. cruzi antibodies, using ELISA technique with SODe CRU antigen, in 540 sera of children from the state of Queretaro (Mexico). The values given are estimated with Western Blot as the comparator. View Table 3
The concordance between the two tests (ELISA-SODe and WB-SODe) established the positivity of 93 children, a prevalence of 17.22% of the total population. In the analysis of the results on the prevalence of the samples coming from rural and urban areas, it only showed a slight difference; Infection rates were higher (18.58%) in rural areas than in urban areas (15.98%) (Figure 1).
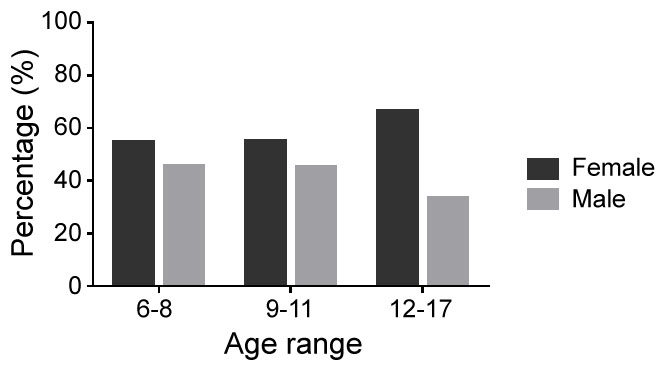 Figure 1: Percentages of positive sera in rural and urban pediatric population by gender in Queretaro, Mexico. The data were analyzed by Chi-square test.
Figure 1: Percentages of positive sera in rural and urban pediatric population by gender in Queretaro, Mexico. The data were analyzed by Chi-square test.
Odds ratio = 0.9213. 95% Confidence interval 0.6563 to 1.293. View Figure 1
By age groups, in the total population studied, the prevalence of age range of 6 to 8 years was 20.08% and 9 to 11 years of 17.6%, and 13.04% of children aged 12 to 17 years. In rural areas, groups of children aged 6 to 8 years presented 21.2% seroprevalence, the group of 12 to 17 years, 13.04%. The results of the urban areas were reversed in comparison with the rural areas, where the groups with the highest values were those with ages of 12 to 17 years (18.2%), (Table 1) while children aged 6 to 8 years showed a lower seroprevalence of 14.3%.
Table 1: List of sera studied in rural and urban pediatric population of the state of Querétaro (Mexico), by location, gender and age. View Table 1
The prevalence was slightly higher in women, 18.0% versus 16.6% in men in the total population. Therefore, no significant differences were observed by gender in the rural and urban areas that have the highest seroprevalence in women of 19% and men of 12% (Figure 2).
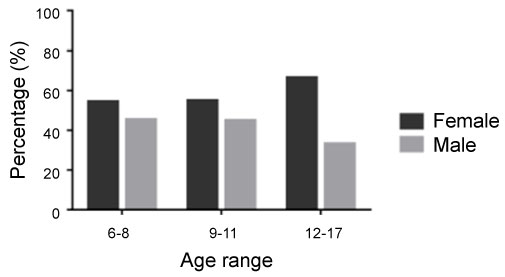 Figure 2: Percentages of positive sera of pediatric population by age range in males and females in Queretaro, Mexico. The data were analyzed by Chi-square test. Odds ratio = 0.9818. 95% Confidence interval 0.4152 to 2.321 in age groups 6-8 and 9-11. Odds ratio = 0.6000. % Confidence interval 0.1328 to 2.711 in age groups 6-8 and 12-17. Odds ratio = 0.6111. % Confidence interval 0.1337 to 2.794 in age groups 9-11 and 12-17. Software GraphPad Prism (version 6, GraphPad Software, Inc.). View Figure 2
Figure 2: Percentages of positive sera of pediatric population by age range in males and females in Queretaro, Mexico. The data were analyzed by Chi-square test. Odds ratio = 0.9818. 95% Confidence interval 0.4152 to 2.321 in age groups 6-8 and 9-11. Odds ratio = 0.6000. % Confidence interval 0.1328 to 2.711 in age groups 6-8 and 12-17. Odds ratio = 0.6111. % Confidence interval 0.1337 to 2.794 in age groups 9-11 and 12-17. Software GraphPad Prism (version 6, GraphPad Software, Inc.). View Figure 2
Due to the high incidence of Chagas disease in a wide variety of nearby endemic areas surrounding Querétaro, such as Hidalgo, Michoacán, Guanajuato, San Luis Potosí and even the State of Mexico, (Figure 3), and the internal risk posed by humans and other mammalian species to act as natural reservoirs of T. cruzi, it is of the utmost importance that appropriate prevention measures are provided in the populations most at risk. It is crucial to keep updated the techniques of diagnosis and it is vital to develop highly sensitive and specific diagnostic methods to provide the appropriate treatment and in time, to reduce transmission of any kind.
 Figure 3: Map of the state of Querétaro. The municipalities studied and neighboring states are indicated, whose seroprevalences estimated by various studies were shown as endemic to Chagas disease. View Figure 3
Figure 3: Map of the state of Querétaro. The municipalities studied and neighboring states are indicated, whose seroprevalences estimated by various studies were shown as endemic to Chagas disease. View Figure 3
In this sense, the present study proposes a confirmatory approach, since the use of the enzyme SODe used as antigen in ELISA and Western Blot, is highly effective for diagnose T. cruzi infections in human populations living in endemic areas of the disease.
In addition, the presence of false positives with the ELISA technique may be due to cross reactions with other protozoa, mainly with T. rangeli and with species belonging to the genus Leishmania spp, among others. This is a serious inconvenience for patients from geographical areas that harbor other infectious agents.
The FeSOD enzyme has been identified in several protozoa as: Plasmodium spp [21] Acanthamoeba castellanii [22], Entamoeba histolytica [23], Toxoplasma gondii [24], Trichomonas vaginalis [25].
Mateo and collaborators in 2008, purified and characterized four SOD isoforms present in T. cruzi, one of them, with Isoelectric Point (IP) around 3.8 and Molecular Weight around 25 kDa [26]. Subsequently, the same authors showed that this isoform excreted by the parasite had immunogenic characteristics, so when used as an antigen in ELISA and/or Western Blot tests, it showed that it does not cross react and that it is specific to genus and species or to other trypanosomatids [11,15,17].
The evaluation of the results obtained with the total sera analyzed with the ELISA-SODe technique and the WB-SODe technique was corroborated with previous studies, whose values of specificity and sensitivity were very good. López-Céspedes and collaborators in 2012, conducted a cross-sectional study in adults of the suburban area of the municipality of Querétaro, obtaining a seroprevalence of 11%. Villagrán, in 2005, initiated the study with the SOD, using it to detect anti-Trypanosoma cruzi antibodies in serum samples, from the general population of endemic communities up to that time, from the same state, with 8.16% seroprevalence, later, in 2009, a serological study was carried out with known conventional tests and a statistical evaluation was carried out among the same tests applied. And finally in 2014, a comparison was made between conventional tests already known and SODe, in sera from rural communities that had not been studied and only in the pediatric population.
The high rate of infection detected in children in rural areas may be the result of congenital transmission and/or high vector exposure. The results of urban areas compared to rural areas, the age group of 12 to 17 years, resulted in higher values. These percentages can be attributed to the cumulative and prolonged exposure to infected vectors, which increases with age. There is no significant difference in the results by age and gender in rural and urban areas.
The prevalence in urban areas was significantly higher in women according to what was reported by other authors in their research in Puebla, Puebla [27], and in Tamazunchale, San Luis Potosí [28]. These preliminary data revealed the degree of infection by Trypanosoma cruzi in urban areas of our country.
The authors thank the parents and principals of the elementary schools, who kindly allowed us to enter their classrooms to take blood samples from their students to conduct the research. To Dr. Manuel Sánchez Moreno, head of the Molecular Biology of Parasites, of the Faculty of Sciences of the University of Granada. Spain, that we opened the doors of your laboratory to perform tests with Superoxide dismutase, and we would like to express our gratitude to E. Guerrero López for the technical assistance in the preparation of the culture media.
Cuerpo Académico UAQ-CA-97 Investigación Clínica Molecular. PRODEP.