Dengue fever is one of the most important emerging infectious diseases constituting important contribution in global burden of disease. Platelet transfusion is required in the patients when they develop Dengue Hemorrhagic Fever (DHF) or thrombocytopenia below 20,000/cu.mm without hemorrhage. Serial platelet counts are used to monitor the patients. In this study we investigated whether Mean Platelet Volume (MPV) could be used as a tool to predict development of significant thrombocytopenia, DHF and Dengue Shock Syndrome (DSS). This may help in triage of high-risk patients and readiness of the care-givers for platelet transfusion when required.
In this prospective study done in IIMSAR, Halides, 100 cases of dengue were included. In those patients who developed thrombocytopenia < 20,000/cu.mm, the MPVs prior to development of this significant thrombocytopenia, were compared with the mean of the MPVs of all the patients under the study. Statistical analysis was done using t-test.
On the previous day on which platelet count was < 20,000/cu.mm, mean MPV was significantly low (p value < 0.0001) compared to the mean of MPVs of all the patients.
Serial MPV monitoring can be used to predict significant thrombocytopenia.
Dengue, Dengue hemorrhagic fever, Dengue shock syndrome, Mean platelet volume, Predict, Thrombocytopenia
DHF: Dengue Hemorrhagic Fever; DSS: Dengue Shock Syndrome; MPV: Mean Platelet Volume; PC: Platelet Count
Dengue is one of the most important emerging infectious diseases, caused by a virus of the Flaviviridae family, incidence of which has grown dramatically in recent decades all over the world. The disease is now endemic in more than 100 countries in WHO regions of Africa, the Americas, the Eastern Mediterranean, South East Asia and Western Pacific. The America, South-East Asia and Western pacific regions are the most seriously affected [1]. Europe is also now under threat of the disease as waves of dengue outbreak have been reported from France, Croatia and some other countries since 2010 [2,3]. An estimate showed 3.9 billion people in 128 countries are at risk of infection with dengue virus at present [4].
Dengue is manifested clinically with fever, headache, retro-orbital pain, back pain and generalized weakness with or without nausea and vomiting. The disease may be complicated by bone marrow depression manifesting as thrombocytopenia of various degrees and leakage from blood vessels lined by functionally damaged endothelial cells, manifested as Dengue Hemorrhagic Fever (DHF) and Dengue Shock Syndrome (DSS). Production of inflammatory cytokines along with immune-mediated reactions are considered to be responsible for the development of these complications leading to fatality [5,6].
Serial hematocrit estimations and platelet counts are used to monitor closely the hospital-admitted patients, as increase in hematocrit may indicate plasma leakage and severe thrombocytopenia may be targeted therapeutically with platelet transfusion. Most of the guidelines for treatment of dengue advocated prophylactic platelet transfusion without hemorrhagic manifestations at platelet level 10,000-20,000/cu.mm [6]. Kumar, et al. also marked patients with platelet count below 20,000/cu.mm as high risk patients [7].
As in India dengue cases are on the rise, in the recent years the clinical laboratories have been getting a large number of blood samples of dengue patients for hematocrit estimations and platelet counts. In our personal experience of examining peripheral blood smears routinely for platelet count of these samples, it was noted that, in some patients, the volume of platelets decreased as the disease progressed and the platelet count diminished. After a certain period when there was an increase in the platelet volume in these patients, the platelet count also increased.
So, it was decided to undertake a study to see the association of Mean Platelet Volume (MPV) with platelet count and disease severity in dengue patients. If such a statistically significant relation really exists then it will be possible to predict severe thrombocytopenia or disease severity in advance which will ultimately lead to better patient care.
The specific objectives of the study were
• To investigate if alteration of MPV is significant in patients with significant thrombocytopenia in dengue.
• To investigate if MPV can be used as a predictor of significant thrombocytopenia in patients of dengue.
• To investigate if MPV can be used as a predictor of development of Dengue Hemorrhagic Fever and Dengue Shock Syndrome in hospital admitted patients of dengue fever.
This was a prospective study done at ICARE Institute of Medical Sciences and Research, Haldia (India) from August 2017 to November 2018. Patients who were admitted with fever, headache, body ache with or without chills and rigor, nausea, vomiting, retro-orbital pain and low back pain, were watched and the ones who were above 18 years of age and whose blood samples were found to be positive for NS1 antigen were selected for the study. Blood samples were tested for NS1 antigen by ELISA method which was based on the Direct Sandwich principle and the kit which was used was DENGUE NS1 Ag MICROLISA, manufactured by J. Mitra and Co Pvt. Ltd., New Delhi, India. Later infection with dengue virus was confirmed with dengue specific IgM antibody assay by ELISA which was also based on Direct Sandwich principle and the kit which was used was DENGUE IgM MICROLISA, manufactured by the same manufacturer. The patients who were reported negative for Dengue IgM were excluded from the study subsequently. Thus the study was done on adult patients found to be positive both for dengue NS1 antigen and dengue specific IgM.
Venous blood was collected in K3EDTA vial every day in the morning from each patient during their stay in the hospital and platelet parameters were measured by Sysmex XP100 automated hematology analyzer. Platelet counts were also matched with the peripheral blood smear examination under microscope. In a specially designed proforma, serial platelet counts and MPV were recorded against each patient. From these serial counts an average MPV was calculated for each patient. From these average MPVs a mean of the average MPVs of the 100 patients was calculated. The proforma also contained clinical information regarding development of DHF and DSS in each patient.
The patients were divided into two groups. One group had the patients in whom platelet count was < 20,000/cu.mm at any point of time and the other group had the patients who maintained platelet count > 20,000/cu.mm during their hospital stay. For each group a 'group mean' of MPVs was calculated from the average MPVs of the patients in the group. These two 'group means' were compared using two tailed t test.
From the collected data of the serial MPVs and platelet counts, a 'cut-off' MPV of each patient was established by taking the MPV of the previous day of the day when the platelet count was noted below 20,000/cu.mm. The mean of these 'cut-off' MPVs were calculated. This mean was compared with the mean of the average MPVs of the 100 patients under the study using one tailed t test.
Then the patients who developed DHF were taken in a group and another group was formed taking the patients who developed DSS. For each group, a 'group mean' of the MPVs was calculated from the average MPVs of the patients in that group. These two 'group mean' of the MPVs were compared separately with the mean of the average MPVs of the 100 patients under study using one tailed t test.
There were total 100 patients included in the study. Among them 30 patients developed thrombocytopenia below 20,000/cu.mm at any point of time. In the rest 70 patients platelet count was maintained above 20,000/cu.mm. 31 patients developed DHF. DSS was seen in 9 patients (Figure 1).
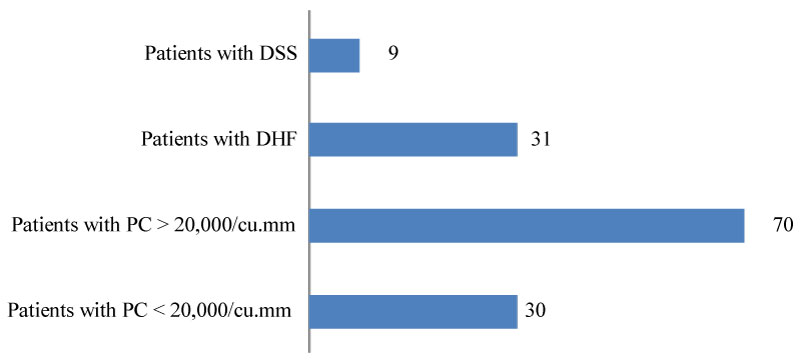 Figure 1: Number of patients with different manifestations.
View Figure 1
Figure 1: Number of patients with different manifestations.
View Figure 1
Mean of the MPVs of the total 100 patients was 10.9 ± 1.5 fl. 'Group mean' of the MPVs of the 30 patients who developed platelet count below 20,000/cu.mm was 9.7 ± 0.7 fl. 'Group mean' of the MPVs of the 70 patients who maintained platelet count above 20,000/cu.mm was 11.4 ± 1.5 fl (Table 1). When these 'group mean' of the MPVs were compared, p value was found to be < 0.0001 which was statistically significant.
Table 1: Mean MPV of different patient groups. View Table 1
In the group of 30 patients who had platelet count below 20,000/cu.mm, in two patients platelet count was below 20,000/cu.mm at the time of hospital admission. In the rest 28 patients gradual decrease in platelet count was observed during the hospital stay. In these 28 patients, on the day which was the previous day of the day when platelet count went below 20,000/cu.mm, mean MPV was 9.8 ± 0.8 fl. (Table 1). Compared to the mean of the average MPVs of all the patients under study, p value was < 0.0001, which was extremely statistically significant.
31 patients developed DHF. 'Group mean' of the MPVs of them was 9.8 ± 0.7 fl. Compared with the mean of the average MPVs of all the patients under study, p value was < 0.0001, which was statistically significant. Nine patients developed DSS. 'Group mean' of the MPVs was also found to be 9.8 ± 0.7 fl in this group. Compared to the mean of the average MPVs of all the patients under study, the p value was 0.0015, which was statistically significant.
In the past MPV has been evaluated for association with a number of conditions manifested with thrombocytopenia [8,9]. MPV depends on platelet diameter, if platelet diameter is increased MPV is also increased and vice versa. Increased diameter indicates increased production rate and also during activation platelet shapes change to biconcave discs to spherical leading to increased MPV [10]. In dengue infection cause of thrombocytopenia is said to be multifactorial, i.e, bone marrow hypoplasia [11] (leading to decreased proliferative capacity of hematopoietic cells [12]) and peripheral platelet destruction by increased apoptosis, activated compliment system and by anti platelet antibodies [13-15]. The marrow suppression can be indicated by low MPV [16]. Bashir, et al. reported that at initial stages of dengue fever MPV may fall [17]. They also found that MPV < 9 fl has strong association with dengue (sensitivity > 90%). Though this finding did not match our finding (Mean MPV in the present study was 10.9 + 1.5 fl), that may be due to geographical variation of normal reference values. (Mean MPV in Indian population is 11.2 ± 1.32 [18], whereas Mean MPV in healthy Sudanese population is 9.8 fl where Bashir, et al. did their study [19]). Similar fall in MPV in dengue patients was found by Navya, et al. [20], Hardeva, et al. [21] and Kanchana PVN, et al. [22].
Our study was aimed to investigate if there is significant change of MPV in different risk groups of dengue. Winwanikit V observed that MPV in DHF was not altered compared to healthy patients [23]. This was supported by findings of Dewi, who did not find significant difference of MPV between patient groups of DF, DHF and DSS [24]; Sharma K, et al. who observed no significant correlation of MPV with severity, serology and treatment outcome in dengue infection [25] and Prakash GM, et al. who found no significant difference of MPV with severity of disease [26]. Our study showed significantly decreased MPV in cases of DHF and DSS in comparison to the mean of the MPVs of all the patients, whereas Dewi and Sharma, et al. compared the MPV in between different risk groups. In the published work of Prakash GM, there was no DHF and DSS patient.
Another possibility for the difference in findings is, the strain of the dengue virus prevalent in the areas of these two studies (Indonesia and Jaipur, India) are different than the strains prevalent at the area of our study (Eastern coastal area of India); thus leading to different mechanisms of thrombocytopenia. Thrombocytopenia mainly due to bone marrow depression would be reflected as low MPV at initial stages of infection, whereas when the mechanism is mainly peripheral destruction of platelets, MPV may be unchanged or even increased [6,11-13].
The present study showed a significantly low MPV in patients with platelet count below 20,000/cu.mm compared to patients with higher platelet counts. Similar result was found by Mukker P, et al. in their retrospective observational study [27]. We found significant fall in MPV on the previous day of the day on which platelet count came below 20,000/cu.mm, thus indicating that the significant fall in platelet count may be predicted by looking at serial MPV.
Our study showed that in patients of dengue the MPV was significantly lowered in patients in whom platelet count came below 20,000/mm3. Serial MPV observation can be useful in predicting this significant platelet count level as lowering of MPV preceded reduced platelet count. Decreased MPV was also associated with complications such as Dengue Hemorrhagic Fever and Dengue Shock Syndrome.
The limitation of the study was small sample size and limited geographic area. Further large scale studies involving different geographic locations and data regarding the serogroups of the affecting virus are needed to fix the critical cut-off values of MPV for triage of high-risk patients. As reference values of MPV are different in different ethnic groups, a standard critical z-value can be fixed, taking data from different ethnic groups so that the caregivers can be cautious when MPV of a patient of dengue comes below that critical standard deviation level.
Approved by the Institutional Ethical Committee.
None.
Dr. Anupam Brahma conceived the presented idea that Mean Platelet Volume can be used to predict significant clinical outcomes in dengue. It was supported by Dr. Prasit Kumar Ghosh. Dr. Brahma, Dr. Ghosh and Dr. Utpal Goswami reviewed the published literature together and planned the study design. Data collection and analysis was done by Dr. Brahma and Dr. Ghosh. Dr. Goswami and Dr. Saswati Majumdar reviewed the analytical process. All authors discussed the final results and contributed the final manuscript.