Elderly patients have impaired physical function, which is further reduced by the incidence of hospitalization for heart failure. In these patients, nutritional status also deteriorates during hospitalization, which may cause impairment in their physical function. In this study, we repeatedly measured physical function using gait speed (GS) during hospitalization, and evaluated the factors including nutritional status that are associated with GS at discharge in elderly patients with acute heart failure who underwent exercise training.
From January to December 2015, we enrolled 93 consecutive patients over 80 years of age who were admitted to our hospital with acute heart failure. A 10 m walking test to measure GS was performed at the beginning of training (first time point) and at discharge (second time point). Nutritional status was assessed using the controlling nutritional status (CONUT) score.
At the first time point, five out of 93 patients (5%) had a GS of ≥0.8 m/s, whereas 24 patients (26%) achieved this speed at the second time point. Univariate logistic regression analysis revealed that age, sex, body weight, ADL before admission, handgrip strength, GS at the first time point, and improvement in CONUT score were associated with a GS of ≥0.8 m/s at the second time point. In the multivariate analysis, improvement in the CONUT score was associated with a GS of ≥0.8 m/s at discharge after adjustment for confounding factors.
Change in nutritional status during hospitalization is associated with GS at discharge in elderly patients hospitalized with acute heart failure.
Gait speed, Heart failure, Elderly, CONUT score
ADL: Activities of Daily Living; GS: Gait Speed; NT-proBNP: N-terminal pro-B-type Natriuretic Peptide; CONUT: Controlling Nutritional Status Score; LV: Left Ventricular; SD: Standard Deviation; CRP: C-reactive Protein
Elderly patients have impaired activities of daily living (ADL), and the incidence of hospitalization for acute heart failure further reduces their level of physical function, leading to the development of frailty [1-3]. In patients hospitalized with acute heart failure, physical function at discharge predicts mortality [4], suggesting that improving physical function to an adequate level during hospitalization is needed to reduce mortality in these patients. Exercise training is helpful to improve physical function [5], but, unfortunately, not every patient can achieve a high enough level of physical function despite the exercise training. Thus, identification of the factors involved in the improvement of physical function is required.
In patients with heart failure, nutritional status deteriorates during hospitalization because of disease progression and insufficient intake, which may cause further impairment of ADL [6,7]. Malnutrition is associated with low physical function at discharge in patients with heart failure [8]. In this study, we repeatedly measured physical function using gait speed (GS) during hospitalization, and evaluated the factors including nutritional status that are associated with GS at discharge in elderly patients with acute heart failure who underwent exercise training. We hypothesized that nutritional status during hospitalization is associated with GS at discharge.
From January 2015 to December 2015, we enrolled 93 consecutive patients over 80 years of age who were admitted to our hospital with acute heart failure. Patients who could not walk by themselves were excluded. Heart failure was defined based on the modified Framingham criteria, as follows: Satisfaction of two major criteria (paroxysmal nocturnal dyspnea, orthopnea, rales, jugular venous distension, third heart sound, and radiological signs of pulmonary congestion and/or cardiomegaly) or one major criterion together with two minor criteria (effort dyspnea, peripheral edema, hepatomegaly, and pleural effusion). A diagnosis of heart failure was made by a cardiologist or an internist. Poor ADL was defined as persons who are unable to go out by themselves before admission.
All patients underwent simple exercise training consisting of walking training and functional strength training of the lower extremities which was supervised by a physical therapist. Patients started training once they were able to walk without symptoms such as dyspnea. Blood pressure, pulse rate, and oxyopia saturation were measured before and after training. We performed these training in accordance with the standard cardiac rehabilitation program in patients with heart failure published by Japanese Circulation Society in 2014 [9]. In this program, it is described that all patients with acute heart failure may participate in cardiac rehabilitation programs when the patients' condition are stabilized. Also, patients are recommended to begin exercise training with bending exercise of limbs, low-intensity resistance training on the bed, and standing position practice and tiptoeing on the bedside floor. After the safety is confirmed, exercise training is advanced to walking, cycle ergometer, light aerobics, low-intensity resistance training. The study protocol was approved by the appropriate institutional review board of the hospital and all of the participants provided written informed consent.
Physical ability was assessed using a 10 m walking test to measure GS at the beginning of training (first time point) and at discharge (second time point). In the 10 m walking test, participants were asked to walk along a corridor at a comfortable speed. GS was calculated using the distance in meters and time in seconds. The maximum handgrip strength of the dominant hand was measured in kilograms using a handheld dynamometer. The best result of three attempts was recorded. A blood test was also performed at both time points to evaluate N-terminal pro-B-type natriuretic peptide (NT-proBNP) and nutritional status. NT-proBNP levels were measured using the commercially available Elecsys proBNP sandwich immunoassay using an Elecsys 2010 (Roche Diagnostics, Mannheim, Germany). Nutritional status was assessed using the controlling nutritional status score (CONUT) score [10] at both time points. The CONUT score was calculated using the serum albumin level (g/dL), total cholesterol level (mg/dL), and lymphocyte count (count/mL). Echocardiography was performed in the left lateral decubitus position using a commercially available system during hospitalization. Left ventricular (LV) mass index and LV ejection fraction was calculated in accordance with the recommendations of the American Society of Echocardiography [11].
Continuous variables were expressed as the mean ± standard deviation (SD) or the median with the interquartile range. Dichotomous variables were expressed as the number and percentage. Patients were divided into two groups based on their GS at the second time point, with a cut-off value of 0.8 m/s: [12] high GS group (n = 24) and low GS group (n = 69). Differences in the continuous variables between the two groups were analyzed using the Student's t-test, the Mann-Whitney U-test and Wilcoxon Signed-rank test, as appropriate. Categorical data were compared using the χ2 analysis and Fisher's exact test as appropriate. In a subsequent analysis, the NT-proBNP and C-reactive protein (CRP) data was log-transformed because they did not exhibit a normal distribution. Univariate and multivariate logistic regression analyses were performed to evaluate the predictors of a GS of ≥ 0.8 m/s at the second time point. The multivariate logistic regression included the variables that were associated with a GS of ≥ 0.8 m/s at the second time point. Statistical analyses were performed using SPSS V.24 statistical software (IBM, Armonk, NY).
Mean GS increased from 0.50 m/s to 0.63 m/s between the two time points (p < 0.001). The mean interval between the two time points was 13 days. At the first time point, five out of 93 patients (5%) had a gait speed of ≥0.8 m/sec, whereas 24 patients (26%) had a gait speed of ≥ 0.8 m/s at second time point (Figure 1).
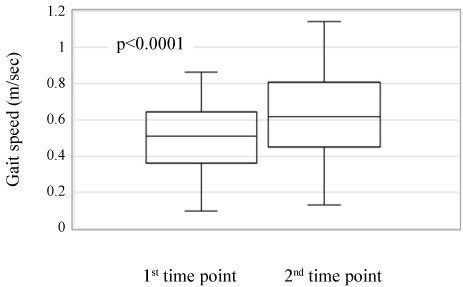 Figure 1: Comparison of gait speed between 1st and 2nd time point in all patients.
View Figure 1
Figure 1: Comparison of gait speed between 1st and 2nd time point in all patients.
View Figure 1
The patients' characteristics at baseline are shown in Table 1. There were differences noted between the groups as follows: The low GS group was older and had a higher proportion of women; and the low GS group also had a higher prevalence of patients with poor ADL and had a lower body weight and handgrip strength. There was no statistical difference in CONUT scores, cardiac parameters, such as NT-proBNP and LVEF, at baseline between the two groups.
Table 1: Patients characteristics at baseline. View Table 1
The changes in variables between the two time points are shown in Table 2. Hand grip strength was higher in high GS group than that in low GS group at both time points.GS increased, and NT-proBNP and CRP levels decreased in both groups. CONUT scores significantly improved in the high GS group, but not in the low GS group. Among the factors that contribute to the CONUT score, total lymphocyte count, serum albumin, and total cholesterol improved in the high GS group, whereas only albumin improved in the low GS group. The delta changes in clinical parameters between the two time points are shown in Table 3. The high GS group showed greater changes in both GS and CONUT scores. The percentage of patients with improved CONUT scores was higher in the high GS compared with the low GS group (79% vs. 52%, p = 0.020).
Table 2: Changes in clinical parameters between the two time point. View Table 2
Table 3: Delta changes in clinical parameters between the two time points. View Table 3
In the univariate logistic regression analysis, age, sex, body weight, ADL before admission, handgrip strength, GS at baseline, and improvement in CONUT score were associated with a GS speed of ≥ 0.8 m/s at the second time point. In the multivariate analysis, improvement in the CONUT score was associated with a GS speed of ≥ 0.8 m/s at the second time point after adjustment for confounding factors (Table 4). During hospitalization, one patient in the low GS group died. The mean length of hospitalization was significantly longer in the low GS compared with the high GS group: 29 vs. 20 days (p = 0.008). All patients in the high GS group were discharged and returned home, whereas 13% of patients in the low GS group were transferred to a skilled nursing home (p = 0.081) (Figure 2).
Table 4: Clinical factors associated with a gait speed of ≥ 0.8 m/sec at the 2nd time point. View Table 4
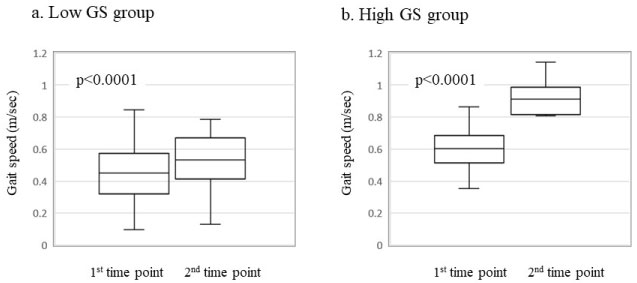 Figure 2: Comparison of gait speed between 1st and 2nd time point.
Figure 2: Comparison of gait speed between 1st and 2nd time point.
a) Low gait speed group; b) High gait speed group.
View Figure 2
In this study, we repeatedly evaluated physical function using GS during hospitalization in elderly patients who were admitted with heart failure and who underwent exercise training. Although only 5% of patients had a GS of ≥ 0.8 m/s at the beginning of training, the percentage increased to 26% at discharge. Patients who had a GS of ≥ 0.8 m/s at discharge showed improvements in their nutritional status, as assessed using the CONUT score. Conversely, there was no change in nutritional status in patients with a GS of < 0.8 m/s at discharge. Improvement in the CONUT score was associated with a GS of ≥ 0.8 m/s at discharge in these patients.
GS, which is a simple and useful assessment of physical function, is a predictor of cardiovascular events in the general elderly population [13] and in elderly patients with heart failure [14]. A few previous studies have demonstrated a relationship between nutritional status and physical function, [8,15] but none have evaluated the influence of changes in nutritional status on physical function at discharge.
In the present study, we have shown a significant association between the improvement in nutritional status during hospitalization and GS at discharge. There are several potential explanations for this association. In patients with heart failure, malnutrition is common and is associated with greater mortality [6]. Malnutrition causes a loss of skeletal muscle mass and strength, both of which are characteristics of sarcopenia [16] which becomes highly prevalent in old age, and contributes to a greater risk of physical disability [17]. Higher circulating levels of amino acids, as well as exercise, stimulate muscle protein synthesis [18], which may improve muscle strength and prevent the development of sarcopenia. We have found that hand grip strength remains relatively high in patients with high GS, in whom the CONUT score improved. Maintenance of skeletal muscle strength using a combined nutritional and exercise strategy may explain the sufficient GS achieved at discharge.
In contrast, nutritional status did not improve in the low GS group, which may have been responsible for the inadequate improvement in GS in these patients. Although the precise reason for the difference in the time-course of the CONUT score during hospitalization between the two groups has not been explained, we speculate that a lower appetite and malabsorption may underpin the sustained malnutrition during hospitalization in the low GS group [8,19].
Higher GS is associated with better outcomes [20,21], and improvement in GS during hospitalization seems to be an important target in the treatment of heart failure in elderly patients to improve their outcome. However, in this study, many patients could not achieve an adequate level of GS at discharge, despite their treatment for heart failure and exercise training. The effect of exercise training on the improvement in muscle size and function in elderly people is smaller than that in younger people [22]. Thus, additional treatment should be provided to improve physical function in elderly patients with heart failure. Our results show that the improvement in nutritional status is related to the high GS in elderly patients, indicating that we need to focus more attention on nutritional status to improve physical function in elderly patients. The CONUT score, which is based on three parameters: serum albumin, total cholesterol, and total lymphocyte count, enables us to evaluate patient protein reserve, calorie depletion, or immune function relatively simply [10,23]. Monitoring of nutritional status using the CONUT score, and nutritional interventions, such as the provision of high-protein oral nutritional supplements [24], guided by the CONUT score, might have a beneficial effect on the physical activity of elderly patients admitted with acute heart failure.
Several limitations should be considered when interpreting our results. There was a difference in patient's characteristics, such as age, sex, level of ADL before admission, hand grip strength, and GS at baseline between the two groups. Although there is a possibility that these factors contributed to the difference in GS improvement during hospitalization, the association between the improvement in the CONUT score and achieving a GS of ≥ 0.8 m/s at discharge was still significant after adjusting for these confounding factors. We acknowledge that this was a single-center study with a relatively small number of individuals with heart failure who were over 80 years of age, and thus, it is unclear if the findings of this study can be extrapolated to other populations.
Improvement in the nutritional status is associated with achieving an adequate GS at discharge among elderly patients who were hospitalized with heart failure. Our results have indicated the importance of monitoring nutritional status during hospitalization to maintain adequate physical status of patients. Further studies, such as an intervention study using an oral nutritional supplementation in combination with exercise training, and accompanied by monitoring of nutritional status using the CONUT score, are needed to validate our results.
We thank Rachel Baron, PhD, from Edanz Group (www.edanzediting.com/ac) for editing a draft of this manuscript.
The authors have no conflict of interest that is directly relevant to the content of this article. All authors have read and approved submission of the manuscript, and the manuscript has not been published and is not being considered for publication elsewhere in whole or part in any language except as an abstract.
SS and NK designed the study. TI, TY, MN, AM, YK and TW collected the data. SS and NK performed the statistical analysis and wrote the paper. KK, MT and YK revised the paper and contributed to discussion.
All authors read and approved the final manuscrip