Lactate dehydrogenase has had an exciting journey as a utility marker in different illnesses, but currently, its clinical utility has been relegated to confirm hemolysis, as a tumor marker, and as a diagnostic biomarker of preeclampsia. The findings of lactate dehydrogenase concentrations taking reference values to healthy persons are not consistent when these are related to hypertensive disorders in pregnancy, mainly to begin symptoms or little severity presentation. The goal in this work was to evaluate the maternal serum concentration of lactate dehydrogenase and its utility as a severity or diagnosis marker for hypertensive disorders in pregnancy.
In this retrospective study, we included 5,558 cases of HDP and 800 healthy pregnancies. HDP classification and LD values were collected from the medical records in the paper chart.
The prevalence of HDP in our hospital was approximately 6.4 ± 0.1%. We found a tendency toward increases in median LD concentrations with the increasing severity of HDP and found a positive correlation (p = 0.037) or error probability of 0.037% between LD concentrations and severity of HDP in Mexican pregnant women.
Serum LD concentration in HDP is a marker of severity, diagnosis and adverse maternal outcomes.
Lactate dehydrogenase, Hypertensive disorders in pregnancy, Diagnostic markers
Lactate dehydrogenase (LD) is a cytoplasmic enzyme that is widely expressed in tissues and cells. LD is an enzyme in the glycolytic pathway catalyzes the oxidation of L-lactate to pyruvate with the mediation of nicotinamide adenine dinucleotide (NAD+) as the hydrogen acceptor. This reaction is reversible and can be detected in the laboratory in serum samples by measuring LD activity in terms of the rate of dihydronicotinamide adenine dinucleotide dehydrogenase (NADH) production determined spectrophotometrically at 340 nm [1,2]. LD is a critical serologic marker for diagnosis, staging/prognosis, and recurrence, and monitoring of germ cell tumors [3], as well as for multiple myeloma, another malignant disease wherein high LD levels are associated with disease severity and poor prognosis [4,5]. Serum LD levels increase in proportion to the clinical severity of idiopathic pulmonary arterial hypertension and have a strong, independent association with the long-term mortality of these patients. Assessing the potential role of LD as a biomarker and mediator involved in the pathogenesis of idiopathic arterial hypertension might be worthwhile [6]. LD has had an exciting journey as a utility marker in different illnesses, but currently, its clinical utility has been relegated to confirm hemolysis, as a tumor marker, and as a diagnostic biomarker of preeclampsia (PE) [3,7]. However, the findings of LD concentrations taking reference values to healthy persons are not consistent when these are related to hypertensive disorders in pregnancy (HDP), mainly to begin symptoms or mild PE.
The HDP are among the leading causes of maternal and perinatal morbidity and mortality worldwide [8]. The public classification system was adopted by the National High Blood Pressure Education Program (NHBPEP) Working Group in 1990 and subsequently endorsed by 46 medical organizations. The updated version in 2000 has become a standard that the American College of Obstetrics and Gynecology (ACOG) follows. From the NHBPEP original reports, guidelines from international societies have emerged, each one with their evidence, although many with similar recommendations [9]. The HDP should be classified as pre-existing hypertension, gestational hypertension, preeclampsia, or others hypertensive effects based on different diagnostic and therapeutic considerations. Hypertension in pregnancy is defined by systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg [10].
Dramatic changes in the cardiovascular system occur throughout gestation beginning soon after conception, presumably with the objective of increasing blood flow and nutrient delivery to the fetal-placental unit. The Healthy pregnancy is associated with increased endothelium-mediated relaxation, blunted response to vasoconstrictors, and increased flow-mediated dilation [11]. Modification of the placental bed arteries to reach a high-flow, low-resistance status to support this increased blood flow is achieved by extravillous trophoblast-mediated remodeling of spiral arteries, with a replacement of the endothelium by trophoblasts [12]. The link between abnormalities in trophoblast invasion and generalized maternal endothelial dysfunction seen in HDP, particularly in preeclampsia, maybe via release of placental factors, such as syncytial knots, shedding of syncytiotrophoblast basement membrane fragments (STBM), leukocyte and platelet membrane particles, activated neutrophils, cytokines, growth factors, angiogenic factors, and hormones [13]. These factors will interact with the maternal vascular endothelium, which may already be damaged and can cause maternal endothelial cell damages. The STBM may also damage the endothelium and activate neutrophils, and this may lead to endothelial dysfunction as part of the widespread intravascular inflammation [14]. Evidence for endothelial dysfunction in preeclampsia includes reduced in-vitro endothelium-dependent dilatation of isolated vessels, increased vascular reactivity in response to vasoconstrictor stimuli, and elevated biomarker levels associated with endothelial activation and injury [12]. Detection of high-risk patients with increased LD levels, as a marker of endothelial damage by HDP, mandates close monitoring and correct management to decrease both maternal and fetal morbidities [15]. In the present study, we evaluated the maternal serum concentration of LD and its utility as severity or diagnosis marker for HDP.
In this retrospective study of 10 years, we included all women diagnosed with any HDP who were admitted to the Gynecology and Obstetrics Department of the Hospital General de Durango, Mexico, between January 2008 and December 2017.
Pregnant women with any HDP were identified by final diagnosis of the patient at discharge in the hospital and recruited by the archive and statistic department in agreement of the ICD-10 code. Patients with HDP diagnosed from localities outside the Durango state and women with HDP associated with trophoblastic disease were excluded. HDP diagnosis was confirmed by medical record review by the principal investigators. Gestational hypertension was defined by systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg on at least two occasions 6 hours apart, without proteinuria. Preeclampsia was defined as > 20 weeks gestation with incident hypertension (defined as a systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure 90 mmHg on at least two occasions 6 hours apart) and proteinuria (300 mg protein excreted over 24 h, or 30 mg/dL in a random urine sample or 1+ protein on urine dipstick). Eclampsia was defined by seizure occurrence in women with preeclampsia that cannot be attributed to other causes. The hemolysis, elevated liver enzymes, and low platelet (HELLP) syndrome in preeclamptic or eclamptic women was defined by platelet count less than 100,000 cells/mm3, liver enzymes more than twice the normal value, and the presence of microangiophatic haemolytic anemia, or observation of burr cell schistocytes and polychromasia on peripheral blood smear observation. Healthy pregnancies were defined as those normotense pregnant women without complications before, during and later pregnancy resolution.
Maternal demographic data including place of birth, age, gravity, gestational age at delivery, mean arterial pressure (MAP), HDP classification, and LD values were collected from the medical records in the paper chart. LD values were taken from the first laboratory examination during admission. The LD concentrations were determined through a dry chemistry method in Johnson & Johnson Vitros® 5.1 FS analyzer by (Ortho Clinical Diagnostics 1001 U.S 202 Raritan, NJ 08869), validated with daily internal quality control and monthly by external quality assurance programs.
The SPSS software (version 15.0; SPSS Inc., Chicago, IL, USA) was used to perform statistical analysis; the clinical characteristics of the HDP sub-types were expressed as mean ± standard deviations (SD) or median and interquartile range (IQR). The mean of the continuous values was compared using the Student's t-test after testing for normality using the Kolmogorov-Smirnov test. A p-value equal to less than 0.05 was considered statistically significant. Mann-Whitney U-test, or student's t-test depending on the normality distribution, was performed to compare the groups. To calculate bi-variate correlation between LD values and HDP severity expressed in the probability that LD concentrations are a severity marker of HDP, we calculated the Spearman range correlation, and data were represented in graphic distribution by error bars later. Finally, a baseline was obtained with IQR (Q1 - Q3) of LD values for each HDP classification, and reference values were established for each classification.
Ethical approval was obtained from the Institutional Review Boards of the Hospital where this retrospective study was conducted. In our hospital 107,937 patients were attended in the gynecological & obstetrical service during 10 years, and 86,202 deliveries occurred during the same period, including fetal deaths 20 weeks gestation. A total of 5,552 women presented with pregnancy complicated with any HDP category in agreement with the criteria of NHBPEP and Technical Guidelines for Diagnosis, Prevention and Management of Preeclampsia-Eclampsia of Health Ministry in Mexico. The case distribution in 2008 to 2017 with the different sub-classifications of HDP, including 800 healthy pregnancies, is shown in Table 1. All cases were confirmed after the medical records were reviewed. The prevalence of HDP in our hospital was about 6.4 ± 0.1%. The occurrence of HDP has increased each year in proportion with the pregnant women attended. However, the proportion related to HDP severity had been changed with respect to mild PE and severe PE because severe PE had been increasing, whereas mild PE had been decreasing over these 10 years possibly by changes in clinical criterial for classification of mild and severe preeclampsia; however, gestational hypertension and eclampsia remained stable (Figure 1). With respect to the frequency of HDP: Gestational hypertension 37.1% (n = 2,057), mild PE 19.6% (n = 1,089), severe PE 32.7% (n = 1,817), eclampsia 3.1% (n = 172), severe PEE with HELLP 6.4% (n = 361), and eclampsia + HELLP only presented, 1.01% (n = 56), of all cases, respectively. The mean of the chronologic age of women was 24.8 ± 7.3 years; the mean for gestational age was 36.7 ± 4.0 weeks. The mean number of pregnancies was 2.29 ± 1.6, and MAP was 108.8 ± 18.3 mmHg. With respect to the chronological age of pregnant women, those who had eclampsia had the lowest mean age (21.6 years ± 6.2 SD), compared with media the total of the women.
Table 1: Lactic dehydrogenase values for different hypertensive disorders of pregnancy including normo-evolutive pregnancy. View Table 1
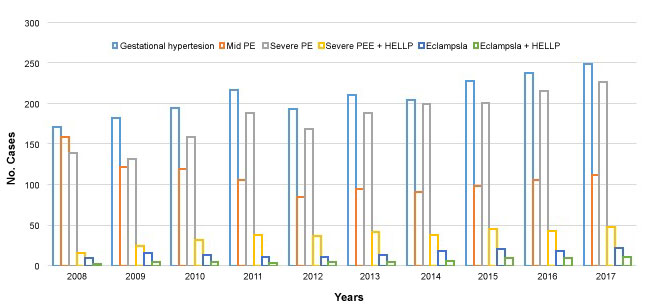 Figure 1: Serum Potassium Concentration of Albino (Wistar) Rats orally administered with a different dose of C. lanatus juices. Values are expressed as the mean ± standard error (n = 5). Values with the same later are statistically significant at P < 0.05.
View Figure 1
Figure 1: Serum Potassium Concentration of Albino (Wistar) Rats orally administered with a different dose of C. lanatus juices. Values are expressed as the mean ± standard error (n = 5). Values with the same later are statistically significant at P < 0.05.
View Figure 1
To calculate the LD reference concentrations for HDP; we include 14.5% (n = 800) LD values of healthy pregnancies which are shown in Table 1. So, LD reference values were stablished for normo-evolutive pregnancies and pregnancies complicated with HDP. Then, we found a tendency to increase the mean of LD concentrations in relation to HDP severity and PE complicated with HELLP syndrome. After establishing the data of non-parametric distribution, and Spearman range correlation analysis, we found a correlation (p = 0.037) or error probability of 0.037% between LD concentrations and HDP severity in Mexican pregnant women (Figure 2). Likewise, the median and interquartile ranges (IQR) were established for LD values to find reference ranges through Q1 and Q3 values and, propose a new reference range for Mexican normo-evolutive pregnant women and Mexican pregnant women complicate with HDP (Table 1). Finally we established a baseline of LD values related to HDP (Figure 3).
 Figure 2: Serum Sodium Concentration of Albino (Wistar) Rats orally administered with a different dose of C. lanatus juices. Values are expressed as the mean ± standard error (n = 5). Values with the same later are statistically significant at P < 0.05.
View Figure 2
Figure 2: Serum Sodium Concentration of Albino (Wistar) Rats orally administered with a different dose of C. lanatus juices. Values are expressed as the mean ± standard error (n = 5). Values with the same later are statistically significant at P < 0.05.
View Figure 2
 Figure 3: Serum Cardiac Enzymes Activity of Albino (Wistar) Rats orally administered with a different dose of C. lanatus juices. Values are expressed as mean ± standard error (n = 5) Values with the same later are statistically significant at P < 0.05.
View Figure 3
Figure 3: Serum Cardiac Enzymes Activity of Albino (Wistar) Rats orally administered with a different dose of C. lanatus juices. Values are expressed as mean ± standard error (n = 5) Values with the same later are statistically significant at P < 0.05.
View Figure 3
Based on the World Health Organization, HDP has been the second leading cause of maternal death globally to date [16], but it is the leading cause of maternal death in Latin America with up to 25% cases [17,18]. The most at risk age groups are young mothers aged between 10 and 24 years, and there are groups that present HDP with more severity [19]. Our population studied had a similar risk, with more prevalence of severe PE and eclampsia in young women (21.6 ± 6.2 years). In contrast, change in the decrease of frequency for mild PE and increase for severe PE was found in this study, and similar findings were reported first by Kuklina, et al. [20] in 2006, and recently by Cavazos-Rehg, et al. [21]. We also found that eclampsia was more frequent in first-time pregnant women unlike in any other HDP cases. The goal of monitoring symptoms and biochemical markers in patients with HDP is to appropriately time interventions and delivery while avoiding untoward maternal or neonatal complications. In contrast, LD has had an interesting journey, but today its clinical utility has been relegated to confirm hemolysis and serve as a tumor marker [22]. A study similar to ours was conducted by Qublan, et al. [15] and those authors found elevated LD levels at 111 IU/L in women with mild and severe PE, classifying three groups and LD values as follows: healthy pregnant (600 IU/L), mild PE (600-800 IU/L), and severe PE (800 IU/L), and they concluded that LD is indicative of cellular damage and dysfunction, and it can be used as a biochemical marker because it reflects the severity of the disease, occurrence of complications, and fetal outcome. In contrast, Jaiswar, et al. [22] conducted a study to evaluate LD as a biochemical marker for PE-eclampsia, and they analyzed 146 Indian women. They reported LD levels of 278.3 ± 119.2 IU/L in healthy pregnant women, and this value is similar to that found in our study (n = 379 and LD = 274 ± 100.7 IU/L). Furthermore, they concluded that LD levels had a significant association with various maternal and fetal outcomes in patients with PE and eclampsia. Other biomarkers in serum, such as soluble fms-like tyrosine kinase-1 (sFLt-1), vascular endothelial growth factor (VEGF), soluble intracellular adhesion molecule-1 (sICAM-1) and, soluble vascular intracellular adhesion molecule-1 svICAM-1, were varied and could not be pooled. To date, the literature on serum biomarker involvement in angiogenesis or inflammation after HDP has been inconsistent, with reports of lower [23] or higher [24] levels in women with PE. In fact, controversy exists because while Myatt, et al. [25] did not find that assessment of changes in angiogenic markers alone from the first or second trimester can improve predictive power, Widmer, et al. [26] also concluded in a multicenter study that angiogenic biomarker tests performed at ≤ 20 weeks gestation did not perform well enough in predicting PE for incorporation into current practice. However, these serum biomarkers, which are responsible for the initial endothelial insult during early pregnancy and are more expressed in placental tissue than in the endothelium, may not be detected at elevated levels after the index pregnancy. To clarify the confusing data regarding angiogenic factors and the need to obtain a better interpretation of traditional biomarkers, we propose LD values as indicative of cellular damage and endothelial dysfunction in HDP, and LD can be used as an effective biochemical marker because it reflects the severity of the disease, occurrence of complications, and fetal outcomes [15] in the Mexican population.
HDP diagnosis and classification are the main goals in pregnant women with high blood pressure, and the correct evaluation of clinical and laboratory parameters is important to achieve these goals. In this study, we showed that LD concentrations in HDP are predictive of adverse maternal outcomes and, we propose new LD reference values to classify HDP based on serum LD concentration and established a baseline of LD concentrations based on HDP severity. Currently, the basic biochemical tests for LD remain in effect to diagnose and classify HDP, and their use continues to provide valuable information for diagnosis and classification of pregnant women with HDP.
We thank the Hospital General de Durango of the Servicios de Salud de Durango, Mexico who supported and provided facilities for this work.
No potential conflict of interest was reported by the authors.