Hormonal and physical adaptations to pregnancy may result in musculoskeletal discomforts. The pattern and perception of these disturbances may form the basis for the health-seeking behaviours adopted by the pregnant women.
To determine the pattern of, perception on, and biosocial risk factors to musculoskeletal discomfort among pregnant women in South Eastern Nigeria.
This is a cross-sectional, interviewer-administered questionnaire-based study of 115 pregnant women attending antenatal-care outreaches in South Eastern Nigeria.
One hundred and fifteen antenatal volunteers were interviewed, majority were traders (50.4%) and within the age bracket of 26-30 years (45.2%). Most were of parity 1-4 (68.7%) and predominantly of social class 3 (60.0%). Up to 85 (73.9%) of the respondent had heard of musculoskeletal discomfort (MSD) during pregnancy while 55.7% had experienced it in the index pregnancy, and 32% in the last pregnancy. The types of MSD experienced in the index pregnancy includes pelvic pain 45 (70.3%), leg pain 16 (25%), low back pain 15 (23.4%), and coccydynia 1 (1.6%). The major causes of discomfort were attributed to malnutrition (55.6%), strenuous activity (54.7%), big baby (35.7%), pregnancy hormones (21.8%), and too many pregnancies (18.2%). Thirty-three (28.7%) respondents attributed MSD complications to miscarriage and premature deliveries. Experience of MSD, measured as discomfort respondent ratio (DRR) was high at extremes of maternal age, and increased with increasing gestational age, parity and social class. A significantly large number 30 (46.9%) had no form of treatment for their discomfort, while a few others applied a wrong treatment like antibiotics 1 (1.6%) and herbal concoctions 1 (1.6%).
This study showed a higher level of awareness and experience of musculoskeletal discomfort amongst the respondents. There was however insufficient knowledge as to the causes, risk factors, treatment and possible complications among them. Pelvic pain, leg pain and low back pain were the most commonly observed musculoskeletal discomfort amongst the respondents.
Health workers and pregnant women should have adequate knowledge, information and education on the various types of musculoskeletal discomforts as well as their causes, management and treatment as part of a comprehensive pregnancy health education package.
A lot of physical and hormonal changes that occur in pregnancy impact the musculoskeletal system leading to a variety of problems, such as back pain, pelvic/pubic pain, transient osteoporosis and tendonitis [1]. The weight gain, hormonal and other biochemical changes that occur during pregnancy increase the strain on the vertebrae and the appendages resulting in increased laxity (and hence mobility) of joints, increased lumbar lordosis, stretching/weakness and separation of the anterior abdominal muscles. Fluid retention can equally cause compression of vulnerable structures like the median nerve with attendant consequences [1]. The extent to which the skeletal system can be affected during pregnancy can be tremendous, with a variety of presentations that can to a considerable extent point to the particular type of musculoskeletal disorder.
Low back pain, a very common discomfort during pregnancy is defined as pain localized below the line of the twelfth rib and above the inferior gluteal folds. It could present as axial or parasagittal discomfort in the lower back region. It is essentially musculoskeletal and may be due to a combination of mechanical, circulatory, hormonal, and psychosocial factors [2]. Low back pain is a common symptom in pregnancy and occurs in about 50-70% of pregnant women [2-4]. It is most prevalent in the second half of pregnancy. Risk factors include pre-existing back pain, back pain in a previous pregnancy, advanced maternal age, and multiparity [4,5], while height, weight, race, fetal weight, and socioeconomic status do not appear to modify the risk [1]. A rare and undocumented cause of severe crampy low back pain in the early mid trimester of pregnancy has been experienced in relation to nephrolithiasis. The pain is episodic in nature, is usually aggravated by hard work or stress and is worse at night. The diagnosis is made from the discovery of renal stone in the kidney using ultrasonography. Treatment is conservative and involves microscopy, culture, and sensitivity studies of urine samples followed by treatment with relevant antibiotics, strong analgesics such as tramadol and the consumption of large volumes of water [6].
Pregnancy-related pelvic joint disorders including pubic symphysis separation, pelvic girdle pain, sacroiliac joint pain as well as pelvic girdle syndrome (pain in all the three pelvic joints) can arise during pregnancy following increased mobility and/or mechanical strain which can involve one or more of the pelvic joints.
There is usually pubic symphysis separation of at least 2 mm to 3 mm during pregnancy from the normal 4 mm to 5 mm gap in the non-pregnant state. Symphysis diastasis is diagnosed based on the persistence of symptoms and a separation of more than 10 to 13 mm on imaging [7]. The risk factors for pubic symphysis diastasis are fetal macrosomia, precipitous labour, rapid second stage of labour, intense uterine contractions, previous pelvic pathology, trauma to the pelvic ring, multiparity, and forceps delivery [8]. While pain resolves in the majority of patients within a month, the pelvis usually returns to normal by 4 to 12 weeks postpartum [9].
Pelvic girdle pain (PGP) is sometimes classified under the broad category of low back pain [1]. It is a specific form of low back pain, with onset during pregnancy or the immediate postpartum period [10]. It is described as a stabbing pain in the buttocks distal and lateral to L5-S1 which can radiate down to the knee, may be worse on weight bearing. It is related to nonoptimal stability of the pelvic girdle joints, hence pain in symphysis pubis, and/or uni- or bilateral pain in the sacroiliac joints are designated as PGP [10]. Risk factors include increased parity, previous low back pain, emotional stress, obesity, young maternal age, low educational level, early menarche, physically demanding work, and caesarean delivery [1].
Hip pain in pregnancy can result from osteonecrosis of the femoral head and transient osteoporosis of the hip. The former is rare with unclear aetiology, but may be secondary to weight gain, endogenous production of glucocorticoids by the adrenal gland [11], or a hypercoagulable state. It manifests as hip pain radiating to the groin or lateral thigh, particularly with weight-bearing. Transient osteoporosis of the hip also presents with pain on activity and limitation of motion of the hip. In contrast to osteonecrosis which may be progressive, transient idiopathic osteoporosis resolves by six to eight months postpartum with conservative therapy [12].
Knee pain including patellofemoral disorder are not uncommon in pregnancy. Postural changes, increase in weight, and increased laxity of ligaments can all contribute to pain in the knee. There is marked improvement in the symptoms of knee pain by 4 months after delivery. Patellofemoral disorder presents as pain behind or around the patella, especially when going up and down stairs or with prolonged sitting [1].
Leg cramps which is a common presentation in pregnancy usually manifests in the second half of pregnancy has uncertain aetiology but is believed to be from the build-up of lactic and pyruvic acids resulting in involuntary muscle contraction [13]. They are generally experienced in the calves at night.
Foot pain is significantly more common in pregnant women than in nonpregnant nulliparous women, self-limiting, resolving in less than four months [14]. Potential causes include weight gain, peripheral ligamentous laxity, and changes in posture and pedal pressure points [14]. Peripheral oedema is equally a notable cause of foot discomfort in pregnancy.
Hand and wrist pains are commonly caused by carpal tunnel syndrome and de Quervain's tenosynovitis. While the former is of neurological origin, the later occurs as a result of tenosynovitis of the abductor pollicis longus and extensor pollicis brevis tendons due to chronic overuse of the wrist and hand. De Quervain's tenosynovitis (or de Quervain tenosynovitis) results from stenosing tenosynovitis of the first dorsal compartment of the wrist which contains the two tendons [15]. It presents as pain at the dorsolateral aspect of the wrist, with referral of pain toward the thumb and/or the lateral forearm. It is more common in the postpartum period where lifting the infant can cause the initial irritation [1].
Chest wall pain: There are no causes of musculoskeletal chest pain specific to pregnancy other than fractures of the ribs that may occur with the rare disorder "pregnancy associated osteoporosis" [16]. Chest wall changes that occur during pregnancy include increases in the subcostal angle, the anterior-posterior and transverse diameters of the chest wall, and the chest wall circumference. These changes compensate for the elevation of the diaphragm during pregnancy and preserve total lung capacity, and are not usually associated with pain [1]. However, pregnant women, especially those who have a short torso or a very large uterus, near term may complain of discomfort (soreness and tenderness) in lower rib area, often on the right usually presumed to be due to pressure from the uterus in this area [1]. The painful rib syndrome characterized by discomfort in the lower chest or upper abdomen, tenderness over the costal margins, and reproduction of the pain by pressure on the ribs [17] is most common in women, usually unrelated to pregnancy.
Arthritis: Pregnancy related changes in circulating hormones may cause an imbalance in the immune system that may impact the activity of autoimmune diseases associated with arthritis. As a result of this, women who have rheumatoid arthritis may experience flaring in the postpartum period [1].
The range of structures involved in musculoskeletal discomfort during pregnancy, as elaborated in the foregoing, attests to the magnitude of the problem such discomfort can add to the overall burden of pregnancy. This study has been undertaken on pregnant women in South Eastern Nigeria to assess their experience of and perception on musculoskeletal discomforts and disorders of pregnancy. The biosocial characteristics of the pregnant women; their experience of musculoskeletal discomfort in the index and previous pregnancy; their perception as to the causes of musculoskeletal discomfort, the type of discomfort experienced as well as the treatment given for the relieve of the pains were all studied. The findings from this study are expected to arm health practitioners caring for pregnant women with the necessary information and instruments towards the recognition and effective management of the various types of musculoskeletal discomforts and disorders, should they occur during pregnancy.
This is a questionnaire-based, interviewer-administered cross-sectional study of 115 antenatal clinic attendees during two free antenatal care outreach programmes conducted at two locations - Nnewi and Nkpor in Anambra State of South Eastern Nigeria. Only pregnant women-attendees who gave their consent were drawn into the study. Oral consent was obtained from the participants after due explanation of the objective of the study. The questionnaires were administered by trained interviewers, consisting of clinical medical students and students of physiotherapy, under the supervision of consultant obstetrician and gynaecologist. The questionnaire-schedule elicited information from the respondents with respect to their biosocial characteristics - age, parity, gestational age, social class and occupation; their knowledge of and perception on musculoskeletal disorders during pregnancy with respect to causes, consequences and treatment; presence of musculoskeletal disorders in the current or immediate past pregnancy. The social class of the respondents was derived from Olusanya classification which makes use of educational level of the woman and the occupation of her husband [18]. Data from the completed questionnaire were keyed into the system and analysed using SPSS version 17.0. Statistical relationships between variables were calculated using the Chi square test and a p-value of < 0.05 at 95% confidence interval was considered significant for all statistical comparison. The incidence of experience of musculoskeletal discomfort was expressed as discomfort respondent ratio (DRR). Discomfort respondent ratio measures the overall musculoskeletal discomfort experienced, as a proportion of number of the respondents, with respect to the biosocial variables. Analysed data were displayed in tables and chats.
One hundred and fifteen antenatal attendees took part in the study. Table 1 shows the distribution by the biosocial characteristics of the respondents. Majority of the respondents were within the age range of 26-30 years, 52 (45.2%); of parity 1-4, 79 (68.7%); and of social class 3, 68 (59.1%). Majority of the respondents were of less than 28 weeks gestational age, 54 (47.0%) followed by those between 28 and 36 weeks, 41 (35.7%). Majority of the respondents were traders, 58 (50.4%); 12 (10.4%) were teachers, unemployed, 12 (10.4%), while civil servants were only 2 (1.7%).
Table 1: Distribution by biosocial characteristic of respondents (N = 115). View Table 1
The distribution by knowledge/perception of musculoskeletal discomfort in pregnancy for respondents as shown in Table 2, indicate that as high as 85 (73.9%) participants were aware of musculoskeletal discomfort in pregnancy. The major causes of discomfort were attributable to malnutrition 64 (55.6%) and strenuous activity 63 (54.7%), while big baby 41 (35.7%), pregnancy hormones 25 (21.8%) and too many pregnancies 21 (18.2%) are other attributable causes. Thirty-three (28.7%) participants were of the opinion that musculoskeletal discomforts can lead to miscarriages and premature deliveries.
Table 2: Distribution by knowledge/perception of musculoskeletal discomfort in pregnancy for respondents. View Table 2
Table 3 show the experience, and gestational age of occurrence of musculoskeletal discomforts by the respondents in the last and index pregnancies. Thirty (32%) had experienced one form or the other of musculoskeletal discomfort in the last pregnancy. As high as 64 (68.1%) of the respondent could not remember or know if they actually experienced it or not. Sixty-four (55.7%) of the respondents experienced musculoskeletal discomfort during the index pregnancy, 13 (11.3%) had no experience while 38 (33.0%) could not remember or know if they experienced musculoskeletal discomfort during the index pregnancy. The distribution of the respondents by the gestational ages at which they experienced musculoskeletal discomfort at both past and index pregnancy are, 10 (33.3%) and 30 (46.8%) respectively, at < 28 weeks gestational age; 11 (36.7%) and 15 (23.4%) respectively, between 28 and 36 weeks gestational age; and one a-piece (3.3%) and (1.6%) respectively, between 37 and 42 weeks of gestational age.
Table 3: Distribution by experience, and gestational age of occurrence, of musculoskeletal discomfort amongst respondents. View Table 3
Figure 1 shows the distribution by perceived cause of musculoskeletal discomfort during the preceding pregnancy. Majority of the respondents 63 (67.0%) did not respond to any knowledge of perceptions as to the cause of musculoskeletal discomfort; 15 (16.0%) suspected it was caused by strenuous activity; 7 (7.4%) was caused by trauma, and 4 (4.3%) was due to emotional stress.
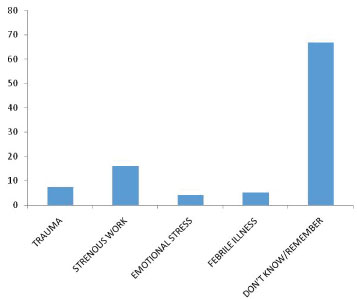 Figure 1: Distribution by perceived cause of musculoskeletal discomfort during the preceding pregnancy (last), N = 94.
View Figure 1
Figure 1: Distribution by perceived cause of musculoskeletal discomfort during the preceding pregnancy (last), N = 94.
View Figure 1
One hundred and fifteen antenatal attendees took part in the study. Table 1 shows the distribution by the biosocial characteristics of the respondents. Majority of the respondents were within the age range of 26-30 years, 52 (45.2%); of parity 1-4, 79 (68.7%); and of social class 3, 68 (59.1%). Majority of the respondents were of less than 28 weeks gestational age, 54 (47.0%) followed by those between 28 and 36 weeks, 41 (35.7%). Majority of the respondents were traders, 58 (50.4%); 12(10.4%) were teachers, unemployed, 12 (10.4%), while civil servants were only 2 (1.7%).
One hundred and fifteen antenatal attendees took part in the study. Table 1 shows the distribution by the biosocial characteristics of the respondents. Majority of the respondents were within the age range of 26-30 years, 52 (45.2%); of parity 1-4, 79 (68.7%); and of social class 3, 68 (59.1%). Majority of the respondents were of less than 28 weeks gestational age, 54 (47.0%) followed by those between 28 and 36 weeks, 41 (35.7%). Majority of the respondents were traders, 58 (50.4%); 12(10.4%) were teachers, unemployed, 12 (10.4%), while civil servants were only 2 (1.7%).
Figure 1 shows the distribution by perceived cause of musculoskeletal discomfort during the preceding pregnancy. Majority of the respondents 63 (67.0%) did not respond to any knowledge of perceptions as to the cause of musculoskeletal discomfort; 15 (16.0%) suspected it was caused by strenuous activity; 7 (7.4%) was caused by trauma, and 4 (4.3%) was due to emotional stress.
Figure 2 shows the distribution by type of musculoskeletal discomfort experienced during the index pregnancy. Sixty-four (55.7%) had experienced musculoskeletal discomfort of low back pain 15 (23.4%), leg pain 16 (25%), pelvic pain 45 (70.3%) and coccydynia 1 (1.6%).
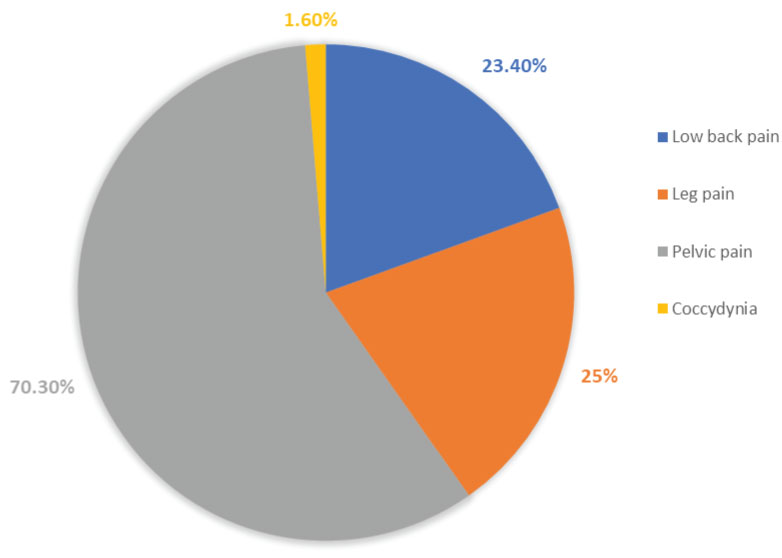 Figure 2: Distribution by types of musculoskeletal discomfort experienced during index pregnancy (N = 64).
View Figure 2
Figure 2: Distribution by types of musculoskeletal discomfort experienced during index pregnancy (N = 64).
View Figure 2
The distribution by treatments given to the sixty-four respondents that experienced musculoskeletal discomfort during the index pregnancy as shown in Figure 3 indicates that majority of the respondent 30 (46.8%) had no form of treatment for the discomfort. 12 (18.8%) had oral analgesics; 3 (4.7%), radiant heat treatment; 2 (3.1%), embrocation; while Other treatment given include- exercise 8 (12.5%); rest 7 (10.9%); antibiotics 1 (1.5%), and herbal concoctions 1 (1.5%).
 Figure 3: Distribution by treatments given to the respondents for musculoskeletal discomfort during index pregnancy (N = 64).
View Figure 3
Figure 3: Distribution by treatments given to the respondents for musculoskeletal discomfort during index pregnancy (N = 64).
View Figure 3
Table 4 shows the distribution by biosocial characteristics of the respondents for musculoskeletal discomfort, and discomfort respondent ratio (DRR). Pelvic pain was the most common discomfort experienced across all age groups, gestational ages, parity and social classes, constituting 39.1% in each biosocial variable, and this was significantly higher than the other types of musculoskeletal discomforts (p < 0.05). Coccydynia was the least common musculoskeletal discomfort (0.9%) across the biosocial variables. The incidence of experience of musculoskeletal discomfort was expressed as discomfort respondent ratio. Discomfort respondent ratio (DRR) measures the overall musculoskeletal discomfort experienced, as a proportion of number of the respondents, with respect to the biosocial variables. DRR is highest at extremes of age: 15-20-DRR-1; 41-50-DRR-2. The experience of musculoskeletal discomfort increase with increasing gestational age range being lower amongst respondents with gestational age less than 28 weeks, DRR = 0.7 compared to those of gestational ages 29-36 weeks and 37-42 weeks-DRR = 0.8 for each. Similarly, the experience of musculoskeletal discomfort increased with increasing parity - from 0.4 in the primigravida (para o) through 0.7 in the multipara (para 1-4), to 0.8 in the grand multipara (para 5 and above). The experience of musculoskeletal discomfort also adopted an increasing pattern with increasing social class of the respondent being 0.2 for the respondents of social class 1, 0.6 for social class 3; 0.8 for social class 4, and 1 for social class 5.
Table 4: Distribution by biosocial characteristics of the respondents for musculoskeletal discomfort and discomfort respondent ratio (N = 64). View Table 4
This study shows that as high as 85% of the pregnant women-respondents are aware of musculoskeletal discomfort in pregnancy. An experience of musculoskeletal discomfort in the index pregnancy, of 55.7% is also high. A lower experience of musculoskeletal discomfort of 32% observed amongst the respondents during their past pregnancy is perhaps on account of the fact that as high as 68.1% of those respondents did not remember whether or not they had experienced musculoskeletal discomfort during the past pregnancy, in contra distinction to only 33% not remembering, in the index pregnancy.
Respondents' perception as to the causes of musculoskeletal discomfort during pregnancy represents an admix of ignorance and reality. As many as 56.6 percent of the respondent believed that musculoskeletal discomfort result from malnutrition. But for obesity, the literature does not corroborate undernutrition as a risk factor to musculoskeletal discomfort in pregnancy. Undernutrition is the more common form of malnutrition amongst women, pregnant women inclusive, in this study area. Most of the women studied belong to the lower social class, with an increased likelihood of malnutrition. It is therefore tempting to speculate that hunger pangs which may be associated with unavailability of food to eat may have made the respondents to ascribe such a high prominence to malnutrition as a cause of musculoskeletal discomfort in pregnancy [1]. Strenuous activities also ranked high, as a perceived cause of musculoskeletal discomforts amongst the respondents. Kar, et al. had identified the place of strenuous exercise as a cause of high prevalence of musculoskeletal disorders especially amongst people of low socioeconomic class, which they suggested is related to stressful work posture, long working hours, use of ill-fitted tools and nature of jobs [19]. Other perceived causes of musculoskeletal discomfort by the respondents in this study includes big fetus, hormones, and 'too many pregnancies'. Although Bermas, et al. [1] have not identified fetal weight as a risk factor for musculoskeletal discomfort, Sabino and Grauer [2] had reported changes in pregnancy hormones together with mechanical, circulatory, and psychosocial factors as significant risk for musculoskeletal discomfort during pregnancy.
The most commonly observed types of musculoskeletal discomfort amongst respondents in this study are pelvic pain, leg pain and low back pain -70.3%, 25% and 23.4% respectively. Low back and pelvic pain may coalesce and become indistinguishable from patient's perception view point. The incidence of pelvic pain in this study, 70.3%, is similar to that reported by Calvalo, et al. 68% [20]. Pelvic joint disorders commonly occurring in pregnancy are associated with mechanical strains or increased mobility involving some of the pelvic joints. In this study, increasing gestational age resulted in increased prevalence of pelvic pain. Pelvic pain occurred in 37% of the respondents of less than 28 weeks gestation, and was as high as 66.7% in respondents of gestational age 37 weeks and above. The higher prevalence of pelvic pain with increasing gestational age is thought to be due to increase in fetal weight and pelvic pressure as pregnancy advances.
Higher parity resulted in increased prevalence of pelvic pain, from 23.8% of those with musculoskeletal discomfort who were nulliparous to 66.7% among the grand multiparous participants with musculoskeletal discomfort. This pattern of relationship between parity and pelvic pain agrees with the study by Bjelland and co-workers who found 11.0% of pelvic girdle syndrome among first-time mothers, 18% among primiparous participants and 21% among those with 2 previous deliveries [21].
Fetal macrosomia and multiparity are two of the risk factors perceived to cause musculoskeletal discomfort by the respondents in this study which have been reported in a previous study to constitute risk factors to pelvic girdle separation [8].
Leg pain manifesting as crampy feelings in the calves occur in as high as 25% of the respondents in this study. Leg cramps as mentioned earlier result from the build-up of lactic and pyruvic acid, usually at night and are of unknown aetiology.
The incidence of low back pain among respondent in this study, 23.4% is much lower than the 50-70% reported in previous studies [2-4]. Previously reported risk factors to low back pain in pregnancy observed in this study include increasing maternal age and parity. Socioeconomic factors which was earlier reported to have no influence as a risk factor [4,5] have been observed to do so in the present study. And this infact is in agreement with the observation of Knut, et al. who found that low socioeconomic status was associated with chronic musculoskeletal complaints among 46,901 adults studied, [22] albeit in the non pregnant state.
Discomfort respondent ratio (DRR) has been employed in this study to ascertain the prevalence of musculoskeletal discomfort in pregnancy with respect to the stems of the various biosocial characteristics which is an indirect reflection of the risk factors status of the biosocial variables. The incidence of musculoskeletal discomfort was relatively higher at extremes of maternal age (DRR-1 for age range 15-20, and DRR-2 for age range 41 and above). It increased with increasing gestational age being DRR-0.7 for gestational age less than 28 weeks and DRR-0.8 for gestational age above 28 weeks. Similarly, the incidence of musculoskeletal discomfort increased with increasing parity of the respondents from DRR-0.4 in the primigravida, 0.7 in the multipara and 0.8 in the grand multipara. The social class of the respondents showed similar manifestation with the incidence of musculoskeletal discomfort being highest in respondents of social class 5-DRR-1, and lowest in respondents of social class 1-DRR-0.2. Clearly therefore, extremes of maternal age, increasing gestational age, increasing parity and increasing social class all constitute risk factors to musculoskeletal discomfort during pregnancies. Maternal age and increasing parity as risk factor are in agreements with previous reports [4,5,8], although social class manifest differently from the report of the previous studies which shows social class as not constituting a risk factor for musculoskeletal discomfort during pregnancy [1].
Eric and Smith [23] in their study on musculoskeletal disorder had in general identified the female gender and age as the most common risk factors. Iranian investigators Ghaderi F, et al. [24] identified non-biosocial related risk factors to MSD, in pregnancy to include low back pain, job satisfaction, body mass index, job status, quality of life and history of previous low back pain while Rhiahi H, et al. [25] in their review of the role of imaging in the identification of risk factors to musculoskeletal disorders in pregnancy identified risk factors, particularly to pelvic girdle pain (PGP), to include genetic predisposition, multiparity, previous history of pelvic trauma, raised body mass index, elevated relaxin hormone levels, asymmetrical laxity of the sacroiliac joint, abnormal pelvic girdle biomechanics, excessive abduction in labor, strenuous work during pregnancy, and hypermobility of the joints.
Treatment given for musculoskeletal discomfort among the respondents in this study present an interesting picture. A considerably high number 30 (26.1%), of the respondents had no form of treatment for their discomfort. The reason for this may be that they and/or their healthcare providers either failed to appreciate or played down on the problem and its impact on their overall well-being. A few others had the wrong treatment like antibiotics and herbal concoctions. This buttresses the fact that acquisition and provision of comprehensive health education by the healthcare providers are important to improve on the knowledge of musculoskeletal discomfort and its treatment.
The awareness and experience of musculoskeletal discomfort by the respondents in this study were considerably high among the respondents; however perceptions as to the causes, risk factors, treatment and possible complications were either distorted or lacking. Pelvic pain was the commonest type of musculoskeletal discomfort followed by leg, and low back pain while coccydynia was found to be rare. Maternal age, gestational age, parity and social class all constituted identifiable risk factors to musculoskeletal discomfort in pregnancy. Musculoskeletal discomfort though a common presentation in pregnancy as shown in this and other studies, deserves a thorough evaluation with the view to appropriate treatment whenever present. The common practice of dismissing most musculoskeletal complaints as 'normal with pregnancy' deserves review.
Health workers and pregnant women alike are expected to have the requisite information and education on the various types of musculoskeletal discomforts, their causes, management and treatment, as a component of comprehensive pregnancy health education package. This would be expected to ensure that pregnant women encumbered with musculoskeletal discomfort receive the appropriate treatment to ameliorate the burden of this often nagging discomfort during pregnancy.
Our Sincere gratitude is extended to South-east PAC-Net for sponsoring this study.