Difficulty swallowing is called dysphagia. There is a wide range of potential causes of dysphagia. Because there are many reasons why dysphagia can occur, treatment depends on the underlying cause. Thorough examination is important, and implementation of a treatment strategy should be based on evaluation by a multidisciplinary team. In this article, we will describe the mechanism of swallowing, the pathophysiology of swallowing dysfunction and different causes of dysphagia, along with signs and symptoms associated with dysphagia, diagnosis, and potential treatments.
Dysphagia, Deglutition, Deglutition disorders, FEES, Videofluoroscopy
Dysphagia is derived from the Greek phagein, means "to eat" [1]. Dysphagia is any disruption in the swallowing process during bolus transport from the oral cavity to the stomach. The swallowing process is divided into four stages: Pre-oral, oral, pharyngeal and esophageal [2].
Pre-oral phase is when the food is transferred from plate to mouth. The oral phase is completely voluntary and involves the entry of food into the oral cavity and preparation for swallowing. The pharyngeal phase is initiated as the tongue propels the bolus posteriorly and the base of tongue contacts the posterior pharyngeal wall, starting a reflexive action. The soft palate elevates to prevent nasal reflux. The pharyngeal constrictor musculature contracts to push the bolus through the pharynx. The epiglottis inverts to cover the larynx and the vocal folds adduct to prevent aspiration. The esophageal phase is completely involuntary and consists of peristaltic waves [2].
Dysphagia is classified into the following major types:
1. Oropharyngeal dysphagia
2. Esophageal dysphagia
3. Complex neuromuscular disorders
4. Functional dysphagia
Swallowing is a complex process and many disturbances in oropharyngeal and esophageal physiology including neurologic deficits, obstruction, fibrosis, structural damage or congenital and developmental conditions can result in dysphagia. Breathing difficulties can sometimes affect the ability to swallow [3]. Some causes of dysphagia are explained here.
Various reasons for this type of dysphagia can be [4]:
• Bad teeth
• Problems with the jaw
• Xerostomia - dry mouth
• Tumors - cavum oris cancer, pharyngeal or laryngeal cancer
• Masses outside the pharynx, such as osteophytosis on the vertebrae that press on pharynx
• Complication of head or neck surgery
• Radiation leading to fibrosis, structural, mechanical, and neurologic deficits
• Stroke or some neurological disease like Parkinson's disease, multiple sclerosis or ALS
• Scleroderma - a rheumatic disease leading to a thickening, fibrosis and scarring of tissue
• Immune system diseases such as polymyositis
• Cricopharyngeal dysfunction- can result in material remaining in posterior pharynx with risk of aspiration of material into the airway after the swallow
• Age-related changes in swallow function
Diseases that can cause esophageal dysphagia can be grouped into different categories. Diseases that narrow the esophageal lumen through inflammation, fibrosis, or tumors, diseases that compromise the esophageal lumen, and diseases that disrupt esophageal peristalsis and/or lower esophageal sphincter function by their effects on esophageal smooth muscle [5]:
• Gastroesophageal reflux disease
• Esophagitis-can be caused by different problems, such as infections
• Eosinophilic esophagitis
• Esophageal spasm
• Achalasia-muscles in the esophagus lose their ability to relax and open
• Diverticula
• Tumors in the esophagus
• Masses outside the esophagus, such as tumors and osteophytosis on the vertebrae
• Radiotherapy treatment that causes stricture, fibrosis and stenosis
• Scleroderma-a rare condition that causes stiffening of the esophagus muscle
• Immune system diseases such as polymyositis
• Age-related changes
Damage to the neuromuscular system can interfere with the nerves responsible for starting and controlling swallowing. Some neurological causes of dysphagia include [6]:
• Stroke
• Neurological conditions that cause damage to the brain and nervous system, including Parkinson's disease, multiple sclerosis, motor neuron disease
• Myasthenia gravis-that causes the muscles to become weak
• Dementia
• Brain tumor
Functional dysphagia, defined in some patients as having no organic cause for dysphagia that can be found. There are several different causes to functional dysphagia [7]:
• Post traumatic syndrome stress disorder
• Stress attack
• Anxiety
• Different psychosocial disorders
Signs and symptoms associated with dysphagia may include:
• Salvia, food, liquid, or pills are sticking in the throat
• Coughing or choking food or liquid
• Sensing of a "lump" in the throat
• Having the sensation of food getting stuck behind sternum
• Wet voice
• Bringing food back up (regurgitation)
• Having food or stomach acid back up into the throat
• Unexpected weight loss
• Pain
• Developing aspirations pneumonia
When the dysphagia is frequent, and the cause is not clear, a comprehensive evaluation of dysphagia should include several medical disciplines including ENT doctors, gastroenterologist, occupational therapist, speech pathologist and dietitian. An examination begins with a clinical examination that includes a detailed history of subjective complaints and medical status. The ENT specialist will examine the mouth and throat and with flexible laryngoscope through the nose examine the throat in greater detail [8].
Several instrumental assessments of swallowing exist to provide objective information about swallowing function and safety. The most widely used procedure is a videofluoroscopic assessment of swallowing (Figure 1) and fiber-optic endoscopic evaluation of swallowing (FEES) (Figure 2). Videofluoroscopy describes X-rays records and shows how food and liquids move down, and helps to evaluate the entire swallowing process, the anatomy changes and dynamics of the swallow, identify the etiology of residue, penetration and aspiration, and assess the benefit of treatment strategies during the study. FEES consist of passing a thin, flexible endoscope into the pharynx and observing the act of swallowing. It provides excellent visualization of anatomical changes and identifies the etiology of residue, penetration and aspiration. Videofluoroscopy and FEES is thought to be the "gold standard" for assessment of in oropharyngeal dysphagia [8].
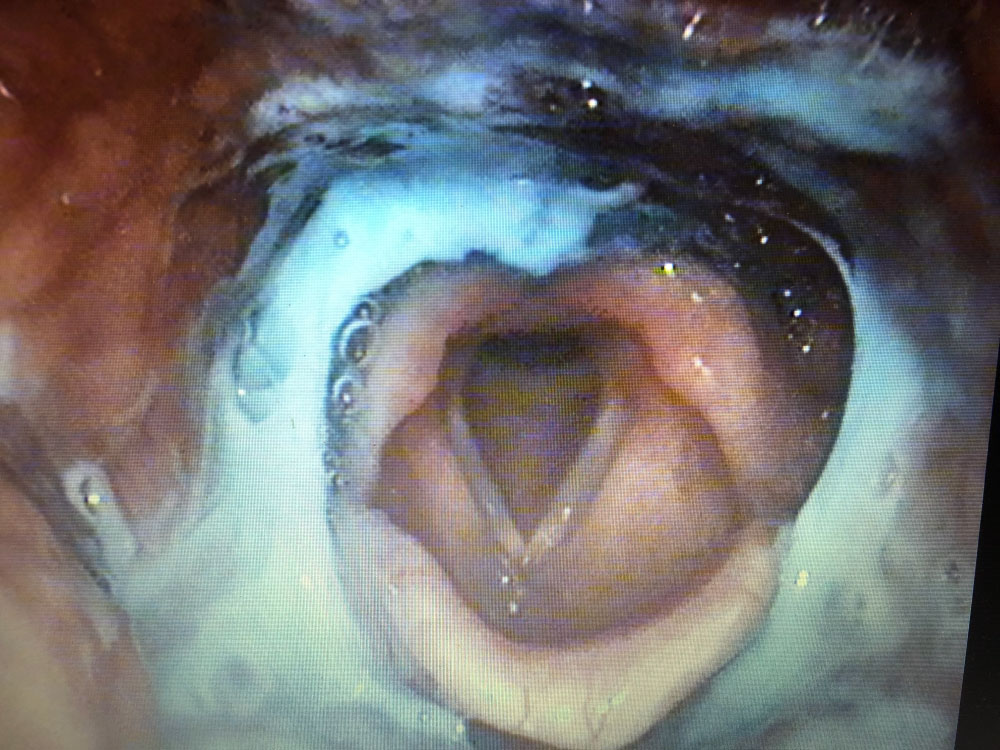 Figure 1: Videofluoroscopic assessment of swallowing. View Figure 1
Figure 1: Videofluoroscopic assessment of swallowing. View Figure 1
 Figure 2: Fiber-optic endoscopic evaluation of swallowing (FEES). View Figure 2
Figure 2: Fiber-optic endoscopic evaluation of swallowing (FEES). View Figure 2
Esophagoscopy is used to look at the esophagus and ventricle. Manometry evaluates pressure created by the throat and esophagus muscles. The pH monitoring is used to see how often acid from the stomach gets into the esophagus and how long it stays there. In some patients medical imaging modalities, for example ultrasound, computed tomography scanners, magnetic resonance imaging or proton emission tomography are necessary [9].
Treatment usually depends on the cause and type of dysphagia. Many cases of dysphagia can be improved with careful management, but a cure is not always possible [10,11]. Successful management requires multidisciplinary collaboration, accurate diagnostic workup and effective therapeutic strategies. Treatments for dysphagia include occupational therapist or speech and language therapy to learn new swallowing techniques, using texture modified foods and thickened fluids, changing the consistency of food and liquids to make them safer to swallow and in sometimes other forms of feeding – such as tube feeding through the nose or stomach [10,12]. Treatment to rehabilitate swallowing function and compensation techniques are common pathways for managing some cases of dysphagia [10,11]. Surgery is used in patients who have some changes (such as a tumor or diverticula) blocking the pharynx or esophagus or patients who have a problem that affects the lower esophageal muscle. Dilation is used to expand any narrow areas of the esophagus [13,14]. If dysphagia is related to GERD or esophagitis, medicines may help prevent stomach acid from entering the esophagus. Infections in pharynx, larynx and esophagus are often treated with antibiotic medicines. Botox injection of cricopharyngeus muscle and esophagus is used to treat dysphagia in patients with underlying muscle spasm and hypertonicity [15,16].
The most common complications of dysphagia are pulmonary complications, dehydration and malnutrition. Other possible complications, such as social isolation, mental and emotional health issues or intellectual and body development deficit in children with dysphagia, have not been studied thoroughly. The main pulmonary complications are aspiration pneumonia, toxic aspiration syndromes and pulmonary fibrosis [17].
Dysphagia is the medical term for the symptom of difficulty in swallowing. It is a common symptom in a wide group of patients. Patients with untreated dysphagia are at high risk of aspiration and malnutrition. Thorough examination is important, and successful management requires multidisciplinary collaboration, accurate diagnostic workup and effective therapeutic strategies. Treatment usually depends on the cause and type of dysphagia. Many cases of dysphagia can be improved with careful management, but a cure is not always possible.
No funding to declare.
Author declares that there is no conflict of interest regarding the publication of this article.
No ethical approval was obtained.
Informed consent not required.