Salivary gland tumours constitute 3% of all head and neck neoplasms. Pleomorphic adenomas arising in the maxilla are extremely rare, with only few cases reported to date. Radiographically and clinically, these lesions have the appearance of osteolytic processes or odontogenic cysts and the diagnosis represents a challenge. The surgical treatment of intraosseous glandular neoplasms is debated because of the few cases reported in literature. The Authors describe a rare case of intraosseous pleomorphic adenoma occurring in the maxilla along with a complete review of literature.
Maxilla, Pleomorphic adenoma
Tumours of the salivary glands account for 3% of all neoplasms. Pleomorphic adenoma is the most common salivary gland tumour and represents 60% to 70% of parotid tumours as well as 40% to 60% of the submandibular gland and minor salivary glands tumours [1,2]. Of the minor salivary glands, the palate is the most common site [3]. Ectopic salivary gland tissue has been found at various sites, including the skin of the neck, the hypophysis, the mastoid bone, the middle ear, the maxilla and mandible [3]. Pleomorphic adenomas arising in the maxilla are extremely rare with only few cases reported to date [3-5]. The intraosseous development of glandular tumours is rare and strict criteria evaluation is required to assess the central origin.
Radiographically and clinically, these lesions have the appearance of osteolytic processes or odontogenic cysts and the diagnosis represents a challenge [3,4]. We present an extremely rare case of intraosseous pleomorphic adenoma occurring in the maxilla.
A 56-year-old male patient was referred to the ENT and maxillo-facial surgery out-patient clinic after a routine dental scan for dental prosthetic rehabilitation; CT scan showed a well circumscribed mass with a well-defined border in the right maxilla (Figure 1). Clinical extra oral examination was unremarkable, no cervical lymphadenopathy was found. The patient was asymptomatic, the mucosa overlying the right maxilla was normal in colour and texture. The lesion was treated under local anaesthesia by enucleation and the defect was smoothened with a surgical burr to remove any residual tissue. The tumour mass was easily removed and was found to be delimited by bony walls without any communication to the maxillary antrum. The mass appeared (without a well definited capsule) as non-capsulated and of jelly-like consistency greyish-pink in colour.
 Figure 1: CT scan: A well circumscribed mass with a well-defined border in the right maxilla. View Figure 1
Figure 1: CT scan: A well circumscribed mass with a well-defined border in the right maxilla. View Figure 1
Histological examination showed a benign neoplasm of salivary gland origin; the features were suggestive of pleomorphic adenoma (PA) (Figure 2 and Figure 3). The specimen analyzed appeared translucent. The tumor looked to be well circumscribed and contained multiple strands, clusters, and islands of plasmacytoid myoepithelial cells with eosinophilic cytoplasm and hyperchromatic round to irregular nuclei. Many parts of the specimen revealed prominent ductal differentiation in neoplastic cells.
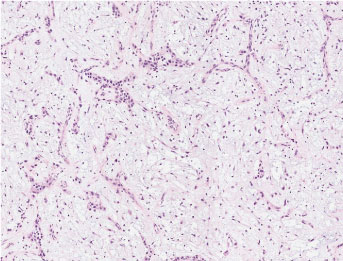 Figure 2: This tumor has zone of plasmacytoid cells in abundant mucinous material. The nuclear features of all cell type are uniformly bland, nucleoli are small or absent, and mitosis are few. (Scan-Scope Aperio System, original magnification ×10). View Figure 2
Figure 2: This tumor has zone of plasmacytoid cells in abundant mucinous material. The nuclear features of all cell type are uniformly bland, nucleoli are small or absent, and mitosis are few. (Scan-Scope Aperio System, original magnification ×10). View Figure 2
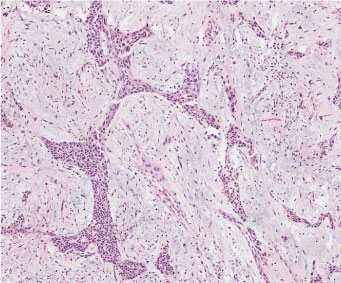 Figure 3: This tumor has zone of plasmacytoid cells in abundant mucinous material. The nuclear features of all cell type are uniformly bland, nucleoli are small or absent, and mitosis are few. (Scan-Scope Aperio System, original magnification × 20). View Figure 3
Figure 3: This tumor has zone of plasmacytoid cells in abundant mucinous material. The nuclear features of all cell type are uniformly bland, nucleoli are small or absent, and mitosis are few. (Scan-Scope Aperio System, original magnification × 20). View Figure 3
In other areas large cells with clear cytoplasm and small round to ovoid basophilic nuclei were found. This tumor has plasmacytoid cells in abundant mucinous material. The mesenchymal-like component accumulates between and around the epithelial elements and often isolates individual epithelial islands and trabecular structures as well as individual epithelial cells. The myxoid or myxochondroid areas contain some heparan sulfate but have large amounts of chondroitin sulfate.
Ductal and the other cells and myxomatous cells were intensely positive for cytokeratin (Figure 4) and E-cadherin (Figure 5). Vimentin and p63 immunoreactivity were present in almost all of the tumor cells and less variable in the clusters of duct-like epithelial cells (Figure 6). The immunoreactivity of S-100 is variable but may be found in all cell types (Figure 7). The index of cell proliferation (ki-67) is low, 1-2%.
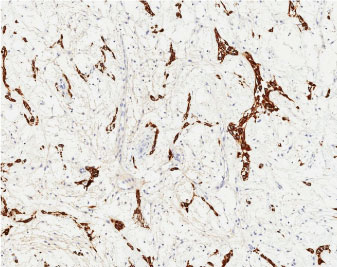 Figure 4: Cytokeratin immunoreactivity is stronger and less variable in the clusters of duct-like epithelial cells. (Scan-Scope Aperio System, original magnification × 10). View Figure 4
Figure 4: Cytokeratin immunoreactivity is stronger and less variable in the clusters of duct-like epithelial cells. (Scan-Scope Aperio System, original magnification × 10). View Figure 4
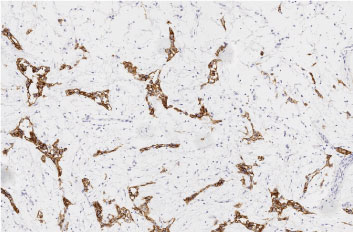 Figure 5: Immunohistochemical findings using E-cadherin antibodies. Most tumor cells showed strong positivity and less variable in the clusters of duct-like epithelial cells. (Scan-Scope Aperio System, original magnification × 10). View Figure 5
Figure 5: Immunohistochemical findings using E-cadherin antibodies. Most tumor cells showed strong positivity and less variable in the clusters of duct-like epithelial cells. (Scan-Scope Aperio System, original magnification × 10). View Figure 5
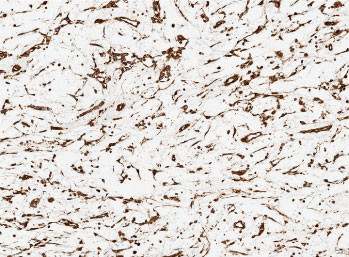 Figure 6: Vimentin immunoreactivity is stronger and less variable in the clusters of duct-like epithelial cells. (Scan-Scope Aperio System, original magnification × 10). View Figure 6
Figure 6: Vimentin immunoreactivity is stronger and less variable in the clusters of duct-like epithelial cells. (Scan-Scope Aperio System, original magnification × 10). View Figure 6
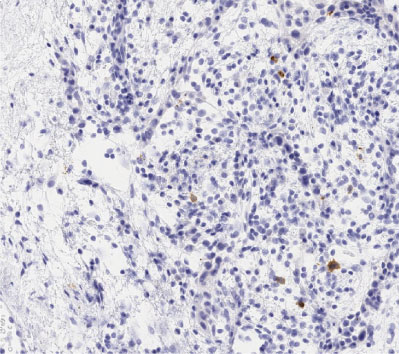 Figure 7: Immunohistochemical image showing that S-100 protein is variable but may be found in all cell types. (Scan-Scope Aperio System, original magnification × 20). View Figure 7
Figure 7: Immunohistochemical image showing that S-100 protein is variable but may be found in all cell types. (Scan-Scope Aperio System, original magnification × 20). View Figure 7
Cytokeratin, E-cadherin, Ki-67, p63, S-100 and Vimentin immunohistochemistry (IHC) were performed on 2.5 μm tissue sections and evaluated according to the manufacturer's recommendations. Specimens were fixed in 4% formaldehyde and embedded in paraffin. Sections were deparaffinized and rehydrated, and IHC was performed using a semiautomatic staining equipment (Autostainer Link 48, DakoCytomation, Glostrup, Denmark) and streptavidin-biotin horseradish peroxidase technique (LSAB-HRP). Specific staining was obtained by mouse anti-Cytocheratin, anti-E-cadherin, anti-Ki-67, anti-p63, anti-S-100, anti-Vimentin (Dako, Stockholm, Sweden, diluted 1:50) antibodies. The sections were examined under light microscope.
For the evaluation of cytokeratin, E-cadherin, p63, S-100 and Vimentin expressions, sum of the immunohistochemical staining was used, based on a proportion score (0-5) and an intensity score (0-3); the sum provides an expression score (0-8). These scores were reviewed and a consensus was reached that a score ≤ 3 was defined as negative and a score ≥ 4 as positive. Immunoreactivity of Ki-67 was evaluated by the counting of cells.
A scan of Major salivary glands was done to exclude the possibility of a primary tumour after the definitive histological examination.
The most common histological type of salivary gland tumour of the jaws of intraosseous central origin is the mucoepidermoid carcinoma [4,5] followed by adenoid cystic carcinoma. Pleomorphic adenomas are rare and the development into the maxilla is extremely rare found in literature with 5 cases. The first case reported, to our knowledge, was reported by Kovalik in 1966 [6], then Brookstone and Huvos [4] reported 1 cases in the maxilla; an additional 3 cases have been described by Aver-De Araujo, et al. [5] and Ferretti, et al. [7]. In 2017, Seema reported a case of pleomorphic adenoma of the maxilla that he assumed to be intraosseous but he admitted that the case did not fulfil the criteria to be classified as intraosseous because he found loss of integrity in some regions of the cortical bone [8]. Seema explains this as a result of the lesion causing a resorption of the cortical bone [8].
Several theories tried to explain the intraosseous origin of salivary gland tumours.
The first theory assumed that these neoplasms derive from neoplastic transformation of glands that migrate the marrow space through small cortical defects [9]. In this case there isn't a true intraosseous origin of these tumours. The central intraosseous origin is easier to recognize in the case of salivary gland tumours arising in the mandible versus arising in the maxilla because such tumours could derive from the submucosal secreting glands present in the maxillary antrum and then invade it through a small defect in the cortical bone. The doubt, in this first theory, that arises is why these tumours have such a big intraosseous component and no extra/osseous or a small component, although they originate from extra osseous secreting mucous glands.
A second hypothesis proposes the explanation of metaplastic or prosoplastic alterations into salivary tissue and then a neoplastic transformation of odontogenic epithelial lesions of periodontal ligament or dental lamina as the origin of intraosseous salivary gland tumours of the jaw. Mucous cells have been found in dentigerous cysts, dental cysts, periodontal, odontogenic keratocyst [10,11]. As reported by Brookstone et Huvos [4], in 30% of the cases of intraosseous salivary gland tumours of the jaws, there are odontogenic cysts or previous dental extractions. It is suggested that an odontogenic lesion the sialo odontogenic cyst often shows histologic similarity to mucoepidermoid carcinoma [12].
The third theory explains the presence within jaw bones of these unique tumours assuming that ectopic salivary tissue is entrapped during early development or from intraosseous sequestration of primordial salivary down growths of oral mucosa and later transformed into salivary gland tumours [12]. The presence of salivary embryonic rests, choristomas and hamartomas within the marrow space of the jaw has been proven by Bouquot, et al. they found 17 types of salivary tissue on 5034 intraosseous tissue samples within the alveolar marrow [12].
Strict criteria has been established to confirm the central origin of these lesions [4]:
• Positive histologic diagnosis of a salivary gland neoplasm;
• Evidence of osteolysis with integrity of the cortical bones;
• Absence of any primary lesion within the salivary glands or within other tissue resembling the histological architecture of glandular tumours.
Our case meets all the required criteria to confirm the central origin since the PA was found embedded of bone completely without communication with maxillary sinus and there wasn't a history of previous surgery to the salivary gland or presence of any lesion within the major salivary gland.
Radiological and clinical findings were typical of a benign lesion so the patient underwent complete enucleation of the lesion and smoothening by surgical burr of the bony wall of the surgical cavity, which in any case appeared normal. The surgical treatment of intraosseous glandular neoplasms is debated because of the few cases reported in literature. Brookstone and Huvous affirm that malignant lesions need more aggressive surgical treatment [4]. In terms of benign lesions, some Authors describe partial maxillectomy as the treatment of choice [7,8], while others consider more conservative treatments [3,5]. The authors think that the behaviour of intraosseous PA could be different from PA in major salivary glands. In literature, there is no histological description of the interface between the bone and the tumour or any atypical growth in the surrounding bony tissue of the PA; and for this reason, a partial maxillectomy could be an overtreatment in case of a benign lesion. Under all circumstances these lesions need careful follow ups.