Laparoscopic roux-en-Y gastric bypass (LRYGB) surgery is often performed on patients with body mass index (BMI) > 35 kg/m2 in Europe and the United States [1,2]. Due to the risk of malnutrition, LRYGB is not always suitable for Chinese diabetic patients, particularly for those with type 2 diabetes mellitus (T2DM), a BMI < 35 kg/m2, and when nutritional levels are not great pre-surgery. Modified gastric bypass surgery is reserved for diabetic patients with BMI < 35 kg/m2 by Chinese clinicians in order to balance the risk of malnutrition [3,4]. This study is the first to report the effect of LRYGB on a patient who was disappointed with the efficacy of modified gastric bypass operated 17 months ago.
The patient, a 42-year-old man, was admitted to our hospital because of hyperglycemia and subsequently requested surgical treatment. He had undergone a modified LRYGB for T2DM 17 months prior at another hospital in Yunnan province of the People's Republic of China. Seventeen months before the present admission, he had a body weight of 73 kg and a BMI 27.82 kg/m2. Prior to modified LRYGB, he was given metformin 25 mg three times a day, but still had inadequate glycemic control. He accepted modified gastric bypass surgery with a 300 mL gastric pouch, alimentary limb 25 cm, and bilio-pancreatic limb 60 cm on July 2011. However, despite the fact that the patient presented with a weight loss of 6 kg as a result of the surgery and hypoglycemic agents were used in an attempt to control glucose, he was not able to adequately control blood glucose levels. Postoperatively, 20 U of insulin glargine was administered subcutaneously at bedtime and metformin 25 mg was taken orally three times daily. Uncontrolled blood glucose with fasting plasma glucose 8-10 mmol/L and postprandial glucose of 12-13 mmol/L troubled him for a long time before he sought help in our hospital.
On admission to our hospital, he had a body weight of 67 kg and a BMI of 25.53 kg/m2. Waist circumference and hip circumference were 90 cm and 94 cm, respectively. Considering his extremely low BMI, a thorough preoperative evaluation was performed. Endoscopy revealed an anastomotic ulcer in A1 phase. Laboratory tests showed hyperglycemia with fasting plasma glucose 11.2 mmol/L, postprandial 2-hour glucose 20.3 mmol/L, glycosylated hemoglobin A1c (HbA1c) 9.3%, and dyslipidemia with triglyceride 2.07 mmol/L, and low-density lipoprotein (LDL) cholesterol 4.15 mmol/L (Table 1). Work-up included imaging examinations, such as electrocardiogram, echocardiography, abdominal ultrasound, and X-ray film, and other examinations, including peripheral nerve electrophysiological examination and pulmonary function, which were all negative preoperatively. Islet functional reserve was good.
Table 1: We had followed up the patient for 18 months form the second surgery. The significance of this report is that a diabetic patient with low BMI who had ever undergone bariatric surgery can benefit from laparoscopic roux-en-Y gastric bypass. View Table 1
This study was conducted in compliance with the protocol approved by the Ethics Committee of the Guangzhou Liuhuaqiao Hospital and we obtained written informed consent from the patient and his family.
The patient underwent laparoscopic gastric bypass surgery on the fifth day after admission. Postoperative changes as a result of the modified gastric bypass could be seen in the abdominal cavity (Figure 1A). There was no bleeding exudate, and the remaining organs were normal. From the original 35 cm gastrointestinal anastomosis, the proximal jejunum was closed using a linear cutting staple by an end-to-side anastomosis (Figure 2B), and the gastric fundus and proximal jejunum were removed (Figure 1C). A small stomach pouch of about 30 mL was established using standard gastric bypass surgery (Figure 2A), with a 100 cm alimentary limb and a 100 cm bilio-pancreatic limb (Figure 1B, Figure 2C and Figure 2D). There were no complications during the hospital stay. The patient recovered very well and was discharged on the sixth day after surgery.
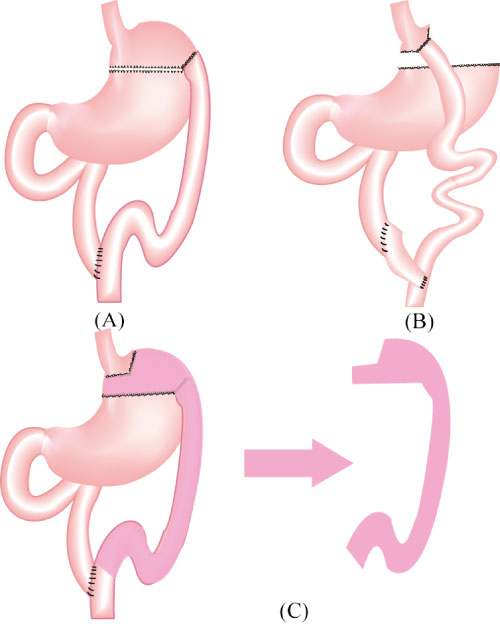 Figure 1: Two types of roux-en-Y gastric bypass surgery. A) Modified roux-en-Y gastric bypass surgery, which has a gastric pouch between 30-400 mL, and shorter alimentary and bilio-pancreatic limbs below 80 cm, is performed for diabetes patients with BMI < 35 kg/m2 by Chinese clinicians in order to balance the risk of malnutrition; B) Roux-en-Y gastric bypass surgery with a gastric pouch 15-30 mL and alimentary and bilio-pancreatic limbs 75-150 cm according to the weight of patient is suitable for obese type 2 diabetes mellitus treatment. The gastric pouch is anastomosed to the distal portion of the jejunum (Roux limb), and the distal stomach and proximal portions of the jejunum (biliopancreatic limb) are anastomosed farther down the jejunum to create a common channel. At present, there is no unified standard for the length of alimentary and bilio-pancreatic limbs; C) Closed proximal jejunum using a linear cutting staple by an end-to-side anastomosis and the gastric fundus and proximal jejunum are removed. View Figure 1
Figure 1: Two types of roux-en-Y gastric bypass surgery. A) Modified roux-en-Y gastric bypass surgery, which has a gastric pouch between 30-400 mL, and shorter alimentary and bilio-pancreatic limbs below 80 cm, is performed for diabetes patients with BMI < 35 kg/m2 by Chinese clinicians in order to balance the risk of malnutrition; B) Roux-en-Y gastric bypass surgery with a gastric pouch 15-30 mL and alimentary and bilio-pancreatic limbs 75-150 cm according to the weight of patient is suitable for obese type 2 diabetes mellitus treatment. The gastric pouch is anastomosed to the distal portion of the jejunum (Roux limb), and the distal stomach and proximal portions of the jejunum (biliopancreatic limb) are anastomosed farther down the jejunum to create a common channel. At present, there is no unified standard for the length of alimentary and bilio-pancreatic limbs; C) Closed proximal jejunum using a linear cutting staple by an end-to-side anastomosis and the gastric fundus and proximal jejunum are removed. View Figure 1
 Figure 2: Sequence of LRYGB after modified RYGB. A) Establishing a small gastric pouch; B) Cutting the alimentary-limb of modified RYGB; C) Connect the distal jejunum to the posterior wall of the stomach with a linear cutting staple by an end-to-side anastomosis; D) Connect the proximal jejunum to the distal jejunum from the anastomosis 80 ~ 120 cm with a linear cutting staple by an side-to-side anastomosis. View Figure 2
Figure 2: Sequence of LRYGB after modified RYGB. A) Establishing a small gastric pouch; B) Cutting the alimentary-limb of modified RYGB; C) Connect the distal jejunum to the posterior wall of the stomach with a linear cutting staple by an end-to-side anastomosis; D) Connect the proximal jejunum to the distal jejunum from the anastomosis 80 ~ 120 cm with a linear cutting staple by an side-to-side anastomosis. View Figure 2
We followed up with the patient four times after hospital discharge at 1, 3, 12, and 18 months. Glucose metabolism, lipid metabolism, and complications were monitored closely at every visit (Table 1).
The global epidemic of diabetes and obesity is one of the most important public health problems today. Complications, such as metabolic syndrome, T2DM, cardiovascular disease, hypertension, and dyslipidemia, amongst others, can cause patients tremendous harm and even death. The effect of RYGB surgery on patients with T2DM and a BMI > 35 kg/m2 is well known and the long-term efficiency has been verified by many clinicians. Most of these patients experience an improvement in glucose metabolism and weight loss after this type of bariatric surgery. However, the majority of T2DM or obese patients have a BMI below 35 kg/m2 in the People's Republic of China [5], which as a single nation accounts for more than 20% of the world's population. For most Chinese people, limited weight loss occurs after standard gastric bypass.
Many studies have demonstrated that patients with normal BMI can benefit from gastric bypass surgery. For instance, diabetes treatment guidelines in 2014 reported that a few small clinical trials have indicated that T2DM patients with BMI between 30-35 kg/m2 can also benefit from this kind of bariatric surgery. However, there is still insufficient evidence to generalize in favor of one bariatric surgical procedure for the non-morbidly obese population with T2DM.
In order to balance the risk of long-term complications, mainly reducing the risk of malnutrition, clinicians in the People's Republic of China have modified RYGB to be appropriate for T2DM with BMI < 30 kg/m2. A larger gastric pouch, about 30-400 mL in volume, is the main feature of modified RYGB. Moreover, it has shorter alimentary and bilio-pancreatic limbs. Herein, we report a case of LRYGB on a diabetic patient with a low BMI who had uncontrolled glucose after modified gastric bypass surgery 17 months ago. The patient experienced poor glucose control, with HbA1c level of 9.3% 17 months after modified gastric bypass. After standard bypass surgery, the patient's weight decreased significantly, from 67 kg to 51 kg during the first three follow-ups, and indicators of glucose metabolism showed a remarkable improvement, with HbA1c going from 9.3% to 5.4%. Therefore, we confirm the short-term therapeutic effectiveness of LRYGB for this patient. The patient did not return to our hospital at the fourth time follow-up (18 months after standard surgery) but we got results of inspection by telephone follow-up which were done in the people's hospital of Guangxi province, People's Republic of China. In order to verify the successfulness of the procedure, follow-up should be pursued for several years and particular attention should be paid to potential long-term complications.
This report raises several questions; for instance, whether modified gastric bypass surgery can reduce the risk of malnutrition by reducing the range of weight loss (Figure 3D). Generally, a larger volume gastric pouch means you can eat more food. Importantly, little concrete evidence is available to confirm that a small pouch is essential for adequate postoperative weight loss. Interestingly, Iannelli, et al. [6] demonstrated that functional pouch volume did not correlate with weight loss result, which is in accordance with the results reported by Madan, et al. [7] and Topart, et al. [8]. However, we worried that a larger volume gastric pouch may affect glucose control (Figure 3C). The second question is whether subsequent weight loss will bring about an improvement in glucose metabolism (Figure 3B). In earlier studies, most bariatric surgeons tended to believe that insulin resistance improvement was a consequence of weight loss. Currently, however, numerous studies have shown that glucose metabolism improvements after gastric bypass surgery has nothing to do with postoperative weight loss. So, what is the relationship between weight and glucose after gastric bypass surgery? How does weight loss affect maintaining stable glucose? All of these questions require many future studies to fully understand and answer. Thirdly, the short-term effects of modified gastric bypass surgery have been reported by Chinese clinicians [3,4], and similar results to standard gastric bypass surgery have been demonstrated. In the present study, the effects of glucose control after modified gastric bypass surgery are not obvious. Further observation is required to determine if longer follow-up periods are required to determine outcome. Fourth, what part of the surgery is the important for the hypoglycemic effect? In the present case, the alimentary and bilio-pancreatic limbs during modified gastric bypass surgery were shorter than during standard gastric bypass; whether this affected the outcome is unknown. Hickey, et al. [9] proposed that bypassing the foregut and reducing food intake produces profound long-term alterations in glucose metabolism and insulin action. This suggests that we should concentrate research on the effect of duodenum, jejunum, and ileum in regulating glucose metabolism. Thus, it is not known what contributes to the improvement in glucose metabolism: A long bypassing foregut or a smaller pouch volume? Fifth, the mechanism responsible for diabetes control after gastric bypass surgery is not clear (Figure 3A). Patriti, et al. [10] and Flatt, et al. [11] suggest that the improvement in glycemic control after bariatric surgery is due to the ablation of gastric inhibitory polypetide (GIP)-secreting intestinal K-cells located mainly in the proximal jejunum. Furthermore, GIP plays a key role in lipid metabolism and fat deposition. However, Le Roux, et al. [12] and Cummings, et al. [13] report that glycemic control after gastric bypass is associated with elevated peptide YY3-36 (PYY) and GLP-1 concentrations; undigested or partially digested food enters the terminal ileum earlier, stimulating the secretion of the gut hormones GLP-1 and PYY by L cells located in the terminal ileum, thereby promoting insulin secretion.
 Figure 3: The probable mechanism responsible for the control of diabetes after gastric bypass surgery. A) Hormone changes in the gut-islet axis after gastrointestinal tract reconstruction plays a key role in glucose metabolism; B) Improving insulin resistance caused by the accumulation of fat by reducing the patient's weight; C) Reducing the intake of energy and the load of glucose metabolism by reducing the intake and absorption of food; D) The volume of the pouch is closely related to an individual's weight. View Figure 3
Figure 3: The probable mechanism responsible for the control of diabetes after gastric bypass surgery. A) Hormone changes in the gut-islet axis after gastrointestinal tract reconstruction plays a key role in glucose metabolism; B) Improving insulin resistance caused by the accumulation of fat by reducing the patient's weight; C) Reducing the intake of energy and the load of glucose metabolism by reducing the intake and absorption of food; D) The volume of the pouch is closely related to an individual's weight. View Figure 3
Surgical treatment is a breakthrough in the treatment of T2DM. An important problem challenging clinicians is that the mechanism of glucose regulation is unclear and its theoretical basis is inadequate. This report was not designed to confirm that modified gastric bypass is not an effective procedure for T2DM patients with BMI below 35 kg/m2, but rather to provide some clues to answer some of the common questions associated with gastric bypass surgery. The long-term benefits and risks of modified RYGB in T2DM patients with BMI < 35 kg/m2 should be studied in well-designed controlled trials with optimal medical and lifestyle therapy as comparators. At the same time, we need to very carefully weigh the risks of this type of procedure against the benefits.
This work was supported in part by grants from the Science and Technology Program of Guangzhou (No.201508020002)to LPW.