Understanding of patient preferences is increasingly seen as an important factor to improve the effectiveness of care, especially in chronic conditions such as obstructive sleep apnea (OSA). Evidence of preferences of patients with OSA is still limited, though the disease is highly prevalent.
Aim of the study was to improve understanding of the relevance of treatment attributes among OSA patients. Based on a structured questionnaire, the relevance of attributes of OSA treatments as well as willingness-to-pay were evaluated. Principal component analysis and cluster analysis were used to define segments of patients with homogenous sets of importance ratings.
78 consecutive subjects with a mean age 60.97 ± 13.25 years and different OSA history participated in the study. The overall Cronbach's alpha was 0.748 with acceptable reliabilities for isolated items. Reducing risk of comorbidities was ranked most important (7.23 ± 1.40), followed by improving daytime sleepiness (6.91 ± 1.85) and ease of therapy application (6.90 ± 1.32), while co-payments of treatments (5.12 ± 2.47) and visibility of treatment (5.21 ± 2.26) were ranked least important on an eight-level Likert scale. Median willingness-to-pay for OSA treatment was € 10-20 per month. Three patient segments could be identified which consisted of homogenous sets of preferences: segment 1: Symptom improvement, segment 2: Physical integrity, segment 3: Treatment efficiency.
Importance of treatments attributes differs among patients with OSA. Gender and treatment history influence the importance ranking. Segments of patients with a common attitude to treatment attributes could be defined. These findings could help to increase disease understanding and preferences from a patient perspective and develop a more patient-centric approach to OSA care.
Sleep apnea, Patient preferences, Treatment attributes, Cluster analysis, Willingness-to-pay, Population segmentation
Among sleep-related breathing disorders, obstructive sleep apnea (OSA) is the most common chronic diseases, with prevalence in the developed world of up to 50%, which affects globally up to 425 million people [1-3]. Caused by a collapse of upper airway soft tissue, the gas exchange in the lungs can be disturbed, which can lead to nocturnal hypoxia and hypercapnia. Affected patients often arouse from sleep to gasp for air. These arousals lead to a fragmentation of sleep, which can cause daytime sleepiness and daytime dysfunction [4].
Especially in chronic diseases, patient engagement and participation are becoming more relevant in healthcare systems around the globe. Recent research raised awareness, that this could be an important factor to improve effectiveness of health interventions by ensuring acceptance by those affected directly [5]. A key element for patient centered design of health interventions is knowledge about patient preferences regarding treatment in general and potential alternatives, in cases of complications or side-effects. Specifically, in chronic conditions patient preferences can be an important factor in adherence and thus long-term effectiveness of a treatment. Though one of the most prevalent chronic diseases, evidence on preferences of patients with OSA is still limited. Objective of this study was to determine and evaluate attributes of OSA treatment, which are important to affected patients. In addition, the study aimed to investigate possibility of segmentation of patients, according to the ranking of identified attributes.
As part of a multi-trial project, we conducted an exploratory pilot-study in order to evaluate relevant attributes of OSA treatments from the patient perspective. Participants were enrolled from a tertiary sleep center cohort in Germany.
To determine the importance of different OSA treatment attributes, a structured questionnaire in German language was developed. The first part evaluated the respondents' OSA history as well as their current treatment status and their primary reason for care seeking was recorded with a multiple-choice question. Respondents could also state if they did not want to receive treatment or add other reasons, if relevant to them. To identify attributes of OSA care that might be of importance to patients, we performed a literature search on preference studies in the disease area. Nine different items that present attributes of OSA treatments were selected for the study: 1) 'improvement of daytime sleepiness', 2) 'improved treatment of comorbidities', 3) 'reducing risk of comorbidities', 4) 'occurrence of side effects', 5) 'treatment without surgery', 6) 'ease of therapy application', 7) 'co-payments of treatments', 8) 'visibility of treatment' and 9) 'ease of maintenance of therapeutic device'. A unipolar Likert scale with eight levels was used to rate importance from 1 (not important at all) to 8 (highly important). Individual item and overall survey reliability were estimated by computing Cronbach's alpha and internal consistency with intraclass correlation coefficient (ICC).
Willingness to-pay for OSA treatment was evaluated using a scaled question, with seven levels from € 0 to more than € 50 of monthly co-payment.
Participants were recruited from a tertiary sleep center in July/August 2020. Patients who presented at the sleep center for an overnight polysomnography with a newly confirmed diagnosis of OSA or an existing diagnosis and ongoing or former treatment with PAP therapy were eligible to participate. The study was conducted with approval of the local ethics committee (Ethics commission University Hospital Essen, Germany: 20-9315-BO) and all participants provided written informed consent. Questionnaires were admitted to participants in paper form and were answered by the participants after consultation with a specialist.
Survey data was managed using the Statistical Package for Social Sciences (IBM, New York / USA). Results are presented as mean with standard deviation, unless stated differently. For comparison of group differences, Student's t-test was used for nominal data and Mann-Whitney-U-Test was applied for ordinally scaled data. One- way analysis of variance (ANOVA) was conducted to evaluate differences in attribute ranking after splitting the data according to disease status and primary reason for care seeking. Spearman rank was used to evaluate correlation between attribute ranking and willingness-to-pay. For all tests, a two-tailed significance level of 5% was set. Clustering with k-means analysis was applied to identify patient segments, based on attribute ranking.
During a period of eight weeks, 78 consecutive subjects (57 males, mean age 60.97 ± 13.25 years) were enrolled into the study. All questionnaires contained sufficient data and all subjects were included in the final analysis. Reliability of the questionnaire was acceptable with a Cronbach's alpha of 0.748 and internal consistency was good with an average measure ICC of 0.748 and a 95% confidence interval from 0.649 to 0.828 (F (69, 552) = 3.995, p < 0.001).
Out of 78 patients, 21 had just received a diagnosis of OSA (26.9%), 43 had an existing diagnosis and stated to use regular therapy (55.1%) and 12 had an existing diagnosis but were untreated at time of the study (15.4%). The majority of respondents were seeking treatment to improve daytime sleepiness (36.58%), followed by reducing risk of comorbidities (24.39%), improved treatment of comorbidities (14.83%) and improving performance (14.83%). No significant differences by gender were found for OSA history (p = 0.205) and reason for treatment seeking (p = 0.058).
Sufficient data was available for all nine attributes, ranging from 71-78 answers (see image 1). Of all attributes, 'reducing risk of comorbidities' was ranked most important (7.23 ± 1.40), followed by 'improving daytime sleepiness' (6.91 ± 1.85) and 'ease of therapy application' (6.90 ± 1.32). Lowest ranked were 'co-payments of treatments' (5.12 ± 2.47) and 'visibility of treatment' (5.21 ± 2.26). The Students't-test was used to identify differences for respondents' gender, which revealed differences for importance of attributes 'improved treatment of comorbidities' and 'treatment without surgery'. Both attributes were significantly more important for female than male patients (t (74) = -2.018, p = 0.047 and t (72) = -2.050, P = 0.044). A one-way ANOVA was conducted to assess the effect of OSA history and reason for treatment seeking on the importance ranking of each of the nine attributes. Statistically significant differences by OSA history among the groups were not observed. For reason of treatment seeking, only 'improved treatment of comorbidities' varied significantly (F (4, 35) = 3.163, p = 0.025) and was obviously higher in respondents for whom this was the primary reason for treatment.
Firstly, a principal component analysis was conducted to reduce the data from the survey for subsequent cluster analysis (Figure 1). Three components were identified with an Eigen value > 1.0 that explained cumulative 63.5% of variance (rotated contribution rate 12.74 - 27.25%). Using k-means cluster analysis we were then able to identify structures in the survey responses and assign patients to different homogenous segments. Population segmentation is a relatively new approach, which us used to develop therapies and care models that meet individual health care needs by improving patient centricity of interventions, especially in chronic conditions [6]. Eight subjects had to be excluded from this part of the analysis due to incomplete data. Based on the cluster analysis we build three segments that were different from each other with regards to the ranked importance of treatment attributes (Figure 2). Derived from the attributes with the highest importance in the three segments, we named them accordingly to describe what drives treatment motivation of the patients included:
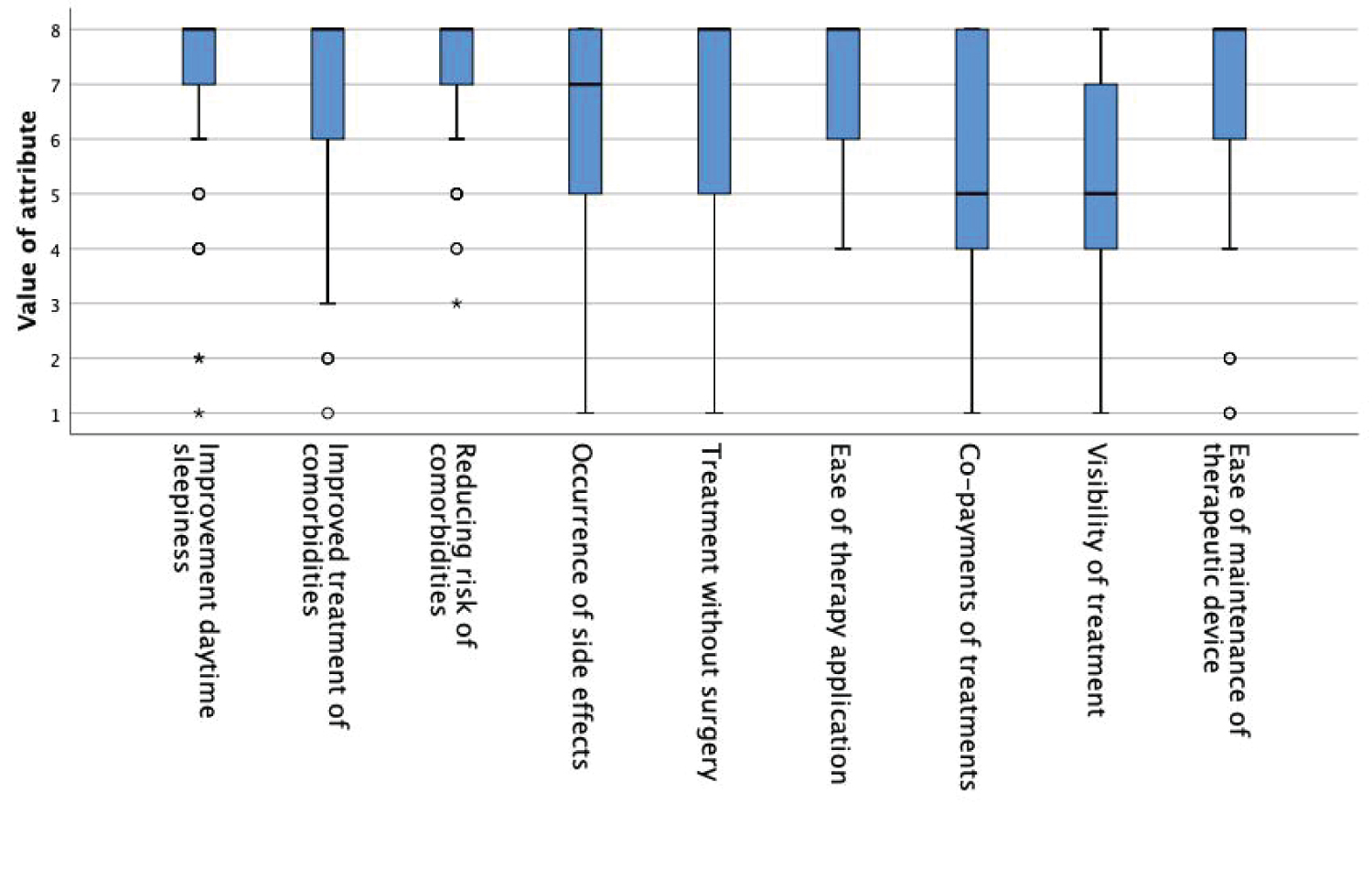 Figure 1: Boxplot graphic demonstrating differences in importance of treatment attributes.
View Figure 1
Figure 1: Boxplot graphic demonstrating differences in importance of treatment attributes.
View Figure 1
Segment 1: Symptom improvement
This cluster is dominated by the attribute 'improvement of daytime sleepiness' as the most important with an average value of 7.83, which is the highest ranking observed over all clusters and attributes. The other attributes are not defining this segment, as they are of lower importance, which in turn are among the lowest values seen in this study. Segment 1 is also the youngest subgroup with a mean age of 31.00 ± 15.13 years and has the smallest share of female patients with 8.3%.
Segment 2: Physical integrity
The second segment, which is also the largest of our cohort with 37 cases, consist of patients to whom potential negative consequences of OSA and its treatment matters most. In this cluster, 'reducing risk of comorbidities' (7.86), 'treatment without surgery' (7.62), 'occurrence of side effects' (7.35) and 'improved treatment of comorbidities' (7.16) receive the highest ranking and are of highest importance. All these attributes could be considered to contribute to physical health and wellbeing. As such, 'treatment without surgery' received the highest valuation in this group, compared to lower importance among the other two segments. Unlike in the other segments, 'improvement of daytime sleepiness' was not seen as relevant and received the third-lowest value in this segment (6.95). This segment also presents as the oldest of the three clusters with a mean age of 63.50 ± 12.05 and has the highest share of female patients of all segments (32.4%).
Segment 3: Treatment efficiency
The third segment, which consist of 21 cases, is not as homogenous as the first one with regards to importance of treatment attributes. Though therapy efficacy, expressed in 'improvement in daytime sleepiness' (7.00) and 'reducing risk of comorbidities' (6.86) is seen as most important, 'ease of therapy application' (6.71) and 'ease of maintenance of therapeutic device' (6.43) are considered highly relevant to this group of patients. We named this segment "Treatment efficiency" as this is what it drives the attributes relevance. This segments' mean age is with 57.00 ± 15.32 years 6.8 years younger than segment 2 and contains slightly fewer female patients (28.5%).
The median willingness-to-pay for OSA treatment among the respondents (n = 75) was € 10-20 per month, while the most respondents stated a willingness-to-pay of € 30-50 (Figure 2). No significant differences between gender, OSA history and reason for treatment seeking was found.
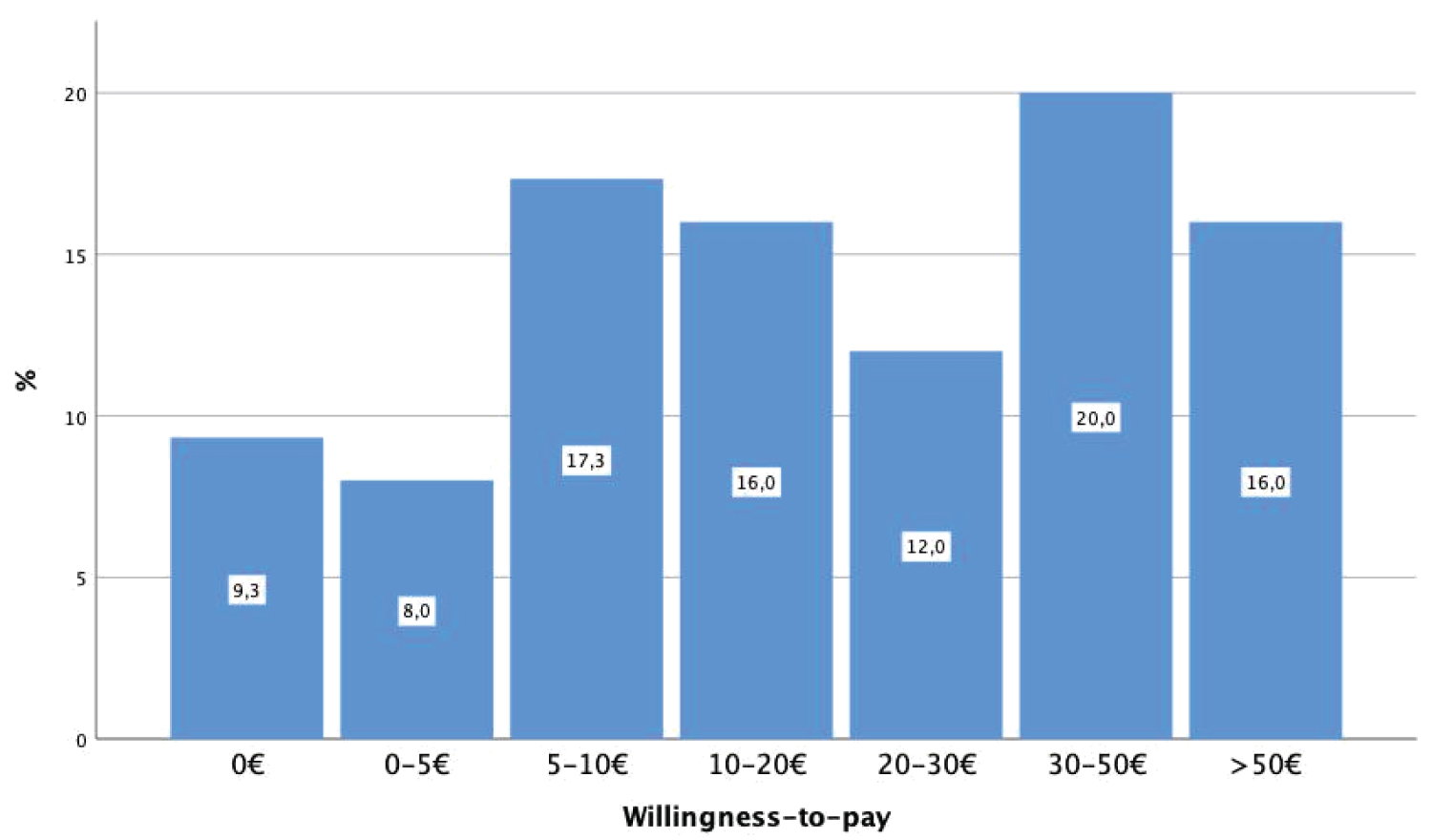 Figure 2: Monthly willingness-to-pay for OSA treatment.
View Figure 2
Figure 2: Monthly willingness-to-pay for OSA treatment.
View Figure 2
A positive correlation between willingness-to-pay and ranking of the attribute 'improving daytime sleepiness' was identified using a Spearman rank test (r2 = 0.237, p = 0.041). Applying the previously identified segments, we were able to confirm the results, which showed that highest willingness-to-pay was observed in patients belonging to segment 1 - Symptom improvement, with an average of € 30-50 per month (r2 = 0.240, p = 0.048). The lowest willingness-to-pay was seen in segment 2 with an average of € 5-10 per month.
The results provide initial insights to preferences of patients with OSA and could help in the design of future studies on this issue (Figure 3). Firstly, we can state that treatment attribute ranking varies among patients, which could influence the decision to accept treatment as well as adhere to one in the long-term. In the whole study cohort, 'reducing the risk of comorbidities' is seen as the most important factor of OSA treatment. This suggests that patients are well informed about possible negative consequences of untreated OSA. As patients mainly present at sleep centers when they are symptomatic, it is not surprising that 'improvement of daytime sleepiness' was ranked high as well. 'Ease of therapy application' was also seen as particularly important, which is in line with previous reports from other chronic diseases. Given that the most commonly used treatment Positive Airway Pressure (PAP) is often discontinued due to handling issues, further improvements in ease of use of therapies could also improve the chronic adherence.
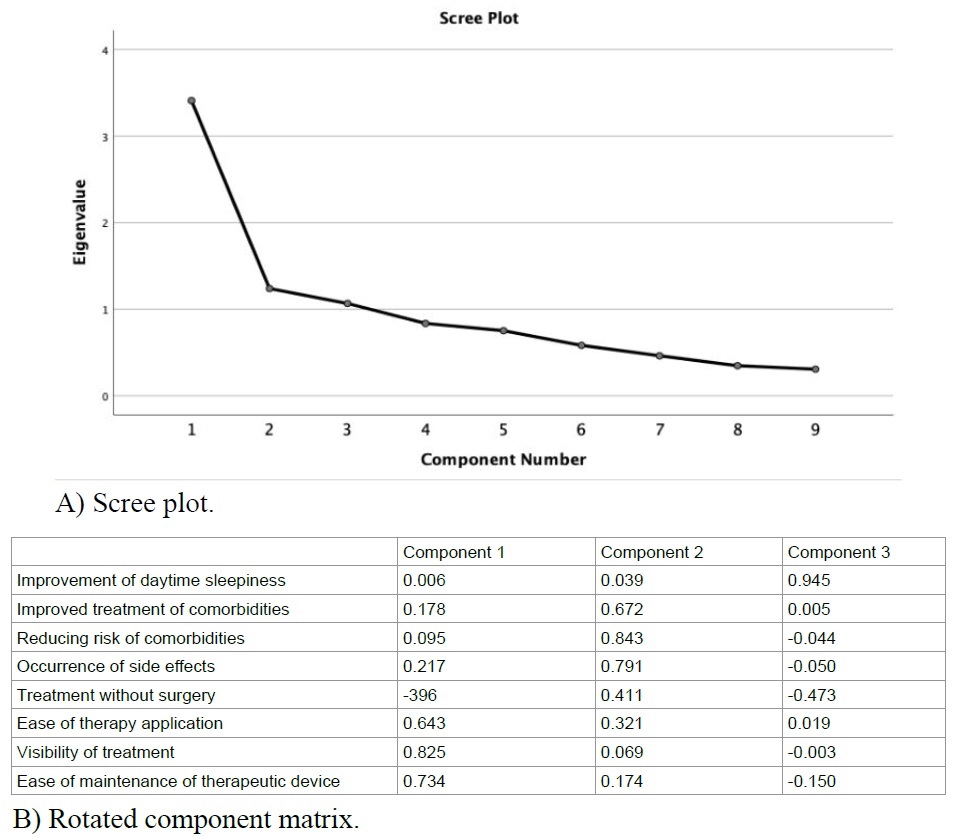 Figure 3: Principal component analysis.
View Figure 3
Figure 3: Principal component analysis.
View Figure 3
The fact that gender plays a certain role in the ranking of treatment attributes is important as it underlines that OSA presents differently in male versus female patients [7] (Table 1). In our study, 'improved treatment of comorbidities' and 'treatment without surgery' was of higher importance in female than male patients. This finding could be helpful to identify treatments that are well accepted by individual patients.
Table 1: Gender, OSA history and reason for treatment. View Table 1
The three patient segments (Figure 4) identified by cluster analysis demonstrate that homogenous groups can be identified, which in turn could be helpful to individualize therapies and develop targeted education materials for patients. From the three segments we found in our study cohort, it becomes clear that attitudes and motivational forces are different, which in turn can be important to achieve long-term adherence and therapy satisfaction. This could be important for clinical practice, such that treatments could be selected based on what the individual patients considers important for him. Patients for whom reducing the risk of comorbidities matters most might choose PAP therapy, while for others, ease-of-use is more important, and they might opt for Mandibular Advancement Devices or Hypoglossal Nerve Stimulation.
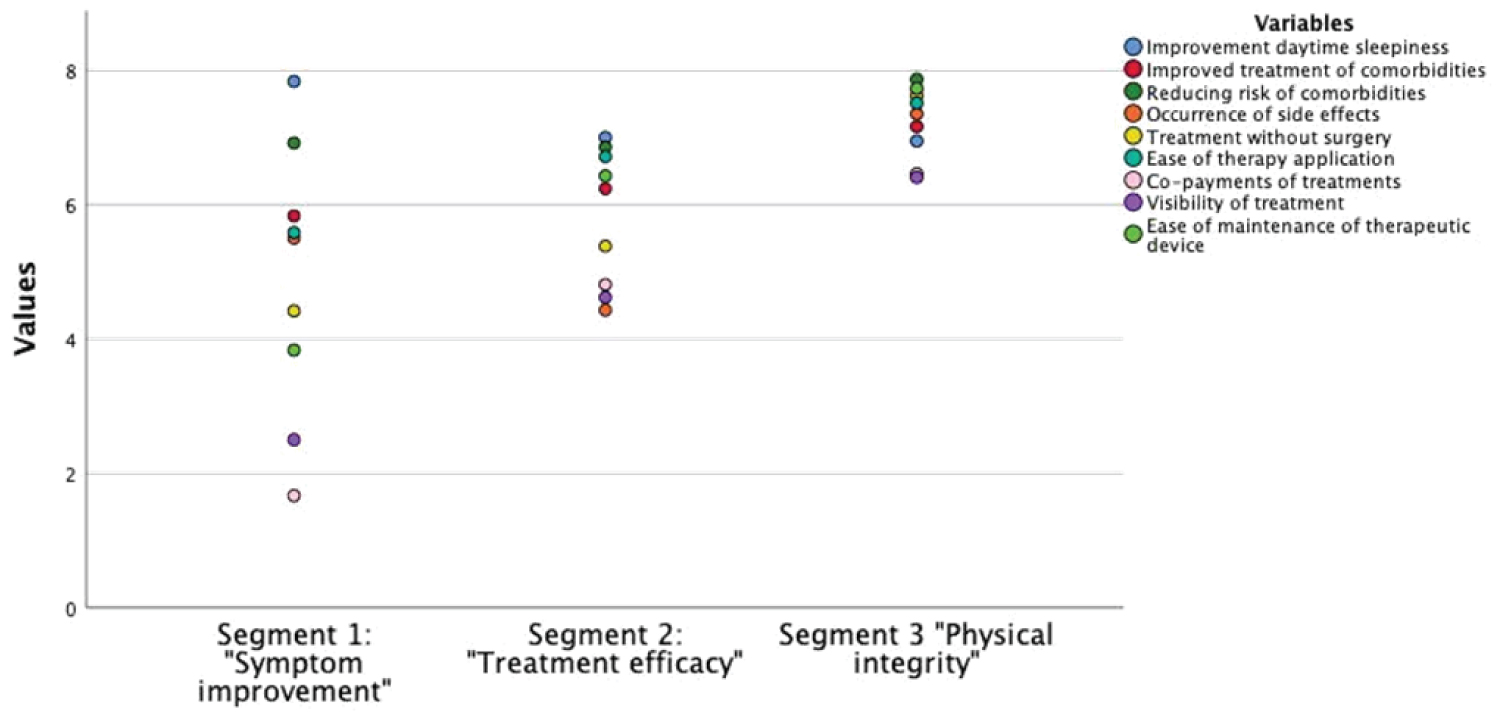 Figure 4: Final cluster centers, with segment 1 "Symptom improvement", segment 2 "Treatment efficiency" and segment 3 "Physical integrity". Dots represent the mean value of each attribute within the clusters.
View Figure 4
Figure 4: Final cluster centers, with segment 1 "Symptom improvement", segment 2 "Treatment efficiency" and segment 3 "Physical integrity". Dots represent the mean value of each attribute within the clusters.
View Figure 4
The willingness-to-pay in our cohort was rather low. This might be related to a general lower motivation to contribute to medical treatment among the German population due to a public health care system that covers many medical services and in which patients usually do not have to provide significant co-payments [8]. Willingness-to-pay was highest in patients of segment 1 - Symptom improvement, suggesting that the medical need is more urgent or apparent in this group and they are more motivated to pay for improvements in quality of life. Though we did not correct for household income or socio-economic status, this is in line with data from other respiratory indications [9,10].
These results could be helpful to further develop the emerging field of OSA phenotyping and personalized medicine for sleep-related breathing disorders. So far, the focus has been mainly on physiological factors, which impact the efficacy of treatments [11,12]. Adding patient preferences to the equation has the potential to substantially improve long-term adherence and thus improve the overall effectiveness of OSA interventions. This in consequence could generally improve the satisfaction and patient experience of medical care for OSA.
However, we have to admit that our analysis is subject to certain limitations. First, the list of attributes presented to the participants was not extensive and is prone to a selection bias. As participants were able to add additional attributes, they considered relevant, and only a few of them did so, we interpret our set of attributes being appropriate for such study. They are also in line with data reported previously [13-15].
While it was designed to be a pre-study for a subsequent project with the main objective to identify relevant attributes of OSA care, we did not collect information on OSA severity, medical history, socio-economic status and income. These additional data would allow a more precise analysis and relate attribute ranking to the medical status of each patient. Another limitation is the sampling from one sleep center with a certain catchment area in Germany. Conducting the same study in an area with different cultural background, socio-economic status and income might delivery different outcomes. Given the number of subjects and the distribution of answers, we are confident though that the results can used to draw certain conclusions.
The study adds aspects to the knowledge on treatment preferences of patients with OSA. We could demonstrate that attitudes and importance of attributes of treatments for OSA differ among individual patients and patient groups. The particular importance ranking allows to define relatively homogenous segments of patients, that share common preferences and attitudes. Willingness-to-pay for OSA treatment is also influenced by these factors. The findings from the study can help to develop a more patient-centric approach to care and can support adaption of patient education in order to improve therapy acceptance and thus long-term adherence.
This study received no funding.
All authors state that there is no conflict of interest for the subject matter and materials discussed in this manuscript.
The study was approved by the Ethics Commission of the University Duisburg-Essen (20-9315-BO) and all patients provided written informed consent.
MB and CS conceived the original idea and planned the study. MB and SD carried out the study and analyzed the data. MB wrote the manuscript with support from SD, CT and CS. CT and CS supervised the project.