Selective Amygdalohippocampectomy (SAH) is a widespread technique for Mesial Temporal Lobe Epilepsy (MTLE) treatment. Dr. Niemeyer was the first to describe SAH using transventricular approach technique in 1958. In 2018, we celebrate 60 years of the original description of Niemeyer's approach. This study reviews the approach in light of currently technology and shows the results achieved with patients submitted to SAH following Niemeyer's approach at Instituto Estadual do Cérebro Paulo Niemeyer (IECPN)*.
A retrospective case series of MTLE patients who underwent SAH using the transventricular approach between August 2013 and October 2015 at IECPN. Only cases with Hippocampal Sclerosis (HS) were included.
We identified 13 HS patients with 37.4 years mean age who underwent SAH, with favorable outcomes, 11 (84.6%) classified as Engel I while the other 2 (15.4%) as Engel II.
In our sample, the pioneer transventricular approach described by Niemeyer was followed to perform SAH while using current surgical resources with excellent outcomes.
Epilepsy, Temporal lobe, Amygdala, Hippocampus, Selective amygdalohippocampectomy
Epilepsy is a broadly studied disease, it affects about 1% of the world population, and is a common, difficult to treat pathology. Seizure is derived from the Greek and seize means "capture" or "take ownership". Epilepsy encompasses several types of disorders with different symptoms, and clinical manifestations [1-3]. The International League Against Epilepsy (ILAE) defines epilepsy as "two or more recurrent seizures over a period greater than 24 hours, without a clear set cause". The Term Temporal Lobe Epilepsy (TLE) was introduced in the ILAE classification in 1989 as the group of "Symptomatic epilepsies related to localization characterized by seizures with specific mode of precipitation". Over the years, there were changes in the classification and in 2017 the newest revision of terms and concepts of epilepsies was published [1-5].
The temporal lobe is the most epileptogenic region of the human brain and the most common site of the epileptic syndrome called Mesial Temporal Lobe Epilepsy (MTLE) [1,3,5-9]. MTLE has its peculiarities. Research of the Montreal Neurological Institute (MNI) suggested a psychic phenomenon with experimental hallucinations during intraoperative stimulation of this region. Gibbs and Lennox suggested the term "psychomotor epilepsy" to set a pattern of emotional mental and automations disorders, for crisis originated in the temporal lobe [1,10]. Gastaut proposed the term "Complex Partial Seizures" (CPS) for partial seizures associated with consciousness loss [1,10]. ILAE changed the term recently to "Focal Impaired Awareness Seizure" (FIAS) [5].
EEG and video-EEG (VEEG) tests are indispensable to research and determine the epileptogenic zone [4,11,12]. In about thirty percent of patients with MTLE, surface EEG detection of epileptogenic zone of discharge, with or without bilateral focus lateralization may be flawed. In these cases, we can use the Stereoelectroencephalography (S-EEG), which uses depth electrodes introduced by bilateral foramen ovale, to the mesial temporal lobe region to record the FIAS [5,13,14].
With the Magnetic Resonance Imaging (MRI), there has been dramatic improvement in the diagnosis of brain disorders, including cases of epilepsy. The primary objective of the image in patients with seizure is to exclude a possible structural lesion as a cause, either a brain tumor or an arteriovenous malformation. MRI is recommended for all patients who have FIAS. The Hippocampal Sclerosis (HS) is the most common pathological substrate found in MTLE patients MRI [4,12,15].
Antiepileptic Drugs (AEDs) such as phenytoin, carbamazepine, valproate, phenobarbital is widely used in FIAS treatment. As well as newer drugs such as topiramate, lamotrigine, oxcarbazepine and pregabalin [16]. Patients who remain refractory to drug therapy, should be evaluated for possible surgical epilepsy treatment [16-20].
Between the 1940s and 1950s, neurosurgeons, neurologists and neurophysiologists furthered studies to elucidate temporal lobe epilepsy, also using the Electroencephalogram (EEG) to locate the correct epileptic focus. After confirming the epileptic focus in the temporal lobe for psychomotor seizures, Paulo Niemeyer with the help of neurologists, used the EEG to study the epileptogenic activity of the hippocampus and its relation with cortical activity. Niemeyer believed that psychomotor epilepsy had its origin in the amygdala, the temporoinsular cortex, or the hippocampus, and these structures together formed a "functional unit responsible for the production of psychomotor attacks, leaving most cases of the temporal cortex in the background". Based on his studies, Niemeyer showed "astrocytic gliosis, particularly in the H2 and H3 areas of the hippocampus" (i.e., CA2 and CA3) in surgical specimens. This made it possible to affirm the secondary role of the temporal cortex. Based on these results, Niemeyer idealized a surgical technique where the amygdala and the hippocampus could be selectively resected, preserving the temporal cortex, which then became the Selective Amygdalohippocampectomy (SAH) [21-24].
In 1958, Paulo Niemeyer published the paper "The Transventricular Amygdalo-Hippocampectomy in Temporal Lobe Epilepsy". This technique was spread around the world and continues to be used today. Microsurgical anatomy of the temporal lobe in the human brain is complex, with great surgical importance. But it requires the neurosurgeon to have the proper knowledge of treatment for the diseases that affect the region [21,23-26]. MTLE represents about two thirds of the population undergoing surgical treatment with seizures refractory to treatment [1,25].
SAH is a widespread surgical technique used in cases of refractory psychomotor seizures [22]. In 1973, Wieser and Yasargil introduced the transsylvian approach for the mesial temporal lobe structures resection [2,22].
In 2018, we celebrate 60 years of the original description of Niemeyer's approach. It also encouraged several neurosurgeons to apply other access routes to the SAH. At the Epilepsy Center at the IECPN, the standard transventricular approach is usually performed.
This paper is a retrospective study and data analysis of results of patients undergoing SAH by transventricular approach at IECPN between August 2013 and October 2015.
MTLE diagnosed patients, refractory to AEDs treatment, VEEG consistent results visualized on MRI, diagnosed as HS and undergoing SAH, were included in this study. While those, with tumor or other cause induced MTLE, or who underwent nonselective amygdalohippocampectomy, were not.
All patients underwent MRI scans to show HS signals. T2 and STIR sequences in coronal were used to study the mesial temporal region.
After general anesthesia, patients were placed in the surgical supine position, with the head lateralized and deflected. This deflection is extremely important to expose the mesial structures (Figure 1). A Temporal craniotomy was performed.
 Figure 1: Surgical position: Supine position with a pad under the ipsilateral shoulder, head lateralized to 45 degree and deflected.
View Figure 1
Figure 1: Surgical position: Supine position with a pad under the ipsilateral shoulder, head lateralized to 45 degree and deflected.
View Figure 1
The transventricular approach was performed with the aid of a surgical microscope and neuronavigation with the MRI images [27]. Then when the intraventricular structures (choroid plexus, choroidal fissure, amygdala, hippocampus, lower choroid point and collateral sulcus) were located, an ultrasonic aspirator was used for the amygdala aspiration.
The arachnoid membrane and the relationship of the amygdala with the optic tract and basal ganglia were the aspiration limits. Then the fimbriae and the hippocampus were dissected to expose the arachnoid, which limits the hippocampus and the cistern Ambiens.
The fimbriae and hippocampus were then dissected, and with arachnoid exposure, which limits the hippocampus and the Ambiens cistern. En bloc resection of the hippocampus, about 2.5 to 3.0 cm as well as resection of the parahippocampal gyrus are performed (Figure 2A, Figure 2B, Figure 2C and Figure 2D).
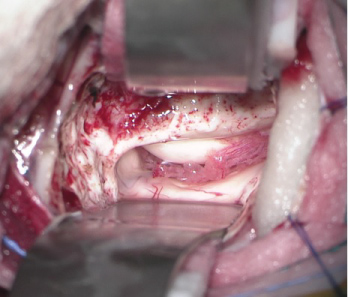 Figure 2A: A) Right intraventricular microscopic view with exposure of the amygdala, hippocampus and choroid plexus;
View Figure 2A
Figure 2A: A) Right intraventricular microscopic view with exposure of the amygdala, hippocampus and choroid plexus;
View Figure 2A
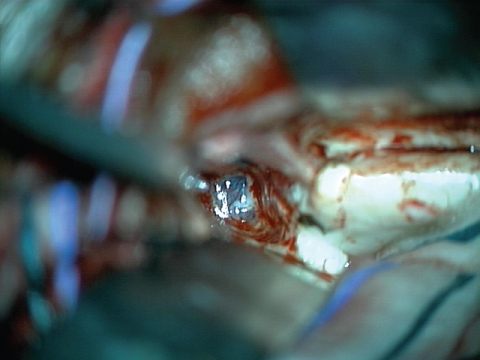 Figure 2B: B) Right intraventricular microscopic view, after aspiration of the amygdala, with exposure of the arachnoid membrane and anterior relation to the head of the hippocampus;
View Figure 2B
Figure 2B: B) Right intraventricular microscopic view, after aspiration of the amygdala, with exposure of the arachnoid membrane and anterior relation to the head of the hippocampus;
View Figure 2B
 Figure 2C: C) Right intraventricular microscopic view, after aspiration of the amygdala, with exposure of the arachnoid membrane and anterior relation to the head of the hippocampus;
View Figure 2C
Figure 2C: C) Right intraventricular microscopic view, after aspiration of the amygdala, with exposure of the arachnoid membrane and anterior relation to the head of the hippocampus;
View Figure 2C
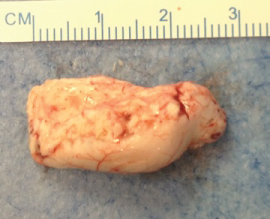 Figure 2D: D) Surgical specimen (hippocampus) after an block resection through SAH.
View Figure 2D
Figure 2D: D) Surgical specimen (hippocampus) after an block resection through SAH.
View Figure 2D
Follow up of patients undergoing SAH is made by neurosurgeons and neurologists one week, one month, six months, one, two and five years after surgery. Postoperative brain MRI is requested of patients to evaluate the surgical resection area.
The Engel Class is used for surgical outcomes of patients. During the study, initiated request of pre and postoperative campimetry to evaluate possible deficit in the visual field.
All hippocampus obtained from resection were fixed in 10% buffered formalin to be thoroughly evaluated in the neuropathology laboratory. Coronal sections of the hippocampus were processed for paraffin embedding and sections were stained with hematoxylin and eosin. Patients undergo neuropsychologist's assessment before and after the procedure, in which overall quality of life, memory, cognition and concern for epileptic seizures are part of the interview. The QOLIE-31 score is then deployed to neuropsychological results.
Evaluations of possible surgical complications such as wound infection, CSF leaks, hydrocephalus, esthetic result, motor or sensory deficits and death shall be carried out.
Until October 2015, 2597 surgeries had been performed at IECPN. Of these 1000 endovascular procedures 13 SAH and 76 epilepsy surgeries. The last include callosotomy, vagal nerve stimulator, mesial temporal tumors, lesionectomy for cases of cortical dysplasia, hemispherectomy, foramen ovale electrode and, selective and nonselective amygdalohippocampectomy procedures. This last is performed associated with anterior temporal lobectomy. Figure 3 details the number of Epilepsy Center surgeries.
 Figure 3: Epilepsy Center Surgeries at the IECPN. (SAH = Selective Amygdalohippocampectomy; NSAH = Non-Selective Amygdalohippocampectomy; VNS = Vagus Nerve Stimulation; DBS ANT = Deep Brain Stimulation - Anterior Nucleus Thalamus; FO Electrode = Foramen Ovale Electrode).
View Figure 3
Figure 3: Epilepsy Center Surgeries at the IECPN. (SAH = Selective Amygdalohippocampectomy; NSAH = Non-Selective Amygdalohippocampectomy; VNS = Vagus Nerve Stimulation; DBS ANT = Deep Brain Stimulation - Anterior Nucleus Thalamus; FO Electrode = Foramen Ovale Electrode).
View Figure 3
The 13 patients undergoing SAH in this period represent 0.03% of the total IECPN surgeries and 17.2% of Epilepsy surgeries. Regarding gender, 8 (61.5%) were male and 5 (38.5%) female. The mean age of study was 37.4 years and of seizure onset was 13.5 years. The disease duration between 7 and 47 years; 46.2% of the patients had higher education; 23.1% had a family history of epilepsy; 38.5% of these patients had some type of memory complaints in the initial evaluation. 69.3% were right-handed, 23.1% left handed and 1 ambidextrous patient. Only 3 patients had some initial precipitating event that led to seizures, like encephalitis, a febrile seizure or head trauma. The frequency of MTLE in these patients ranged from four times a week to four seizures per month. No patient included had history of status epilepticus. There were no deaths among the operated patients. Results are detailed in Table 1.
Table 1: Results of patients underwent SAH at the IECPN. View Table 1
AEDs were used in the medical treatment of patients and usually with some kind of association.
All patients undergoing SAH and included in this study, were diagnosed with HS. Regarding laterality, 8 (61.5%) patients had right mesial temporal sclerosis, visible in the brain MRI, and 5 (38.5%) left. The semiology of the seizures was consistent with the laterality of temporal focus detected, temporal right or left.
SAH was performed 61.5% on the right side and 38.5% on the left. At IECPN, T2 and STIR sequences in coronal images were the main preoperative study. These are very important for surgical planning. in which the pathway to access the temporal horn of the ventricle were measured to verify if they are consistent with middle temporal gyrus for transcortical approach, as described by Niemeyer [22], and also reported by Spencer [2]. Depending on the individual anatomy of each patient MRI was useful to study of the sulcus, the thickness and size of the temporal gyrus, depth of the sulcus, these characteristics also cited by another Brazilian study [28].
Follow up of patients undergoing SAH was made by neurosurgeons and neurologists during the last five years. However, some patients are still within this follow-up term.
Engel classification was used in surgical outcomes, but we compared the results with ILAE classification. Of the patients undergoing SAH, 84.6% (11) were classified as Engel I and remained seizure free, 2 patients (15.4%) Engel II; as to ILAE classification, 69.2% (9) were ILAE 1; 2 patients ILAE 2 and 2 operated as ILAE 3.
Surgical specimens of the hippocampus were analyzed by neuropathology and 100% of the samples had changes consistent with HS. They were characterized by neuronal cell loss and gliosis at CA1 and CA4 regions (Figure 4).
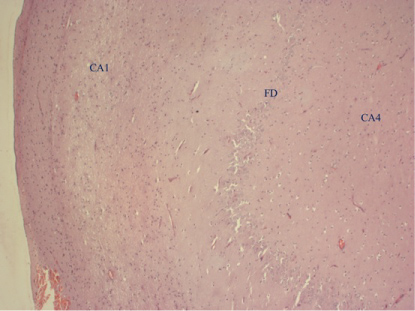 Figure 4: Hippocampal sclerosis. Note the neuronal loss in CA1 and CA4 regions and also fewer neurons in the Fascia dentata (FD). Bar = 200 µm.
View Figure 4
Figure 4: Hippocampal sclerosis. Note the neuronal loss in CA1 and CA4 regions and also fewer neurons in the Fascia dentata (FD). Bar = 200 µm.
View Figure 4
In the middle of study, pre and postoperative campimetry of patients, were implanted. So it is not possible to have reliable evaluation of the data, however, 2 patients showed no change and their visual field remained intact. Another fact is that there have been no complaints about the visual field by operated patients. As to neuropsychology, patients report significant improvement in quality of life and the social sphere, particularly the improvement of seizures. QOLIE31 score, which evaluates results as cognition, physical health, quality of life and emotional conditions patients has been implanted with more routine use at the hospital.
Postoperative follow-up was performed by neurosurgeons and epilepsy neurologists. Patients were evaluated in general and brain postoperative MRI was made to evaluate the surgical resection of mesial structures (Figure 5A and Figure 5B).
 Figure 5A: A) T2 - weighted coronal MRI showing a right-side hippocampal sclerosis;
View Figure 5A
Figure 5A: A) T2 - weighted coronal MRI showing a right-side hippocampal sclerosis;
View Figure 5A
 Figure 5B: B) Post-operative coronal T2 - weighted MRI showing right side resection of mesial temporal structures.
View Figure 5B
Figure 5B: B) Post-operative coronal T2 - weighted MRI showing right side resection of mesial temporal structures.
View Figure 5B
Surgical follow-up was 5 years, but the latest surgery of this period had a shorter follow up and patients undergoing SAH must be accompanied for longer terms for better conclusion of the results after surgery. This is due to the fact that IECPN was inaugurated and started activities only five years ago.
In 1973, Wieser and Yasargil published the SAH by transsylvian approach [2,21,29]. Through the Sylvian fissure, Yasargil supported the hypothesis that it was possible to perform the lesionectomy and avoid trauma to adjacent structures, cortical, subcortical temporal, as well as cortical vessels. It comprises a pterional craniotomy and about 3 to 5 cm opening of the anterior portion of the fissure, a 15-20 mm pial incision lateral to the M1 segment of the Middle Cerebral Artery (MCA), between the origins of the polar and anterior temporal artery. After dissection of the fissure, the amygdala is removed in its laterobasal portion towards the ambiens and crural cisterns. The temporal horn is then accessed and the hippocampus and parahippocampal gyrus approached and resected. The results for seizure control were also satisfactory, since the structures involved in MTLE were resected [30].
Over the last four decades, efforts have been focused on making smaller and less invasive resections [31-33]. The advent of increasingly modern surgical microscopes led to the adaptation of epilepsy surgeries to modern microsurgery and the increasingly precise diagnosis instigated different approaches to the MTL, trying to minimize the damage of adjacent structures. Transcortical, transsylvian, trans sulcal, transcisternal, subtemporal or transtentorial and even endoscopically accesses were developed. The use of microsurgery and other devices such as the ultrasonic aspirator, functional MRI and neuronavigation, caused a decrease in postoperative morbidity and, at the same time, an improvement in the number of Engel class I results, where patients are free or have rare seizures [31-36].
Other accesses have arisen over time as variants of the anterior supraorbital craniotomy, where the orbital border and the zygomatic process of the frontal bone are removed, also called minimodified orbitozygomatic craniotomy. Spetzler uses this access for lesions in the circle of Willis and Sylvian cistern and, based on this experience, the mesial temporal structures and the crural cistern were exposed by a group of the Barrow Neurological Institute (Figueiredo, et al.), They claim to have an appropriate previous surgical corridor. A microsurgical technique for anterior-guided SAH imaging was then described [37].
Thudium, et al. report that the subtemporal access, described before, as an access rout through the fusiform gyrus to access the temporal horn for more caudal resection of the amygdala and hippocampus, presented benefit in relation to cognition and avoided optical radiations injury. They also related the use of Meyer's loop diffusion tensor treatment and its implementation in neuronavigation for visualization during microsurgery, but these findings need to be studied in larger series [38].
A cadaveric study by Bahuleyan B, et al. explains the endoscopic transventricular access for SAH. Occipital trepanation is performed and the MTL structures are accessed via the transventricular route. Through the occipital horn the endoscope is advanced to the atrium, where two cavities are seen, the smallest is the temporal horn and the largest is the lateral ventricle body. The temporal horn is accessed and the hippocampus, amygdala, choroid plexus, choroidal fissure and collateral eminence are visualized, and then the SAH is performed. In this study, the authors describe endoscopic anatomy before and after resection and also report the advantages, the most important of which is to minimize damage during SAH, and disadvantages of this access path [39].
The best access to SAH is that one the neurosurgeon knows best and is still a subject of debate among surgeons around the world [17,37,38].
Meyer's loop is the most vulnerable part of the optical radiations in the temporal horn and MTL accesses and is usually found during SAH. Damage to the anterior portion of the optical radiation fibers, Meyer's loop, often results in visual field deficiency with superior homonymous quadrantanopia. In anterior temporal lobectomy surgery, the damage is related to the extent of resection in 50-90% of cases [40,41].
Yeni, et al. published their results of visual field deficits following transsylvian SAH in patients with MTLE due to HS. They used the approach described by Yasargil [30]. All 30 patients in the study had visual field normal on preoperative examination and after the procedure, 36.6% had visual field deficits. As expected, the deficit was superior quadrantanopia, in its various degrees. However, all patients with visual impairment were free of postoperative seizures, but this may be coincidental since there was no significant difference in Engel I and non-Engel I class patients with quadrantanopia (P > 0.05) [41]. Yeni, et al. Also mention other series, not only with HS, but also with tumors of uncus, hippocampus, amygdala; transsylvian and transcortical via also presented quadrantanopia with the superior homonymous quadrantanopia [41].
Memory deficit and intellectual cognitive impairment may also be associated, as reported by Beaton, et al. Some characteristics such as comprehension, verbal memory and also in immediate visual memory in some cases showed improvement after surgery, and others as facial memory remained stable [12,42-44].
Another complication is cerebral vasospasm, cited by Lackner, et al., where 32.7% of the patients developed vasospasm after epilepsy surgery, including SAH, 16.8% ipsilateral to the surgical procedure and 15.9% diffuse cerebral vasospasm [2,45].
Complications inherent to neurosurgical procedures such as bleeding, ischemia, infection, meningitis, cerebrospinal fluid leak, incomplete resection, reoperation for better seizure control and death may also occur, in addition to mood disorders [12,20,46,47]. There was no death, infection and CSF leakage in our series.
Temporal lobe epilepsy is a complex and difficult to control disease. A challenge for neurologists and neurosurgeons. With the advent of technologies there has been an expressive improvement in resection of the amygdala and hippocampus.
The majority of patients undergoing to Niemeyer's technique at the IECPN were classified Engel class I, as free from seizures or with rare seizures and patients showed improvement in general quality of life. The benefit of SAH can be verified in the surgical results of this study as well as several series during the last 60 years,
Own funding.
None.