We present an unusual case of a 60-year-old female who developed subtle, new-onset left upper and lower extremity weakness on day five after perioperative thoracic epidural placement. The onset of a focal neurological deficit in any patient undergoing epidural anesthesia usually raises suspicion for the presence of an epidural hematoma, abscess, or traumatic cord lesion. However, in this patient, brain imaging revealed a large, occult intracranial mass. Classically, the risk of mass related intracranial pressure shifts leading to neurological changes is associated with spinal techniques, including diagnostic lumbar puncture, combined-spinal epidural catheter analgesia, and unintended dural puncture during epidural placement. In the context of other similar reports, we report that tumor related neurological changes may present after uncomplicated thoracic or lumbar epidural as well. Symptom onset ranges from six hours to ten days and can be highly variable, depending on tumor location and may include headache, vision changes, focal deficits, or alterations of consciousness. Further studies would be necessary to establish causation between the epidural technique and changes in cerebrospinal fluid pressures leading to symptom onset. Though rare, this is a time sensitive diagnosis that should be considered for any patient with unexplained neurological findings after neuraxial anesthesia.
Epidural analgesia, Focal neurologic deficits, Complication, Postoperative, Elevated intracranial pressure, Meningioma, Central nervous system disorders, Intracranial
CSF: Cerebrospinal Fluid; CT: Computed Tomography; EVD: External Ventricular Drain; GIST: Gastrointestinal Stromal Tumor; ICP: Intracranial Pressure; MRI: Magnetic Resonance Imaging; POD: Post-operative Day
The differential diagnosis for focal neurological findings after neuraxial anesthesia includes epidural hematoma, epidural abscess, meningitis, traumatic cord lesion, and cauda equina [1-3]. Epidural hematoma is the most common cause, with a variable rate of incidence depending on the population studied, from 1/168,000 in obstetric epidurals [4] to 1/3,600 in elderly females undergoing knee arthroplasty [1]. Infectious and traumatic complications are comparatively less common but are prevalent enough to be reported in cross sectional studies [1-3]. Intracranial processes such as stroke after cervical epidural [5] or after spinal anesthesia [6] or brain masses causing neurological deficits after epidural or spinal anesthesia procedures [7-11] are rare, and only reported on a case report basis.
Although the presence of a headache can sometimes help to guide the differential towards an upper versus lower motor neuron lesion, diagnosis is confounded in this situation by the relatively common occurrence of post-dural puncture headache. A high degree of vigilance is warranted for patients with headache after a neuraxial procedure, as intracranial masses can cause rapid decompensation. One case report describes the sequela of a labor epidural complicated by an unintended dural puncture. Initial complaints of headache were followed by fatal deterioration only two hours later. Imaging revealed an intracranial mass, but a tissue diagnosis was not obtained [12].
The contraindication to perform neuraxial anesthesia in the setting of elevated intracranial pressure (ICP) [13], particularly in the presence of an intracranial mass, was initially based on case reports of herniation after diagnostic lumbar puncture procedures with large bore needles and large volume cerebrospinal fluid (CSF) withdrawal [14]. Although epidural techniques are considered to have a lower risk of complication compared to spinal anesthesia, they do carry a risk of inadvertent dural puncture [13]. Refinements in technique, such as the use of small gauge pencil-point needles, have reduced complications such as CSF leak and post-dural puncture headaches [14]. Such refinements hypothetically lower the risk of ICP changes and CSF shifts that would result in neurologic complications, but the exact risk reduction is unknown. In a detailed review of 41 cases of neuraxial techniques in a variety of cases with known elevated ICP, most outcomes were, in fact, uneventful [15].
Though additional studies would be needed to establish a causal relationship between epidural access and symptom onset due to intracranial process, a proposed mechanism relates to the relative shifts in intracranial pressures. Epidural injection causes a transient increase in ICP, generally lasting for three to seven minutes in healthy patients and producing no adverse effects [16]. However, in pathological states with elevated ICP, this increase can potentially compromise blood flow to the brain and spinal cord [17,18]. Hilt, et al. measured the effect of extradural injection of local anesthetic on patients with altered cerebral compliance and demonstrated a significant increase in ICP due to lumbar dural sac compression with cranial shift of CSF [18].
A 60-year-old female patient with a past medical history of asthma and hyperlipidemia presented to our tertiary care hospital's hepatobiliary surgery clinic with symptoms of nausea, vomiting, diarrhea, abdominal pain, and ten-pound weight loss. Magnetic resonance imaging (MRI) of the abdomen and pelvis demonstrated a 6.7 cm hypodense lesion of the pancreas which was concerning for possible neuroendocrine tumor. Biopsy samples collected under endoscopic ultrasound noted atypical cytology consistent with possible mucinous neoplasm. Computed tomography (CT) of the chest demonstrated no evidence of metastasis. Due to the interval increase in the size of the mass along with the patient's progression of symptoms, the patient was scheduled for a pancreaticoduodenectomy (Whipple procedure).
For post-operative pain control, a thoracic epidural catheter was placed at the T9-10 interspace via a paramedian approach with loss of resistance to saline using a 17-gauge Tuohy needle. The needle placement was uncomplicated, and there was a loss of resistance at 6 cm with no return of cerebrospinal fluid or blood. The catheter was threaded to a depth of 12 cm.
The operation proceeded uneventfully. Microscopic sections of the specimen obtained demonstrated fascicles of spindled cells, some of which with epithelial features and background collagen (Figure 1A). The tumor cells were positive for DOG1 (Figure 1B) and CD117, consistent with gastrointestinal stromal tumor (GIST).
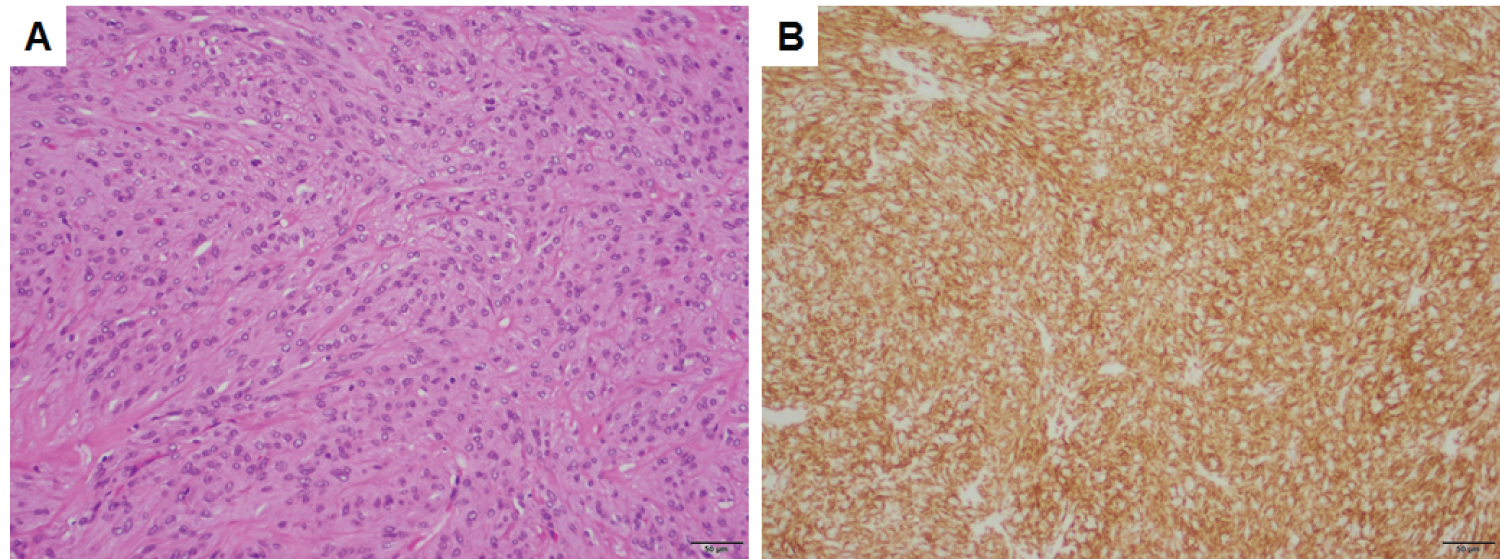 Figure 1: Gastrointestinal stromal tumor. A) Spindled and epithelioid cells with intervening collagen; B) Immunopositivity for DOG1. Both panels are taken at a total magnification of 100×, scale bars = 50 μm. View Figure 1
Figure 1: Gastrointestinal stromal tumor. A) Spindled and epithelioid cells with intervening collagen; B) Immunopositivity for DOG1. Both panels are taken at a total magnification of 100×, scale bars = 50 μm. View Figure 1
Post-operatively, an epidural infusion of 0.0625% bupivacaine with 2 mcg/ml of fentanyl was initiated at a rate of 6 ml per hour. The epidural functioned well, providing analgesia without motor block. The next day, the patient was started on enoxaparin 40 mg daily for DVT prophylaxis. The patient was ambulating on post-operative day two. On post-operative day four, enoxaparin was held in anticipation of possible epidural removal. Platelet counts were within normal limits.
On post-operative day five, with the epidural infusion stopped, the patient noted subtle left upper and lower extremity weakness and complained of a mild headache. Nursing staff and physical therapists noted unequal gait phases on ambulation. Neurological exam showed 4-/5 foot dorsiflexion and 4/5 foot plantarflexion, 4+/5 grip strength, and 4-/5 elbow extension on the left side. There were no other deficits on a complete neurological exam. The epidural was gently removed without difficulty and noted to be intact.
Although epidural hematoma would be the most common reason for unilateral deficits, the level of the epidural was too low to affect the upper extremity. Furthermore, the patient had no risk factors for epidural hematoma such as coagulopathy, renal dysfunction, or difficult epidural placement. Due to the lack of any fever, leukocytosis or tenderness at the epidural site, an epidural abscess was also felt to be unlikely. Thus, an upper motor neuron lesion was suspected. However, the patient had minimal risk factors for stroke, and no severe headache, mental status changes, aphasia, or cranial nerve deficits. The possibility of brain metastases was also considered but the incidence is extremely rare for gastrointestinal stromal tumors.
Ultimately, a CT of the head without contrast demonstrated a 5.9 × 6.5 × 5.2 cm heterogeneously enhancing mass in the right frontoparietal lobe with a small amount of surrounding edema. There was mass effect causing a midline shift of 2.5 cm at the level of the lesion, and mild effacement of the lateral and third ventricles. Neurosurgery was consulted and the patient was started on dexamethasone 4 mg every 6 hours. Ten days after the initial Whipple procedure, a right parietal craniotomy was performed for intraventricular tumor resection.
Post-operative MRI (Figure 2) demonstrated near gross total resection with a small amount of enhancement around the anterior aspect of the resection cavity. Microscopic sections demonstrated sheets and lobules of spindled to plump cells with syncytial cytoplasm (Figure 3A), background collagen, and scattered psammoma bodies, immunopositive for EMA (Figure 3B and Figure 3C), PR (Figure 3D), and SSTR2a, consistent with a diagnosis of meningioma. Figure 2B demonstrates numerous WHO grade II features, including necrosis, loss of lobular architecture, prominent macronucleoli, increased mitotic figures (focally up to 6/10 HPF), and elevated Ki-67 proliferation index (focally greater than 30%), which is associated with a high rate of recurrence. Additional immunohistochemistry was negative for CD117 (c-KIT) and DOG1, ruling out metastasis of the previously known GIST. The patient was started on imatinib therapy under the care of the oncology service. Her neurologic exam improved post-operatively to the point of having no residual neurological deficits on follow up.
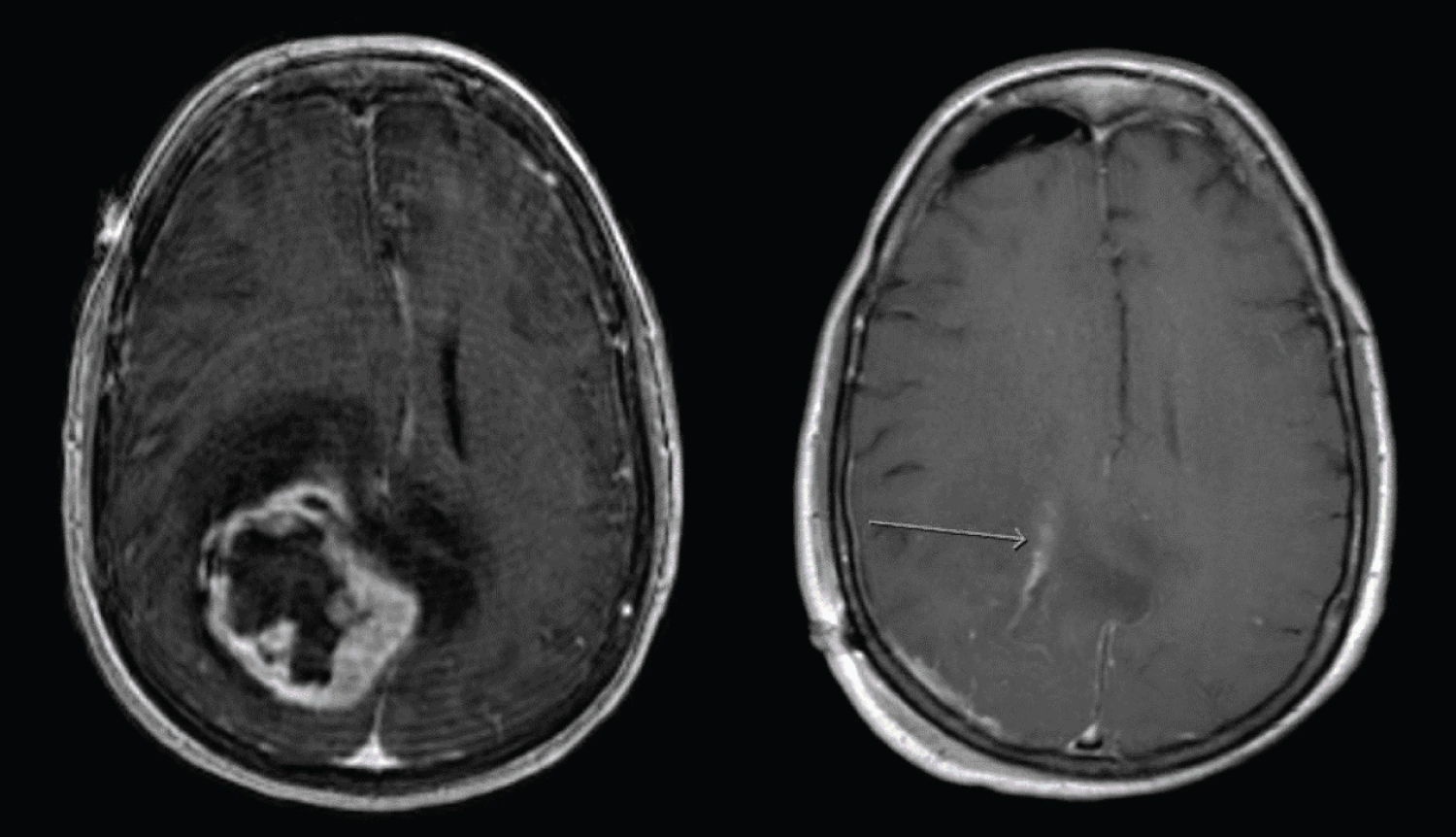 Figure 2: Pre and post-operative T1 MRI (axial view) with contrast. Post-operative imaging shows near gross total resection. View Figure 2
Figure 2: Pre and post-operative T1 MRI (axial view) with contrast. Post-operative imaging shows near gross total resection. View Figure 2
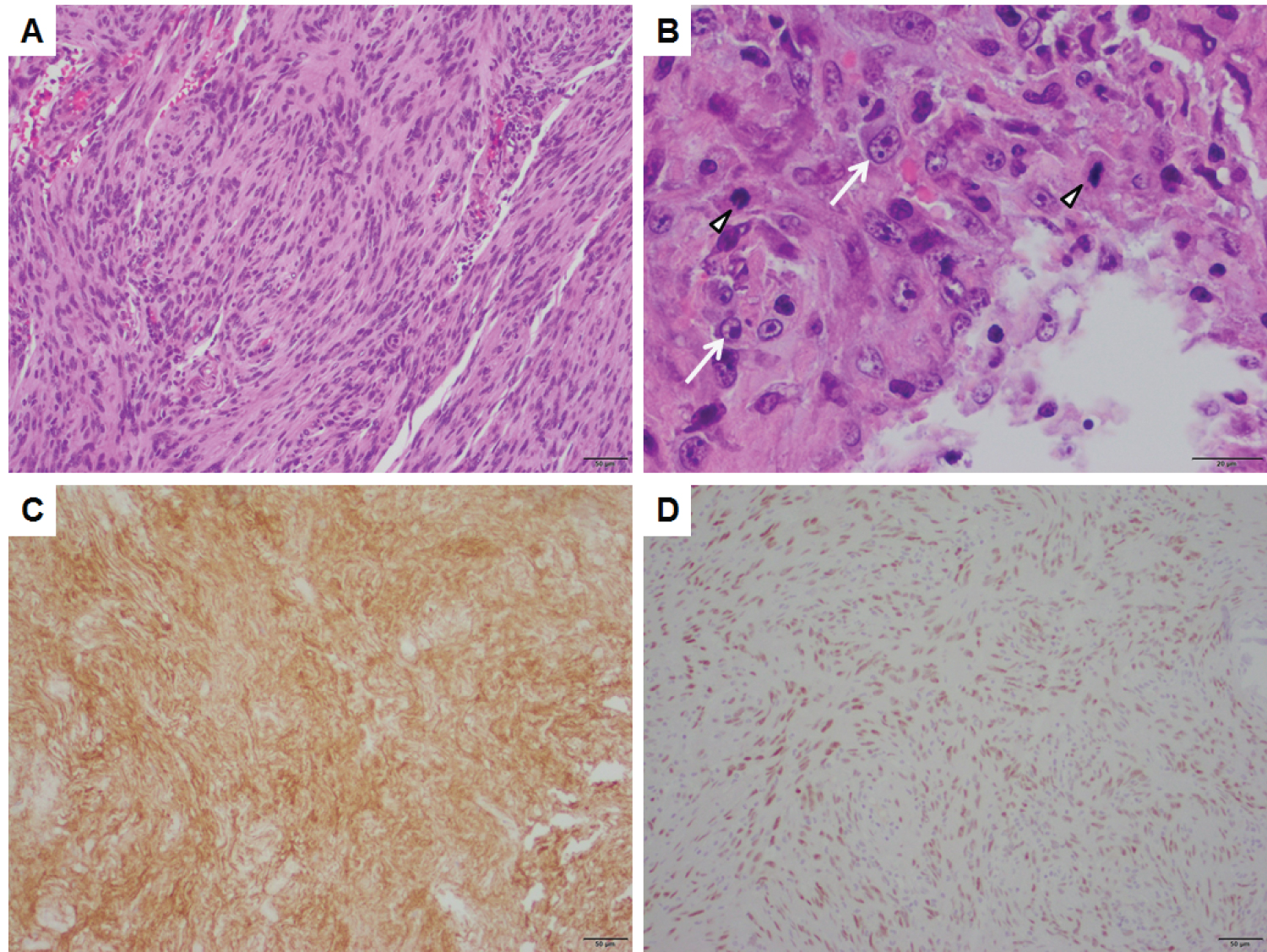 Figure 3: A typical meningioma, WHO grade II demonstrating. A) Lobules and sheets of spindled and plump cells with; B) High-grade features, including elevated mitotic figures (arrowheads) and macronucleoli (arrows). The tumor is positive for; C) Epithelial membrane antigen (EMA); D) Progesterone receptor (PR), consistent with meningioma. Panels A, C, and D are taken at a total magnification of 100×, scale bars = 50 μm. Panel B is taken at a total magnification of 400×, scale bar = 20 μm. View Figure 3
Figure 3: A typical meningioma, WHO grade II demonstrating. A) Lobules and sheets of spindled and plump cells with; B) High-grade features, including elevated mitotic figures (arrowheads) and macronucleoli (arrows). The tumor is positive for; C) Epithelial membrane antigen (EMA); D) Progesterone receptor (PR), consistent with meningioma. Panels A, C, and D are taken at a total magnification of 100×, scale bars = 50 μm. Panel B is taken at a total magnification of 400×, scale bar = 20 μm. View Figure 3
This case report describes a rare incidental diagnosis after epidural analgesia. Compared with other reports summarized in Table 1, it is the first to describe this complication after a thoracic epidural catheter placement, and the first to report focal weakness as the presenting sign [7-11]. The previous case reports consist of four females and one male, ages 49 to 86, presenting for intra-abdominal or orthopedic procedures. A variety of neuraxial techniques are represented, including spinal, lumbar epidural, and combined spinal-epidural approaches. Interestingly, the onset of neurological symptoms was highly variable, from as little as six hours to up to ten days after surgery. All five cases presented initially with alterations of consciousness such as somnolence, agitation, disorientation, or behavioral changes. Progression to unresponsiveness occurred in three out of five cases. Pupillary changes were a late sign described in two cases. In the case where the meningioma was located in the sphenoid region, the patient presented with reduced optic acuity and optic atrophy, as well as hyponatremia and urinary incontinence, consistent with possible syndrome of inappropriate antidiuretic hormone given the lesion's position in deep brain structures. Cushing's triad of hypertension, bradycardia and Cheyne-Stokes respirations was observed in one case.
Table 1: Summary of case reports of symptomatic meningioma after neuraxial anesthesia. View Table 1
Although meningioma is the most common non-malignant brain tumor, accounting for 37.6% of all central nervous system tumors [19], the probability of performing a neuraxial block in a patient with an undiagnosed meningioma is low. According to the US Central Brain Tumor Registry's 2019 report, meningiomas have an average annual age-adjusted incidence rate of only 8.6 per 100,000 [19]. It is unknown what percentage of patients with undiagnosed meningioma receive uneventful neuraxial anesthesia. Longitudinal screening studies of the general population would require such a large sample size as to be prohibitive in scope and cost.
It has been proposed that for patients with slowly growing masses, the presence of the mass per se may not represent an absolute contraindication to a neuraxial technique. Rather, it has been proposed that relative risk depends on the size and location of the mass with regard to whether it causes significant mass effect (high risk of herniation), moderate mass effect or obstruction of CSF flow (moderate risk), or no findings of increased ICP (minimal to no risk) [20]. This case-by-case approach may be reasonable, considering other routine examples of neuraxial access with raised ICP, such as diagnostic lumbar puncture for purulent meningitis, which carries only a 5% risk of herniation [21].
The obstetric literature addresses the topic of the parturient with a known intracranial mass with a variety of approaches [20]. One case report describes successful management of a patient with a meningioma using ventriculoperitoneal shunt placement prior to an uneventful cesarean delivery [22]. Taking an alternative approach to avoid exposing the fetus to general anesthesia, another team proceeded first with cesarean delivery under epidural anesthesia. The patient had worsening symptoms six hours after delivery and went immediately for craniotomy [23].
The successful management of this complication ultimately hinges on early recognition, brain imaging, and early consultation to neurology and neurosurgery. At the present time, the implementation of screening imaging prior to neuraxial analgesia is likely cost prohibitive, with a low risk-benefit ratio. It is reasonable to reserve imaging for symptomatic individuals. Alterations of consciousness in these cases were often initially presumed to be due to polypharmacy or delirium, and attempts to treat with various pharmacologic reversal or sedating agents delayed brain imaging and diagnosis in three of the cases in Table 1. Three of the studies employed measures to acutely reduce ICP after the development of symptoms. Such measures may include elevated head of bed, dexamethasone, mannitol, hypertonic saline, and optimized sedation [24]. Hyperventilation for hypocapnia should only be instituted as a last line therapy [25]. If noninvasive measures are inadequate, external ventricular drain (EVD) or shunt placement may be required [15,22,24]. Based on patient and tumor characteristics, a craniotomy or radiation therapy may be warranted.
In conclusion, it is important to recognize the potential significance of mental status changes and focal deficits in the hours to days after neuraxial anesthesia. Manifestations of an intracranial process may be difficult to distinguish from other possible post-operative or post-procedural complications. Onset of neurological symptoms may occur after any form of neuraxial access, including intrathecal, inadvertent dural puncture, and bolused or continuous infusion thoracic or lumbar epidural catheters. Though intracranial pathology has long been considered an absolute contraindication to spinal anesthesia, it is time to broaden consideration to epidural techniques as well. Further investigations are needed to examine whether the incidence of intracranial pathology is increased following epidural catheter placement.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
None.