Hairy cell leukemia (HCL) is a rare neoplasm of mature B cells histologically characterized by small lymphocytes with distinctive and circumferential cytoplasmic "hairy" projections. HCL accounts for 2% of all leukemias and less than 1% of lymphoid neoplasms with an estimated 600-800 new cases per year [1]. There is a strong male predominance with a median age of onset of 50 to 55 years [2]. Genetically, HCL is classically associated with a BRAF V600E mutation which is considered a molecular hallmark of the disease [3]. However, the absence of the BRAF mutation is reported in up to 10-20% of patients with HCL and is thought to constitute a subgroup of HCL patients (HCL-variant) with a worse prognosis [4].
HCL patients typically present with symptoms related to splenomegaly or cytopenia [5]. Neurologic involvement is rare in HCL patients with a rate of approximately 5% and is predominately related to infection secondary to associated pancytopenia [6]. To date there are three published reports of brain parenchymal involvement in HCL with variable treatment response and limited information on genetic profile [7-9]. Herein we describe a case of diffuse HCL metastases to the brain in the framework of genetic variations to aid the understanding of this rare neurologic manifestation of HCL.
A 64-year-old male presented with two months of headache, gait difficulty with frequent falls, persistent blurred vision of right eye, and poor healing wounds over his bilateral upper extremities. His past medical history was notable for hypertension and hyperlipidemia, and he was an active daily smoker with occasional alcohol use. Family history was unremarkable with no history of blood disorders. Initial examination revealed splenomegaly with multiple excoriations over his extremities. He was neurologically intact with no deficits.
Laboratory findings are summarized in Table 1. CT chest-abdomen-pelvis confirmed profound splenomegaly with a mildly prominent liver and several prominent lymph nodes (Figure 1). Peripheral blood smear demonstrated mostly agranular mononuclear cells with prominent nucleoli and occasional irregular nuclei, with some cells showing circumferential cytoplasmic projections (Figure 2). The patient underwent a bone marrow biopsy showing hypercellular marrow with increased medium-sized CD20+ B-cells in interstitial distribution. Flow cytometry performed on bone marrow demonstrated abnormal kappa-restricted B-lymphocytes positive for CD25 and CD103. The summation of these findings was diagnostic of HCL. Genetic testing performed on peripheral blood was negative for the BRAF V600E mutation seen in classic HCL and positive for MAP2K1, BCOR and DDX3X mutations, suggesting an HCL-variant.
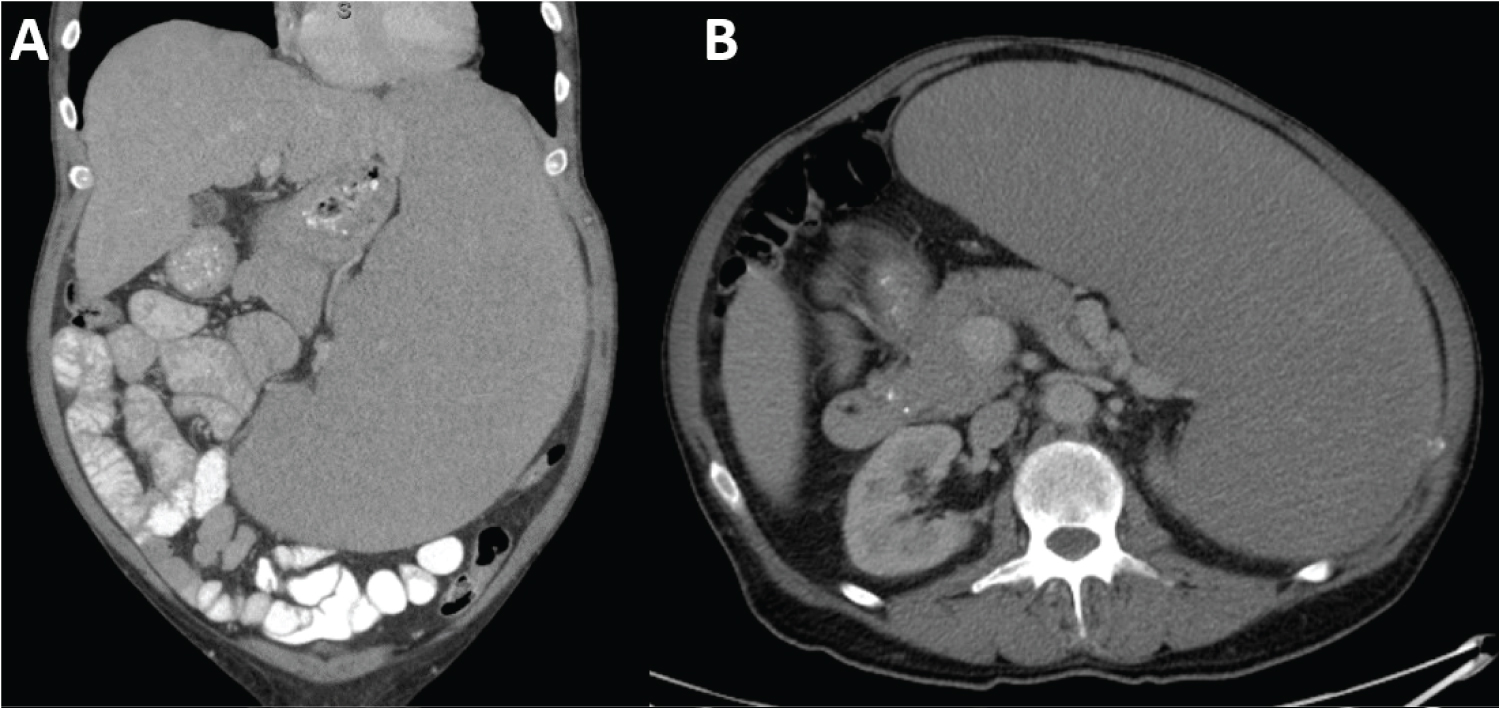 Figure 1: A) Coronal; B) Axial computed tomography scan with contrast demonstrating splenomegaly.
View Figure 1
Figure 1: A) Coronal; B) Axial computed tomography scan with contrast demonstrating splenomegaly.
View Figure 1
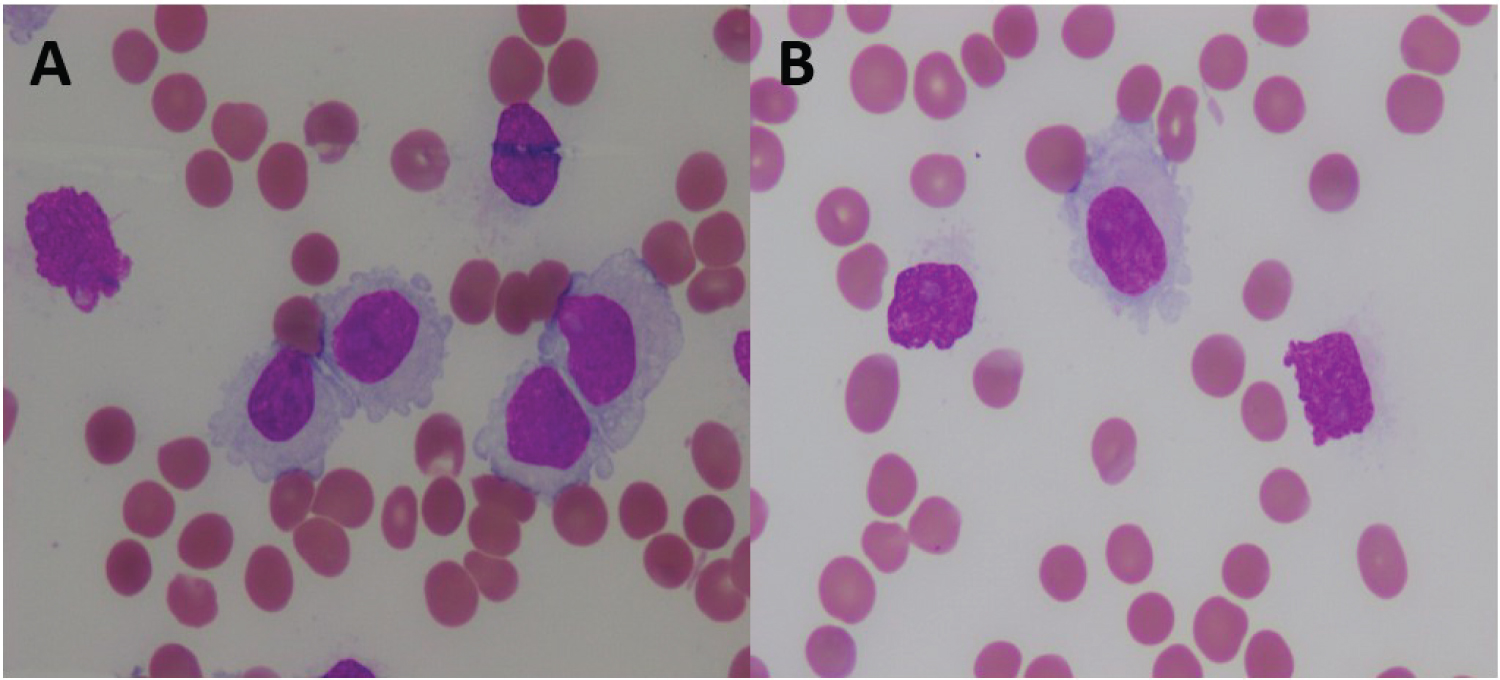 Figure 2: Intermediate-large lymphocytes with abundant cytoplasm, cytoplasmic (hairy) projections, and conspicuous nucleoli present in the peripheral blood (A and B, Wright-Giemsa stain, ×1000).
View Figure 2
Figure 2: Intermediate-large lymphocytes with abundant cytoplasm, cytoplasmic (hairy) projections, and conspicuous nucleoli present in the peripheral blood (A and B, Wright-Giemsa stain, ×1000).
View Figure 2
Table 1: CBC on initial presentation. View Table 1
Neuroimaging studies included a CT head which demonstrated bilateral supratentorial hyperdense lesions with variable degrees of vasogenic edema. MRI head with and without contrast showed innumerable T1 hyperintense rim-enhancing lesions in the bilateral cerebral hemispheres primarily concentrated in the frontal lobes (Figure 3). The diagnostic differential for innumerable rim-enhancing lesions with T1 hyperintense eccentric points included the scolex phase of neurocysticercosis in addition to the rare occurrence of HCL metastasizing to the brain. Neurosurgical biopsy was requested to resolve the diagnostic question of infection versus neoplastic etiology of the brain lesions.
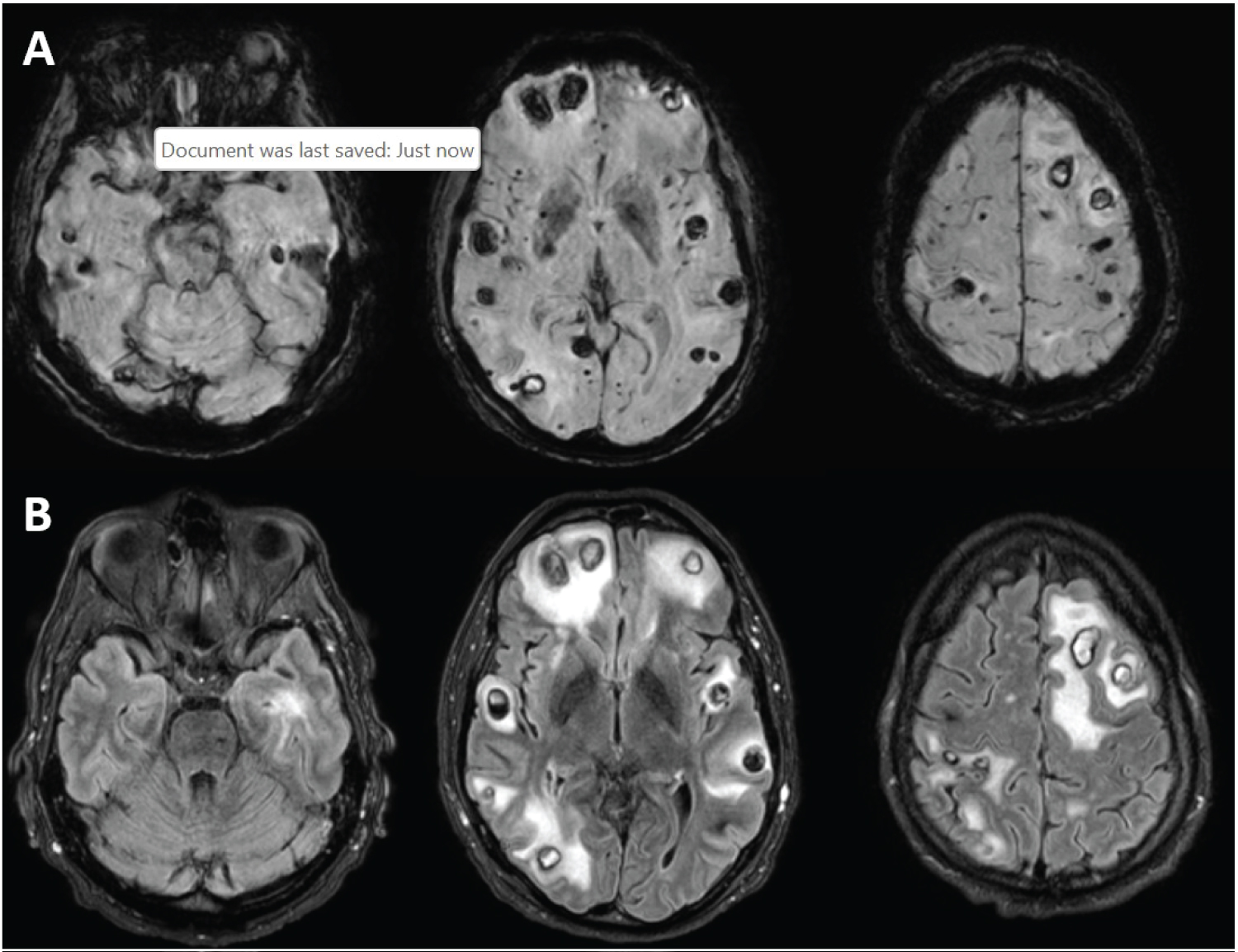 Figure 3: Magnetic resonance imaging of HCL brain metastasis (A) Axial gradient-echo (GRE) sequence demonstrating multiple microhemorrhages throughout the cortex with some brainstem involvement; (B) Axial fluid-attenuated inversion recovery (FLAIR) sequences demonstrating multiple contrast enhancing lesions with associated vasogenic edema.
View Figure 3
Figure 3: Magnetic resonance imaging of HCL brain metastasis (A) Axial gradient-echo (GRE) sequence demonstrating multiple microhemorrhages throughout the cortex with some brainstem involvement; (B) Axial fluid-attenuated inversion recovery (FLAIR) sequences demonstrating multiple contrast enhancing lesions with associated vasogenic edema.
View Figure 3
The patient was taken for left frontal craniotomy for biopsy of a superficial lesion after medical optimization of coagulopathy. Pathology results from the biopsy identified intraparenchymal malignant lymphocytes in small clusters. These cells were positive for CD20, PAX-5, BCL-6 (70%), Cyclin-D1 (50%), and CD123 (weak) with a Ki-67 index of 30% (Figure 4), while negative for annexin. Flow cytometry of the specimen demonstrated similar findings with 12% abnormal B lymphocytes positive for CD11c, CD19, CD20, CD22, CD23, CD25, CD45, CD103, and CD123. These results confirmed the diagnosis of HCL metastatic to the brain.
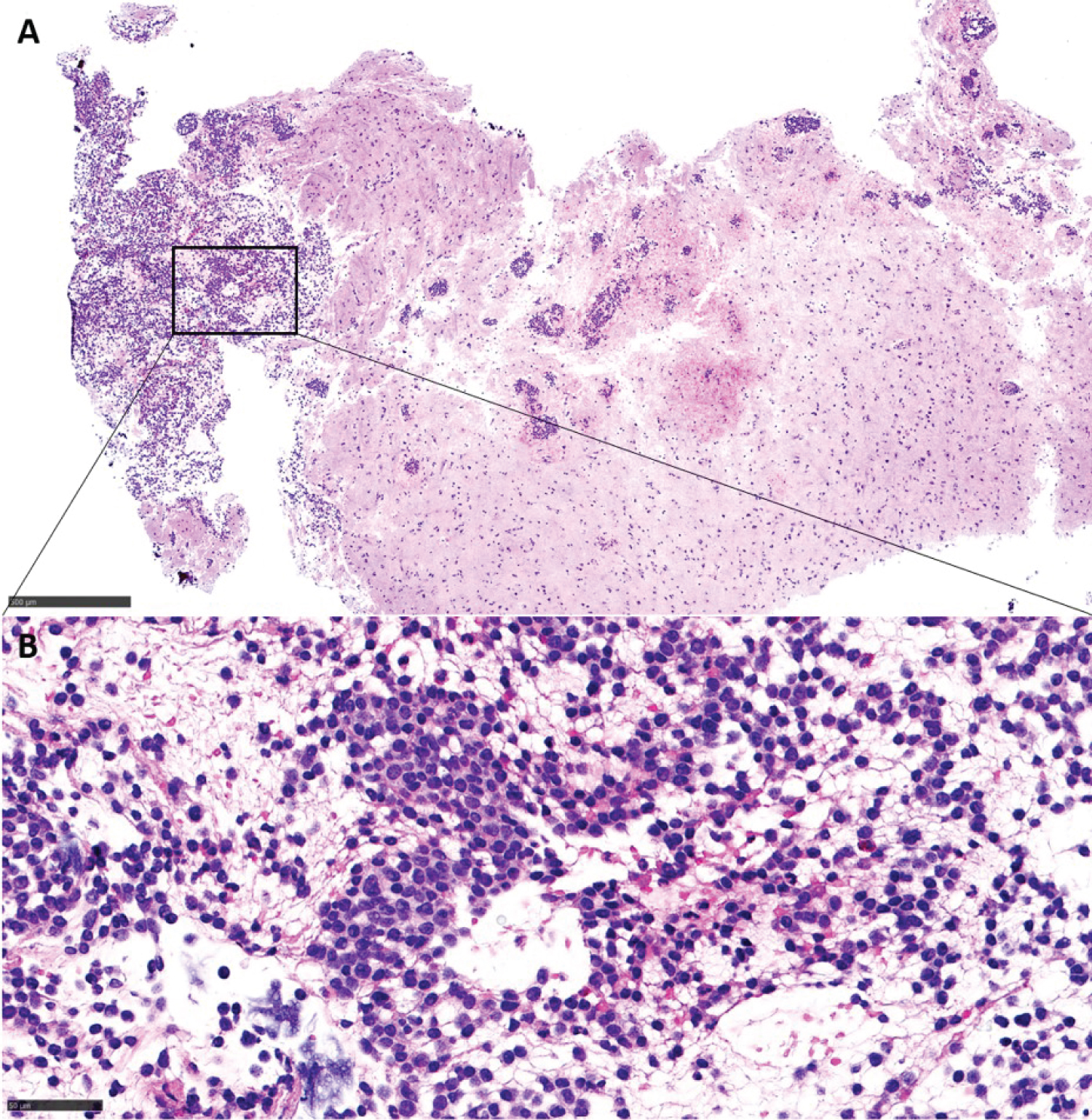 Figure 4: (A) Brain tissue with infiltration by intermediate size lymphocytes in a perivascular and interstitial patten (H&E, ×40); (B) Higher magnification showing lesional cells with abundant cytoplasm and oval nuclei (H&E, ×400).
View Figure 4
Figure 4: (A) Brain tissue with infiltration by intermediate size lymphocytes in a perivascular and interstitial patten (H&E, ×40); (B) Higher magnification showing lesional cells with abundant cytoplasm and oval nuclei (H&E, ×400).
View Figure 4
Post-operative head CT demonstrated expected postoperative changes without acute hemorrhage. The patient subsequently became increasingly agitated and impulsive throughout his hospital course. On post-operative day 6, he became lethargic and a repeat CT head at that time demonstrated interval development of a subdural hematoma with midline shift. He returned to the operating room for emergent hematoma evacuation with recovery of neurological exam to pre-operative baseline thereafter. He was monitored closely postoperatively in the intensive care unit without further complication and interval improvement in his mental status.
During the initial hospital course, the patient received 1g/day of intravenous methylprednisolone for 3 days followed by a dexamethasone taper. After discharge, he was started on standard of care chemotherapy including rituximab and ibrutinib. Less than 5 days after he was discharged home, he developed altered mental status. CT head demonstrated primary intraventricular hemorrhage in the right lateral ventricle with ventriculomegaly. On presentation he had thrombocytopenia with platelets of 30,000/mL and coagulopathy with INR elevated to 1.4. Goals of care discussions were held with the family regarding his prognosis and possible treatment options in the setting of recurrent intracerebral hemorrhage with coagulopathy and HCL. The patient was transitioned to comfort measures in keeping with his wishes.
This report provides the clinical, pathological, and genetic description for HCL metastatic to the brain to provide further understanding into the outcomes of this rare phenomenon. The patient underwent rapid decline with death less than 60 days after diagnosis of both HCL and brain involvement. The role of HCL subtypes in brain intraparenchymal involvement and outcomes remain in question.
Of the 3 published cases of HCL with brain involvement, 2 featured rapid clinical deterioration similar to this case. The first reported case was a 35-year-old male with 5 months of rapid clinical deterioration following HCL diagnosis in which cerebral parenchymal involvement was discovered post-mortem [7]. The second case was a 51-year-old male with leukocytosis of 60,000/µl treated with high-dose steroids, methotrexate, and cladribine from which he developed anemia, thrombocytopenia with a subsequent gastrointestinal bleed, and neutropenia with sepsis. He ultimately died from hemodynamic instability 66 days after initial HCL diagnosis [8]. The third case was a 42-year-old male with a leukocytosis of 37,700/µl diagnosed with classic HCL (positive for BRAF V600E mutation). He underwent treatment with cladribine and rituximab after which his blood counts returned to normal levels with repeat MRI showing resolution of the acute brain lesions at 9-months post-treatment [9]. This third case is the only report in which molecular study data is available.
While this case demonstrates many classic features of HCL that enabled pathologic diagnosis, there were several immunophenotypic findings suggestive of an HCL variant. These included the atypical morphology in peripheral blood showing prominent nucleoli, lack of annexin expression in the brain infiltrate, weak CD123, expression of BCL6, and the absence of BRAF V600E mutation with the presence of MAP2K1 mutation, which can be seen in about 42% of HCL variants and less frequently in classic HCL [10]. These findings are in contrast to the immunohistochemistry described by Perry, et al. which was positive for CD123 and negative for BCL6 [9]. The limited information regarding HCL-classic and HCL-variant subtypes in the first two reported case prevent any meaningful extrapolation of clinical outcomes of HCL brain metastasis and molecular phenotype. Further investigation and analysis of the mechanism by which HCL metastasizes to the brain is needed to adequately assess this relationship.
This case highlights the utility of brain biopsy in HCL patients. As noted in the previous reports, there was initial concern for underlying infection, rather than metastasis given the rarity of the phenomena. Data regarding the incidence and etiology for cerebral infections in HCL patients remains sparse. Radiographically similar to the case reported by Perry, et al., this patient demonstrated diffuse microhemorrhages on GRE sequences of the MRI [9]. This may suggest some means to raise clinical suspicion for metastatic disease in HCL when possible infectious etiology is being considered.
The present case details the clinical course of the fourth documented case of HCL brain metastases. Ultimately, this offers more insight into our limited understanding of HCL brain metastases with the hope of facilitating future work into this rare pathology, especially as understanding of molecular subtypes continues to expand.