

International Journal of Cancer and Clinical Research
Web-Based Quality of Life Questionnaire Followed by Paper-Based Questionnaire for the Non-Responders: Daily Practice in Patients with Prostate Cancer
Tillier CN1*, van Stam MA2, de Blok W1, van Muilekom HVM1, Bloos-van der Hulst J1 and van der Poel HG1
1The Netherlands Cancer Institute, Amsterdam, The Netherlands
2University Medical Center, Utrecht, The Netherlands
*Corresponding author: Corinne Tillier, NKI-AVL, Urology Department, The Netherlands Cancer Institute, Plesmanlaan 121, 1066 CX Amsterdam, The Netherlands, Tel: +31-205121983, Fax: +31-205126257, E-mail: c.tillier@nki.nl
Int J Cancer Clin Res, IJCCR-2-015, (Volume 2, Issue 2), Research Article; ISSN: 2378-3419
Received: March 27, 2015 | Accepted: April 10, 2015 | Published: April 13, 2015
Citation: Tillier CN, van Stam MA, de Blok W, van Muilekom HVM, Bloos-van der HJ, et al. (2015) Web-Based Quality of Life Questionnaire Followed by Paper-Based Questionnaire for the Non-Responders: Daily Practice in Patients with Prostate Cancer. Int J Cancer Clin Res 2:015. 10.23937/2378-3419/2/2/1015
Copyright: © 2015 Tillier CN, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Purpose: Patient-related outcome measures (PROMS) play an increasingly important role in the planning and evaluation of medical care. A high response rate is crucial to get a good view of the patient population. Quality of life questionnaires in oncology are important in order to evaluate the impact of the disease or the treatment of cancer patients and guide treatment decisions. The traditional way to collect data is a paper-based questionnaire sent by post. However, online questionnaires seem an attractive and cheap way to send a survey.
In this study we describe our experience with the introduction of digital questionnaires in daily practice and study factors that affect the response rate.
Methods: The study design was an observational cohort study of patients who had a localized prostate cancer and underwent a Robot Assisted Radical Prostatectomy (RARP) at our institute. Validated questionnaires were mailed to the patients before the RARP and subsequently, 6 months, 1 and 2 years after surgery. After sending twice a digital questionnaire and without any response, we sent the patients a paper-based questionnaire with a stamped return envelope.
Results: The response rate was higher when a reminder paper-based questionnaire was sent to the patients who did not respond to the web-based questionnaire. Furthermore, the elderly patients respond significantly more often than younger patients to both questionnaires (web-based or paper-based). Age was the strongest predictive factor for response on quality of life questionnaires. The fact that the patient no longer came to our institute for follow-up had no negative influence on the response rate.
Conclusion: To our knowledge there is no previous study that has explored the response of web-based and paper-based quality of life questionnaires in patients with prostate cancer in a sequential setting. Response rate was significantly higher in older men.
Key words
Localized prostate cancer, Radical prostatectomy, Web-based quality of life questionnaire, Paper-based quality of life questionnaire, Response rate questionnaire
Introduction
Patient-related outcome measures (PROMS) play an increasingly important role in the planning and evaluation of medical care. A high response rate is crucial to get a good view of the patient population. The traditional way to collect data is a paper-based questionnaire sent by post. However, online questionnaires seem an attractive and cheap way to send a survey.
Nowadays, almost everyone in The Netherlands has access to the internet. The Netherlands is since 2011 the European country where the household Internet access is the highest on 94% [1]. Therefore, it is not surprising that digital quality of life questionnaires are attractive for research purposes. For several years web-based questionnaires are sent to patients. There are several advantages of web-based questionnaires compared with paper-based version: it is cheaper to send a questionnaire by email than by post [2], it is easier and faster to send a reminder email for the non-responders [3], but above all, the data can be easily processed in a computer program without any possibility of errors due to the manual transcription of the paper-based data�s in a database. The use of a digital questionnaire is also environmentally friendly.
Internet use under elderly people has increased strongly the past few years. In the Netherlands alone, the access to the internet for people aged 65 and older has been increased from 54% in 2007 to 81% in 2012 [4]. The incidence of prostate cancer increases with age, particularly from the age of 65 onward [5]. Almost 50% of all newly diagnosed patients are above 69 years [6]. Although web-based questionnaires seem to be particularly attractive to a younger population [7], when patients have a choice between web-based and paper-based questionnaires, they are likely to choose a paper-based questionnaire irrespective of age [8].
The online, validated quality of life questionnaires are since November 2011 routinely sent to patients with localized prostate cancer in the Netherlands Cancer Institute- Antoni van Leeuwenhoek Hospital (NKI-AVL). In this study we describe our experience with the introduction of digital questionnaires in daily practice and study factors that affect the response rate.
The objective of this study was to investigate what the response rate was to digital questionnaires and which factors predict the response to the web-based and paper-based questionnaire. The main goal was divided in three specific research questions: 1. 'Do patients who always completed the questionnaires (web-based and paper-based) differ from patients who did not respond to at least one questionnaire?' 2. 'Do patients who completed the digital questionnaire differ from patients who completed the paper-based version?' 3. 'Do patients who completed the paper-based reminder differ from patients who did not complete the paper-based reminder?'
To our knowledge, no studies are available that have analyzed the routine use of web-based quality of life questionnaire followed by web-paper questionnaires for non-responders in daily practice in patients with prostate cancer.
Methods
The study design was an observational cohort study of patients who had localized prostate cancer and underwent a Robot Assisted Radical Prostatectomy (RARP) at our institute since November 2011. Before their first visit of the prostate cancer outpatient clinic all patients received a digital invitation to complete a Web-based Quality of Life questionnaire. Subsequently, 6 months, 1 and 2 years after the surgery, we mailed the same Web-based questionnaire. The questionnaires were sent through the website: https://www.levenskwaliteitprostaatkanker.nl. Before their first visit in our institute we asked all patients with prostate cancer to provide their email address. All patients with an email address received a digital personal coupon that referred them to the site "levenskwaliteitprostaatkanker.nl" (translated: quality of life prostate cancer.nl). The patients could subsequently fill-out the online questionnaire and send it back. The results were then uploaded into our local system for processing. The results were available at the time of the first outpatient consultation and were included in the anamnesis.
Study population
We mailed five validated questionnaires worldwide used in oncology to evaluate the quality of life and functional outcomes. Demographic and clinical characteristics such as age, height, weight, co-medication and comorbidity were obtained from the questionnaires. Urinary in continence was defined as any involuntary loss of urine. The degree of erectile nerve sparing was measured according to the Fascia Preservation Score [9]. A maximal score of 12 means a total preservation of the erectile nerves in the periprostatic fascia. A higher score correlates to more extensive periprostatic fascia preservation containing the neurovascular bundles driving erectile function. Biochemical recurrence after radical prostatectomy was defined according to the international consensus by two consecutive PSA values of >0.2ng/mL and rising [10]. Patients were excluded from analysis if: patients had no email address (n=6; 2%), or if patients could not understand the questionnaire (because they did not read and/or speak Dutch or were mentally incompetent).
Ethical committee
In 2008 the ethical committee approved the use of the validated quality of life questionnaires (QoLQ) for research. The patients in the study participated voluntarily and gave written consent prior to the study for obtaining the research material.
Data collection procedure
After sending the first digital questionnaire, we sent a digital reminder after 2 weeks to the non-responders. If we did not receive a response after 2 weeks, we sent the patients a paper-based questionnaire with a stamped return envelope.
Statistical analysis
The obtained items-scores in the questionnaires were transformed in domain-scores using standardized scaling manuals. The employment status was divided according to the CBS (Central Bureau statistics/ Central Office of Statistics) in 3 groups: low level of profession (fishermen, metal workers, janitors, construction workers, vendors or drivers), average level of profession (laboratory technicians, nurses, secretaries or accountants) and high level of profession (project managers, therapists, writers, journalists, physicians or economists). The cohort of patients was divided into the following groups: 1). Patients who always completed the questionnaires (web-based and paper-based) versus patients who did not complete it at least one time; 2) Patients who completed the digital questionnaire versus patients who completed the paper-based version; 3) Patients who completed the paper-based reminder versus patients who did not complete the paper-based reminder. Continuous characteristics of the groups were compared using analysis of variance (ANOVA), and categorical characteristics were compared using the Chi-square test. Next, to gain more insight into the strongest predictors of response, all factors found to be significantly associated with response in the univariate analyses were included in a multivariate logistic regression model. A p-value below 0.05 was considered as significant.
Results
Between January 2011 and April 2013, 297 patients were included in the study. All men underwent a RARP and had a follow up of more than one year and maximally two years.
In Table 1 the clinical and socio demographic characteristics of patients in the sample are shown. The mean age of the patients was 63 years (range 37-79 years). The patients were divided almost evenly between working (51%) and not working (48%) population. Most patients (39%) had an average employment status, 24% a low level and 19% a high level. The average distance between our institute and the patient's habitations (based on ZIP code) was 49 km (SD of range). Some patients (34%) returned to the referring hospital8 months after RARP.
The FP-score was lower in patients with postoperative erectile dysfunction (IIEF-EF< 20). Forty-nine percent (49%) of the patients had no erection after the RARP, 25% had an erection and 26% used medications or tools in order to get an erection. Biochemical recurrence was observed in 17% of patients (Table 1).
![]()
Table 1: Description of the study population (N=297)
View Table 1
A follow up of 1 year was available in all 291 men, while 64% (n=191) of the patients had a follow up of 2 years.
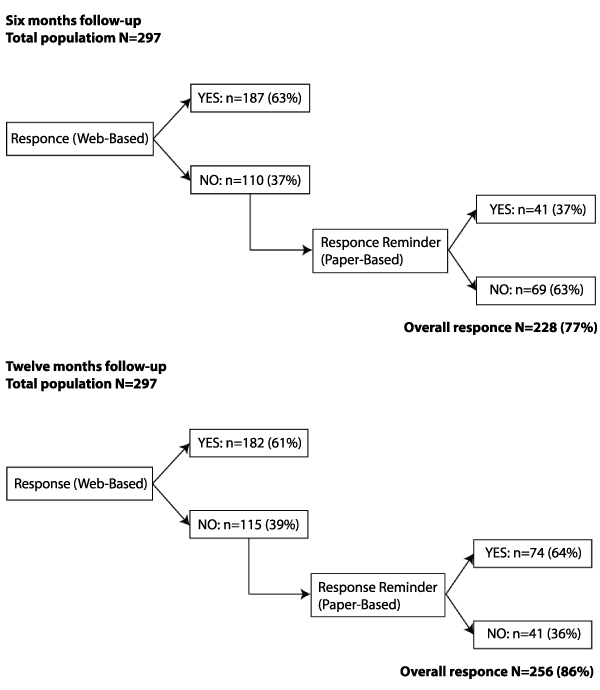
As shown in Figure 1, six months and one year after RARP, the overall response on both forms of questionnaires was respectively 77% (n=228) and 86% (n=256).
Two years after RARP, 59% (n=112) of the patients answered to the web-based questionnaire and 57% (n=45) of the non-responders (n=79) filled out the paper-based reminder questionnaire. The overall response rate was 82% (n=157).
We also studied the interval between the sending of the digital questionnaires and the response one year after RARP (n=182). The online questionnaires were always sent on a Friday. Most responses were within 3 days (Friday, Saturday and Sunday) on our site (53% N=92). During the week, except on Monday (21%), the response rate was low: Tuesday 7% (n=14), Wednesday 8% (n=17), Thursday 11% (n=20).
Do patients who always completed the questionnaires (web-based and paper-based) differ from patients who did not respond to at least one questionnaire?
As presented in table 2, a higher age was associated with a higher response rate (p< 0.05). Furthermore, patients who did not have professional activity also completed more often the questionnaires than those who were employed, but this difference was not statistically significant (p=.082). The response rate was not dependent on level of employment (p=.149). We noticed a better response on the questionnaires in patients without lymph node dissection or negative lymph nodes compared with patients with lymph nodes metastasis (p< 0.05). Postoperative functional problems such as urinary incontinence (p=.903), loss of urine drops (p=.544) or erectile dysfunction (p=.499) were not associated with response rate. However, there is a trend towards significance for a lower response rate after biochemical recurrence (p=.057).A multivariate analysis showed that age was the strongest predictor for answering to the web-based and paper-based questionnaires (p=.009). None of the other predictors included in the model (professional activity, pT status, pN status, FP-score, biochemical recurrence and functional outcome) were significantly related to the response rate in the multivariate analysis (Table 2).
![]()
Table 2: Differences between patients: Who did or did not complete the questionnaires (web-based and paper-based) in all intervals?
View Table 2
Do patients who completed the digital questionnaire differ from patients who completed the paper-based version?
Table 3 reveals the differences between digital responders and paper-based responders. Patients whose FP score was higher (more nerve sparing) answered the most through email (p< 0.05). Patients who had a biochemical recurrence frequently sent a response on the web-based questionnaire (p< 0.05). Patients with a higher pT status (p< 0.05), and lymph node metastases (p=0.097) answered mostly by the paper-based questionnaire. There was no association between type of questionnaire response and Gleason score (p=.307), post-operative urinary incontinence (p=.624), loss of drops (.170), erectile dysfunction (p=.333), or age (p=.407). In a multivariate analysis, none of the other predictors included in the model (age, professional activity, pT status, pN status, FP-score and biochemical recurrence) were significantly related to the response rate.
![]()
Table 3: Differences between patients who have completed the last questionnaire on paper and patients who have responded to the last questionnaire by email?
View Table 3
Do patients who completed the paper-based reminder differ from patient who did not complete the paper-based reminder?
At one year follow up 61% (n=182) of the patients (n=297) completed the web-based questionnaire (Table 4). We sent a reminder paper-based questionnaire to 115 digital non-responders. Sixty four percent (n=74) of them answered to the paper-based reminder questionnaire. Older patients sent a response more often than younger men (p< 0.05). Also patients who had less nerves spared as assessed by the FP score were more likely to respond to the paper-based questionnaire (p< 0.05) which correlates with the fact that patients who do not have an erection answered to the paper-based questionnaire reminder (p< 0.05). In a multivariate analysis, none of the other predictors included in the model (age, professional activity, pT status, pN status, FP-score, biochemical recurrence and functional outcome) were significantly related to the response rate (Table 4).
![]()
Table 4: Differences between patients who filled out the paper-based reminder questionnaire and the patients who did not fill out the paper-based reminder questionnaire at one year follow up?
View Table 4
Discussion
One of the issues of surveys or questionnaires is a low response rate that could lead to bias [11]. In the beginning of 2000 a low response rate was expected from the web-based questionnaires [11]. This ascertainment was seen in a literature research from the beginning 2000 [12] but since mid-2000, a higher response was observed in online surveys compared to other survey types [13] probably because of the rapid increase of internet access in the Netherlands. A response rate of 60% in surveys/questionnaires is usually required in order to decrease the risk of bias [14]. A response rate of minimal 60% is also important as a threshold for statistical significance at P< 0.05 [15]. In our study the response rate on only web-based quality of life questionnaires was around the 60% at all intervals which can be considered as a good response rate for statistical significance. However, this response rate on web-based questionnaires was not always observed in some other studies [16,17]. Mixed-mode survey designs (web-based and paper-based) can be used to increase the response rate [18].
Van der Berg et al. [8] showed that when participants have a choice between web-based questionnaire and paper-based questionnaire they more likely choose the paper-based questionnaire. However, the study of Smith et al. [19] showed that non-response is significantly higher in participants who choose the paper-based questionnaire. This seems to be a paradox but it could be possible that the gender of the population played an important role in both studies. In both studies the population was young/middle age, the only difference was the gender of the sample. In the study of van der Berg et al. [8], the study population was female and in the study of Smits et al. [19], male. Our study population included only male participants. We were convinced that men will respond to the web-based questionnaires and in order to reach the potential digital non-responders we choose for a reminder paper-based. We first sent a web-based quality of life questionnaire, followed after 2 weeks by a digital reminder and then again after 2 weeks we sent a reminder paper-based questionnaire to the digital non-responders. The response rate increased after sending the paper-based reminder from 61% to 86% and from 59% to 82% after respectively 12 and 24 months interval post-surgery. It seems to be a good way to improve the response rate [20]. The overall response rate before surgery was very high (98%). This can be explained as follows: all the patients who came to our hospital were referred from other hospitals for second opinion and/or treatment of prostate cancer. In order to prepare the first consultation, we always sent a questionnaire to all patients. These patients are very motivated to respond because they might think that it is important the specialist knows how their quality of life is for further treatment decision-making. Eight months after surgery we propose the patients to have their follow up visits at the referring hospital (to save traveling time for the patients) or general practitioner. There were no differences in response rates between the patients who had a follow up in our hospital and those that had follow up elsewhere. This is an interesting observation and suggests that questionnaires remain useful in settings where follow up is provided at various locations.
One of the advantages of web-based questionnaires is the fast response time [20] (within a few days). We always sent the online questionnaire on Friday because we were convinced that it would have a positive influence on the response rate. People would have perhaps more time in the weekend to answer. The response time of the online questionnaire was indeed fast: we had a response of 53% within 3 days. But we cannot say that the response rate is due to the emailing on Friday. Unfortunately, we could not compare the response time with the paper-based questionnaire because most of the patients did not fill out the date they completed the paper-based questionnaire.
Younger persons are usually more likely to respond to a web-based questionnaire [7]. The internet access in the elderly has been increasing in the Netherlands since the last years. Only 54% of people aged 65 and older had internet access in 2007 and in 2012 this was 81% [4]. The average age of our population group was 63 years old. We did not find that younger patients are more likely to respond to the online questionnaires. In contrast, older patients responded significantly more often what indicates that older patients are more faithfully responding than younger patients concerning the participation to the questionnaire.
We expected that patients with post-operative functional problems such as urinary incontinence and erectile dysfunction would be motivated to respond to the questionnaire in order to let us know about their concerns but we did not notice any significance in response between patients with or without complications. Whereas patients that underwent a more extensive nerve sparing during RARP were more likely to respond to the web-based questionnaire. The response on the paper-based reminder questionnaire was significantly higher in patients with a low erectile nerve sparing and in patients who had erectile dysfunction. It means that the paper-based reminder improved the generalizability of this study.
Surprisingly, patients who had postoperatively a higher tumor stage (>pT2) were more likely to respond to the paper-based questionnaire (p< 0.05) and patients who had a biochemical recurrence were more likely to respond to the web-based questionnaire (p< 0.05). It could be possible that patients with a higher pT stadium prefer to take time to fill out the questionnaires, prefer to think about every question before answering and paper questionnaires make it easier than digital. Patients who had a biochemical recurrence were usually referred to the radiotherapist for salvage radio therapy; it is possible that the patients wanted to send as soon as possible the response on questionnaires. The digital way is the quickest way. Patients who had postoperative no lymph node dissection and patients with no lymph node metastasis responded as well to the digital as paper-based questionnaire compared to patients with lymph node metastases (p< 0.05). It could be that patients who had lymph node metastases are more worried about oncological outcome of their disease and are less bothered by functional problems due to treatment and do tend not to fill out the questionnaires.
In a multi variable analysis only age remained a strong predictor for response to the questionnaires (web-based and paper-based). All the other factors (professional activity, pT status, pN status, FP-score, biochemical recurrence and functional outcome) were not statistically significant which mean that these factors were not independent.
Limitations
Several study limitations have to be mentioned. We do not know if some patients did not respond to the web-based questionnaire because they did not receive our email (due to spam filters, cookies, change of provider etc.) and we did not include this question in the paper-based questionnaire. This could have biased our findings.
Furthermore, we did not randomize patients to web-based and paper-based questionnaire.
The population of reminder paper-based responders versus non-responders was small (74 versus 41) therefore significance/non-significance in this group should be carefully interpreted.
Conclusion
To our knowledge there is no previous study that has explored the response of web-based and paper-based quality of life questionnaires in patients with prostate cancer in a sequential setting. The response rate was higher when a reminder paper-based questionnaire was sent to patients who did not respond to the web-based questionnaire (respectively from 61% and 59% to 86% and 82%, 12 and 24 months after prostatectomy). Furthermore, the elderly patients responded significantly more often than younger patients to both questionnaires (web-based or paper-based). Questionnaire based assessment of QOL is useful irrespective of location of oncological follow up.
References
-
Statistics from the CBS (Centraal Buro voor Statistiek), June 2012.
-
Dillman DA (2000) Mail and internet surveys. The tailored design method (1st edn): 352.
-
Archer TM(2013) Web-Based Survey. Journal of Extension 41: 4.
-
Van Deursen, AJAM, van Dijk JAGM (2012) Trendrapport Internetgebruik 2012, een Nederlands en Europees perspectief. Enschede, universiteit van Twente
-
van den Berg JP, Velthuis MJ, Gijsen BC, Lindeman E, van der Pol MA, et al. (2011) Guideline "Cancer rehabilitation". Ned Tijdschr Geneeskd 155: A4104.
-
IKNL (Integraal Kanker Centrum Nederlands), Bijlage F (2014) Deelrapportage voor prostaatkanker. Bijlage behorend bij het signaleringsrapport �Kwaliteit van Kankerzorg in Nederlands; voortgang en blik op de toekomst.
-
Klovning A, Sandvik H, Hunskaar S (2009) Web-based survey attracted age-biased sample with more severe illness than paper-based survey. J Clin Epidemiol 62: 1068-1074.
-
van den Berg MH, Overbeek A, van der Pal HJ, Versluys AB, Bresters D, et al. (2011) Using Web-Based and Paper-Based questionnaire for collecting Data on fertility issue among female childhood cancer survivor: difference in response characteristics. J Med Internet Res 13: e76.
-
van der Poel HG, de Blok W (2009) Role of extent of fascia preservation and erectile function after robot-assisted laparoscopic prostatectomy. Urology 73: 816-821.
-
Moul JW (2000) Prostate specific antigen only progression of prostate cancer. J Urol 163: 1632-1642.
-
Wyatt JC (2000) When to use web-based surveys. J Am Med Inform Assoc 7: 426-429.
-
Fricker RD, Schonlau M (2002) Advantage and Disadvantages of Internet Research Surveys: Evidence from the Literature. Field Methods 14: 347-367.
-
Evans JR, Mathur A (2005) The value of online surveys. Internet Research 15: 195-219.
-
Groves RM, Peytcheva E (2008) The impact of non-response rates on non-response bias: a meta-analysis. Public Opin Q 72: 167-189.
-
Livingston EH, Wislar JS (2012) Minimum response rates for survey research. Arch Surg 147: 110.
-
Villanueva NE, Thompson HJ, Macpherson BC, Meunier KE, Hilton E (2006) The neuroscience nursing 2005 role delineation study: implications for certification. J Neurosci Nurs 38: 403-408, 415.
-
Feudtner C, Santucci G, Feinstein JA, Snyder CR, Rourke MT, et al. (2007) Hopeful thinking and level of comfort regarding providing pediatric palliative care: a survey of hospital nurses. Pediatrics 119: e186-192.
-
Dillman DA, Smyth JD (2007) Design effects in the transition to web-based surveys. Am J Prev Med 32: S90-96.
-
Smith AB, King M, Butow P, Olver I (2013) A comparison of data quality and practicality of online versus postal questionnaires in a sample of testicular cancer survivors. Psychooncology 22: 233-237.
-
Kroth PJ, McPherson L, Leverence R, Pace W, Daniels E, et al. (2009) Combining web-based and mail surveys improves response rates: a PBRN study from PRIME Net. Ann Fam Med 7: 245-248.
